




This is a republished version of an article previously published in MJA Open
Medical workforce supply levels follow a predictable, if lengthy, cycle between phases of shortage and surplus. In Australia we are currently in an upswing stage; there has been significant growth in Australian medical workforce supply in the past decade. Between 1999 and 2009, there was an increase of over 20 000 employed medical practitioners — from around 50 000 to almost 73 000.1 Recent expansion of medical training programs does not largely account for this increase, as graduates of these programs only began entering the workforce in 2006, with the majority entering after 2008.2
The decreasing participation levels of doctors can be seen in a decline in average working hours. In 1999, Australian doctors worked 45.6 hours per week on average. By 2009, this had decreased to 42.2 hours per week.1 This translates to more than 6000 fewer full-time equivalent doctors than would be the case if average working hours in 2009 were the same as those a decade earlier. This decreasing work effort is attributable to an increased proportion of women in the medical workforce, a changing age profile, and changing work–life balance expectations.
Women comprised 36% of the medical workforce in 2009, up from 29% in 1999.1 Women account for only 19% of doctors aged 55 years and over (who as a group represent 25% of the total workforce), compared with almost 50% of doctors aged 35 years and under. The ratio of women to men in the medical workforce is likely to eventually reach 1 : 1, but currently, significant disparities between subgroups remain. While women comprise 39% of the general practice workforce, they comprise only 25% of the specialist workforce. Female doctors, on average, work fewer hours than male doctors (37.5 hours per week compared with 44.9); however, sex differences are less apparent for younger doctors. Female doctors under the age of 35 years work only 2 hours per week less than male doctors. For those aged 25–34 years, the averages are about 44 hours per week (women) and 46 hours per week (men); and for those under the age of 25 years, the corresponding figures are about 46 and 48 hours per week, respectively.1
While the average age of members of the medical workforce did not change between 1998 and 2008, there was nevertheless a changed age distribution during this period. In 2008, there was a higher proportion of doctors aged 55–64 years than in 1998, and a lower proportion aged 35–44 years. This reflects a sizeable group of medical practitioners who entered the Australian medical workforce in the previous “boom” phase in the 1970s. The “demographic hump” created by this group has been steadily moving through the age range and is now approaching traditional retirement age. Doctors who remain in the workforce beyond 65 years of age work far fewer hours than younger doctors. Hence, the coming years will see a considerable number of doctors either retiring altogether or reducing their working hours as they approach retirement. Retirement trends are a major influence on overall workforce supply levels,3 but there is relatively little information currently available on actual retirement patterns. Studies of retirement intentions suggest that one-third of general practitioners plan to retire before turning 65, and that job satisfaction is a key factor in this decision.4 Recent changes to registration arrangements, implemented as part of the move to the national registration scheme, made it more difficult for doctors to “step down” their clinical practice, by removing categories of registration that allowed some continued clinical practice without the requirements of full registration in relation to professional development and indemnity insurance.5 Proposals to remedy this, to ensure that a stepped approach is still a viable option for doctors, were the subject of a campaign driven by the profession.6
Work–life balance issues are increasingly prominent in the minds of doctors of all ages but have been particularly noted among younger doctors.7,8 Hospital non-specialists (a group largely comprising doctors in their early postgraduate years) overall worked fewer hours per week in 2009 than a decade earlier.1 Male hospital non-specialists have reduced their working hours while women have actually marginally increased theirs, so that the difference between the two sexes is now less than before.1 Overall, male doctors have made greater reductions than females to their working hours over the last decade, thus reducing the overall gender gap.1 Choice of specialty is influenced by the perceived work–life balance afforded by a specialty,9,10 and by hours of work and the possibility of time out from the medical workforce.
The early postgraduate years are a critical time for doctors, when job demands are likely to be high and when many are making decisions about which specialty they wish to practise in for the rest of their working lives.7,10
Since 2000, graduate numbers have doubled; from around 1400 a year to 2733 in 2010. They are projected to increase further, to reach almost 4000 in 2016.11 The number of intern places has been slightly higher (by 5%–10%) than the number of graduates the previous year (Box 1), partly because of New Zealand graduates and other international medical graduates coming into the system (via the Australian Medical Council pathway). The figure also indicates how this gap closed in 2009 and 2010. On the basis of projected numbers of Australian medical graduates, we can anticipate that intern places will need to increase by over 1000 in the next 5 years. Difficulties are already being experienced in attaining sufficient settings and supervisors,12 and these seem likely to continue, or worsen, in the next few years. A broader and more flexible approach to internships is likely to be required to accommodate the growing numbers (eg, incorporating private sector and primary care settings as well as traditional large public hospitals). Achieving this successfully will require cross-sectoral collaboration to ensure comparability of training experiences and appropriate resourcing across settings.13
However, data are available on the number of basic, advanced and total trainees (Box 2). These data indicate relatively little change between 2000 and 2003, followed by significant growth in overall trainee numbers since 2004. Advanced trainee numbers increased 80% between 2001 and 2011, with most of the increase occurring since 2005. Increases have been somewhat uneven across specialties during this period (Box 3). A number of specialties more than doubled their number of trainees, and all clinical patient-care specialties have had some growth. Five new training programs were in operation in 2011 that did not exist a decade earlier. The largest absolute increases in trainee numbers were in general practice (increase of 1429) and adult medicine (increase of 1029). As with internships, a more diverse array of training arrangements is likely to be required for vocational training, with concomitant challenges in maintaining equivalence.
