



Australians have been challenged in many ways over the past two years: some more than others
Welcome to the December issue of the MJA. It has not been a very jolly year, but I hope that reflecting on what has been and where we are (or should be) going is therapeutic. And I remain optimistic that, despite the challenges, the future is brighter.
Out of lockdown — for now
Overall, Australia has weathered the coronavirus disease 2019 (COVID‐19) pandemic remarkably well, thanks largely to the excellent public health response and our frontline health expertise, as well as the successful vaccination rollout, despite a stumbling start: the initial “it’s not a race” messaging crashed quickly.1 On 11 October 2021, New South Wales relaxed restrictions after a lockdown that had started in June following the escape of the Delta variant of SARS‐CoV‐2 into the community. For those fully vaccinated against the virus, this was a moment of widespread celebration across Greater Sydney and the state. The NSW double vaccination rate among people aged 16 years or more was well over 70% on this date, and 90% had received their first dose, a remarkable uptake. Not everyone celebrated, particularly frontline health care workers bracing for a possible surge in people requiring hospital care, despite the relatively high vaccination rates. While communities with lower rates, including regional and remote and First Nations communities, and workers in the disability sector urged that easing of restrictions be delayed until higher rates were achieved across the state, these pleas were largely ignored. Victorians also suffered as a result of the NSW outbreak, despite locking down early, ending aspirations of achieving “COVID‐zero”; Victoria also began loosening restrictions as vaccination rates increased, despite high case numbers. States that lived through 2021 in pleasant, largely COVID‐free bubbles, have been slow to open their local or international borders, instead watching and waiting. The roadmap out of lockdown in NSW was described by the state government and some experts as slow and cautious, but by others as too fast and rash. Relaxations were further accelerated by the new NSW premier.
The MJA has made major contributions to COVID‐19 policy debates throughout 2020 and 2021.2,3,4,5,6,7 What is clear from the published data and overseas experience is that high vaccination rates alone will probably not be enough, and other forms of public health measures should continue into 2022 if major surges in COVID‐19‐related hospitalisations and deaths are to be avoided.3,6 There is no biomedical magic bullet that will end the pandemic, despite what many political leaders might wish. As I write this piece in late October, it is unclear how the opening‐up experiment will work for communities and the hospital systems in NSW and Victoria. But I know this much: whatever the pressures, frontline medical and health professionals will continue to perform exceptionally. The MJA thanks you all for what you have done this year and will continue to do in the future.
Misinformation and vaccine hesitancy
The miracle of vaccination is undeniable. It is hard to believe that there is so much vaccine hesitancy and denial in the 21st century, despite the overwhelming evidence for its benefit and minimal risk.8 The deliberate attempts by a vocal minority to discourage vaccination during the COVID‐19 pandemic have been sobering; around the world, many unvaccinated people have died unnecessarily, and those responsible for spreading misinformation and propaganda have escaped scot‐free.9 Some of the vaccination‐hesitant are misinformed by people who should know better or are using the pandemic for personal gain. Others are deeply suspicious of authority, a sad consequence of the efforts of Big Tobacco and the fossil fuel industry to discredit genuine science for their own ends over decades (and often succeeding), leaving a bitter legacy of mistrust. Yet others are strongly influenced by the echo chambers of social media, arguably the dominant means of sharing news today (both real and fake news; but fake news is often much more entertaining). Some doubters do their own homework, but good research is difficult, and it is easy to misunderstand or be misled: this is why journals that expertly review and curate content remain so important. And it isn’t just vaccines. Misinformation and conspiracy theories about treatment have also permeated social media; too many people, for example, still believe in the benefit of ivermectin, despite all the evidence to the contrary, and aided and abetted by low quality publications, some of which have subsequently been withdrawn.10,11
The upside is that most Australians are pragmatic and have ignored the swirling nonsense; across Australia, more than 87% of people aged 16 years or more have received at least one dose of the COVID‐19 vaccine. However, the pandemic has exposed an underbelly of misunderstanding that only better education can redress. Reversing the defunding of higher education in Australia, despite the obvious value of Australian scientific and health expertise repeatedly evident during the COVID‐19 pandemic, must be a priority.12
The pandemic in 2022
Last year I talked in my annual Editorial of the “spring of hope”.13 I was perhaps premature. However, I remain optimistic that next year will be better, as echoed in an editorial in this issue by two prominent voices during the pandemic, Brett Sutton (the Chief Health Officer of Victoria) and Stephen Duckett (health program director at the Grattan Institute).14 The MJA will continue to publish high quality, evidence‐based perspectives, guidelines, and research articles in 2022 to help guide a smooth transition to the post‐recovery world.
Working from home
For much of 2021, the MJA team, like many people in NSW and Victoria, worked from home. The twice‐weekly MJA editorial committee meetings, where manuscripts are formally discussed before and after peer review, were seamlessly maintained as virtual meetings, as were the weekly issue planning meetings for reviewing all journal and Insight+ content. I am very proud of the efforts of the entire team during this difficult period, in which we continued to receive a high volume of submissions (Box 1).
A stronger Medical Journal of Australia
In 2021, the MJA worked hard to improve the journal for authors and readers. Let me touch on some of the highlights.
First, we moved to a fully online, print‐free model from 1 July, saving trees and reducing the carbon footprint of the MJA. The new online flipbook has been well received and will be further upgraded to improve the reader experience. We are also working on strengthening the MJA website for readers.
Second, the MJA has new procedures for reducing time to publication. For example, we have introduced a fast track publication process for selected peer‐reviewed, accepted articles we deem to be of particular urgency: we aim to publish these articles online within one week of scientific editing. Our detailed structural editing enhances article quality and is one of the advantages of publishing with the MJA. As the fast track option is resource‐intense, however, it must be limited in scope for the time being.
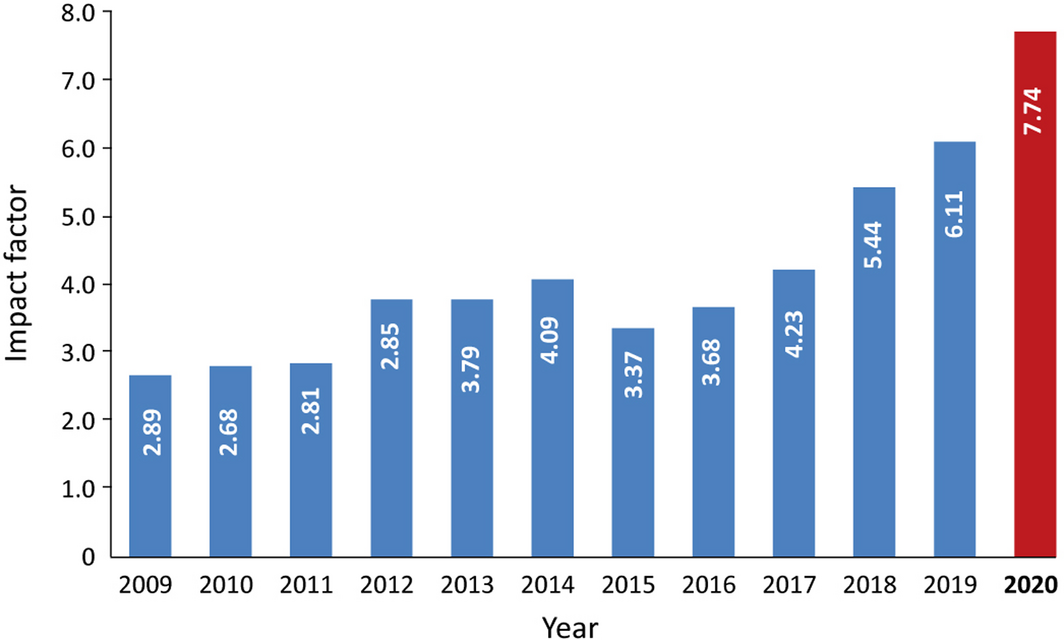
Third, although the ultimate aim of a medical journal is to improve health care, we are nonetheless very pleased that major bibliometric measures also reflect the continued growth in our impact. The MJA is recognised globally as a leading medical journal, and in 2020 our Journal Impact Factor (Clarivate Analytics) again increased, to 7.74 (Box 2). During the pandemic, the MJA has influenced policy by publishing new research findings, evidence‐based opinions, and authoritative guidelines for our international and growing readership and our strong subscriber base. All original research articles and publications on Indigenous health are available free of charge on our website (mja.com.au). Our partnership with Wiley has increased our global reach, and our climate countdown collaboration with The Lancet has made a strong impression.15
The future of preprints
In response to the public health emergency of COVID‐19, we have published peer‐reviewed manuscripts on the MJA website as preprints since early 2020,16,17 and this has been a remarkable success. MJA preprints are rigorously curated and are internally (and not infrequently externally) reviewed prior to publication. All but one of our preprints to date have subsequently been accepted for full publication as MJA articles after external peer review, testimony to the quality of the assessment process for our preprints. However, despite the rigorous process to which we subject them, preprints remain preliminary work and we do not currently assign them digital object identifiers (DOIs). Despite these limitations, preprints are here to stay in medicine and science. Even as the COVID‐19 pandemic begins to fade, we plan to continue using this option in a highly selective manner, and we look forward to further feedback from our readers.
Indigenous voices
The MJA recently published an important letter from Indigenous authors entitled “Who is speaking for us? Identifying Aboriginal and Torres Strait Islander scholarship in health research.”18 They argued compellingly that journals should “enhance the ability to efficiently distinguish Aboriginal and Torres Strait Islander scholarship, increasing the visibility of our knowledges and perspectives in research and translation, thereby improving the transparency of academic literature to guide decisions about our health and wellbeing.” In response to this letter, MJA authors may now include their Country in their article, and we look forward to further working with Indigenous people to advance the ideas they raised.
Reporting sex‐ and gender‐specific health data
Sex‐ and gender‐based differences matter in health, but have been underappreciated.19 In 2020, in an MJA perspective article entitled “Sex and gender in health research: updating policy to reflect evidence”,20 the authors presented the results of their mixed methods analysis (web search of policies and interviews with key informants) of policies on the collection, analysis, and reporting of sex‐ and gender‐specific health data by funding agencies and peer‐reviewed journals in Australia, including the MJA. Our policy is clearly articulated on our website: “The MJA follows the guidelines of the International Committee of Medical Journal Editors (ICMJE) and the World Association of Medical Editors on publishing and editorial matters, including peer review, conflict of interest and confidentiality.” The ICMJE guidelines state: “Because the relevance of such variables as age, sex, or ethnicity is not always known at the time of study design, researchers should aim for inclusion of representative populations into all study types and at a minimum provide descriptive data for these and other relevant demographic variables. Ensure correct use of the terms sex (when reporting biological factors) and gender (identity, psychosocial or cultural factors), and, unless inappropriate, report the sex and/or gender of study participants, the sex of animals or cells, and describe the methods used to determine sex and gender. If the study was done involving an exclusive population, for example in only one sex, authors should justify why, except in obvious cases (eg, prostate cancer).”21 We expect authors will continue to pay attention to these reporting guidelines; the editors certainly do. The MJA refers prospective authors to the Sex and Gender Equity in Research (SAGER) guidelines22 which we encourage authors to follow.
The publication process unmasked
For too many of our authors and readers, the process of assessing manuscripts for publication is a black box. At the MJA we apply rigorous standards, benchmarked against the leading journals in medicine, and each manuscript is individually considered on its merits. Most articles submitted to the top journals are rejected; the MJA is no exception, and the rejection rate for research manuscripts has exceeded 90% in recent years (Box 1). Although many open access journals do not require evidence of originality or impact, MJA authors need to convince the editors that their work is novel or important to the field (that is, will influence practice or policy), and will be read and cited. We first check whether a submitted manuscript conforms with our submission guidelines (https://www.mja.com.au/journal/mja‐instructions‐authors). It is then assigned to an experienced deputy medical editor, always endeavouring to ensure no conflict of interest arises, who may circulate it to other editors or bring it to an editors’ meeting for discussion. If the manuscript is deemed worth sending for review (including statistical and methodological review for research manuscripts), we contact several expert reviewers in order to find at least three who can assess it promptly. All peer review for the MJA is double blinded: reviewers do not know who the authors are until the article is published. The assigned editor then re‐reads the manuscript together with the reviewers’ comments, after which it is usually brought to an editors’ meeting (the “hanging committee”) for further review and discussion before making a decision of rejection, revision, or acceptance.
We rely on content reviewers to identify errors and limitations as well as strengths, but it is the editors alone, after weighing up all available information, who decide whether a manuscript is accepted. Acceptance without revision is very rare. More often, authors are asked to carefully address all comments by the editor and reviewers, recognising that their submission may still be rejected if the revision is unsatisfactory. If major changes are needed (eg, further experiments, addition of a control group, re‐analysis of the data), we will suggest that the authors undertake them if at all possible, but we do not recommend such changes lightly.
As the impact of the MJA has risen, we have received an increasing number of appeals to reconsider articles we have rejected. Authors need to present a compelling argument (and, often, more data) to be successful. Appeals are assigned to a different deputy medical editor, and are discussed at an editors’ meeting, but most rejection decisions are ultimately upheld.
After rigorous peer and editorial review, accepted manuscripts are expertly edited by our team of scientific and structural editors. Careful editing greatly improves research reporting quality,23 a key service for a medical journal, but one that few journals provide free of cost to authors.
Climate change
In an unprecedented move, more than 200 health and medical journals around the world, including the MJA, The Lancet, BMJ, and the New England Journal of Medicine, simultaneously published in 2021 an editorial calling for greater government action on climate change, to minimise global temperature increases and the hazards to health and nature that global warming brings.24 The MJA continues to publish on the science and health consequences of the climate emergency, including the annual MJA‒Lancet Countdown reports, to educate and inform doctors and other health professionals, and to influence policymakers.25,26,27 If current trends continue, the world will overshoot the target of restricting the temperature increase to 1.5°C above pre‐industrial levels.28 Not only do we need to reach net zero emissions soon, we must find ways to drive CO2 out of the atmosphere at scale. The health and societal outcomes of inadequate climate action are likely to be dire, as businesses now widely recognise, but powerful minority voices arguing against change remain loud in Australia. There has never been a more important time for doctors and other trusted health professionals to lead from the front.
The 2021 MJA Christmas competition
Laughter is therapeutic, I’m reasonably sure.29 Although we received fewer submissions for the annual Christmas competition than in previous years, perhaps reflecting what has been a very tough year for many, the quality was high. How would you manage atrial fibrillation in the merry but not so young Santa Claus? It’s not straightforward!30 Does garlic repel vampires, and what is the evidence?31 Are leftover chocolate Easter Bunnies re‐wrapped as Santa Clauses, as some believe (hint: it’s fake news!)?32 Can you practise suturing on a banana?33 And, on a more sobering note, how has the lockdown affected Victorians, according to one of our authors?34 These burning questions are all addressed in our competition this year. I’m pleased to announce that this year’s Christmas hamper will be travelling to the United Kingdom, to Mark Mills (The University of Sheffield) and David Warriner (Doncaster and Bassetlaw Hospitals NHS Foundation Trust).
Many thanks to our readers, subscribers, reviewers, and our Editorial Advisory Group
The MJA exists for our readers and authors, and we thank everyone for their support. It is prestigious to be published in the Journal, and we deeply appreciate the expertise of all the reviewers who have assisted the MJA team assess manuscripts rigorously and fairly (pp. 496–497). Finally, we thank all the members of our Editorial Advisory Group for their advice, input, and service during 2021. I wish you, dear reader, a very Merry Christmas and a Happy New Year on behalf of the entire MJA team!
Box 1 – Manuscripts received and accepted by the Medical Journal of Australia, 1 July 2020 – 30 June 2021, by type; number of peer reviewers, 31 October 2020 – 1 November 2021; and Journal Impact Factor (Clarivate), 2020
|
Manuscripts |
Accepted |
Received |
Proportion |
||||||||||||
|
|
|||||||||||||||
|
All manuscripts |
378 |
1836 |
21% |
||||||||||||
|
Research articles |
37 |
735 |
5% |
||||||||||||
|
Research letters |
26 |
137 |
19% |
||||||||||||
|
Narrative reviews/Meta‐analyses |
5 |
89 |
6% |
||||||||||||
|
Guidelines |
2 |
4 |
50% |
||||||||||||
|
Perspectives |
70 |
317 |
22% |
||||||||||||
|
Lessons from practice/Snapshots |
38 |
178 |
21% |
||||||||||||
|
Editorials |
47 |
47 |
100% |
||||||||||||
|
Letters |
105 |
142 |
74% |
||||||||||||
|
Mean time to decision (days) |
|
|
|
||||||||||||
|
All manuscripts |
Accept: 92; reject*: 33 |
||||||||||||||
|
Research manuscripts |
Accept: 152; reject*: 35 |
||||||||||||||
|
Peer reviewers (31 Oct 2020 – 1 Nov 2021) |
827 |
||||||||||||||
|
Journal Impact Factor, 2020† |
7.74 (2019: 6.11) |
||||||||||||||
|
|
|||||||||||||||
|
* With or without peer review. † Source: Journal Citation reports, Clarivate Analytics, October 2021. |
|||||||||||||||

I thank the tireless efforts of the editorial team throughout 2021, without which the quality and timely publication of our Journal would not be possible: deputy medical editors Alisha Dorrigan, Francis Geronimo, Robyn Godding, Tania Janusic, Wendy Morgan, Aajuli Shukla, and Elizabeth Zuccala; our scientific and structural editors, Paul Foley, Graeme Prince, and Laura Teruel; our consultant biostatistician, Elmer Villanueva; our news and online editor, Cate Swannell; our graphic designer, Leilani Widya; our head of publishing content, Ben Dawe; and our senior publishing coordinator, Kerrie Harding.
A complete list of disclosures is available at https://www.mja.com.au/journal/staff/editor‐chief‐professor‐nick‐talley