Policy debates are already starting to come full circle, with concerns now being raised about potential oversupply in the medical workforce.14 This mirrors the pattern seen in previous decades, with the 1970s boom (in response to perceived shortages) followed by perceived surpluses through the 1980s and 1990s, which in turn influenced restrictive policies on entry to the medical workforce. To some extent, such swings in perception may be inevitable. To avoid the extremes, it is important to maintain a proactive approach to workforce policy that is informed by good evidence and takes into account both macro-level total supply trends and issues in specific sectors or specialties. For example, workforce supply in non-metropolitan areas remains below levels in major cities.15 Shortages are also apparent in specialties, including orthopaedic surgery, ear, nose and throat surgery, obstetrics, pathology, radiology, oncology, psychiatry and general medicine.16,17 Within the primary care sector, specific services are problematic, such as after-hours services, home visits, and procedural GP services in rural areas. Current programs have invested significant funds to try to redress the shortage of after-hours services and procedural rural GPs, but significant problems remain.18
Ensuring an adequate workforce in the primary health care sector and rural regions.
Developing and maintaining capacity to identify and respond to ongoing and emerging health workforce policy challenges.
Accommodating diverse patterns of workforce participation.
While the increases already seen in the general practice pipeline are encouraging, additional strategies for increasing participation include promotion of the attractions of general practice as a specialty, including the potential for good work–life balance, flexibility in the training program, and high job satisfaction.19 Exposure during training to positive experiences of general practice may promote uptake of GP careers among medical graduates. Given the importance of relative pay rates for doctors in their choice of specialty,20 increasing GP pay is another potential strategy to support recruitment. However, non-financial incentives (such as controllable hours, flexibility and opportunities for “interesting” work) are also important.20
The changed expectations and preferences of doctors with regard to working hours and participation will need to be matched by a range of strategies to accommodate such preferences, to prevent even greater losses of work effort over the career span. This may include more flexible leave and part-time arrangements in employment and training, as well as facilitation of re-entry to the medical workforce. It has been suggested that doctors approaching retirement could be engaged in medical education,21 a strategy which has the potential to retain older doctors and increase their job satisfaction, while also meeting the educational needs of younger doctors. Significant gaps remain in an understanding of factors influencing doctors’ choices about workforce participation during the late career, pre-retirement stage. Such information is of crucial importance in maintaining the attachment of these doctors to the workforce.
Innovative care models are likely to be required to meet demand for after-hours care. Many new approaches are already in place, such as call centres and help lines, GP clinics co-located with emergency departments, nurse triage services and so on. Such strategies should be expanded and further developed. Many of these alternatives incorporate an element of skill-mix changes, and further innovation in scope of practice for non-medical health professionals (including new roles such as physician assistants and nurse practitioners) has the potential to significantly alter future medical workforce requirements.22
1 Numbers of Australian medical graduates (domestic and total), and number of intern places*
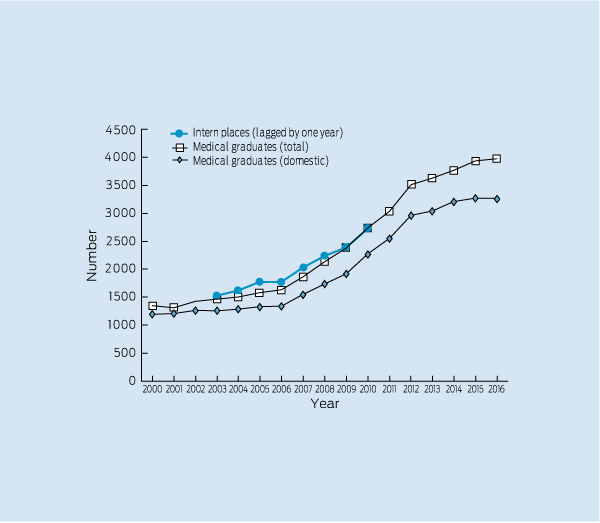
* Actual numbers shown up to 2010, and projected numbers of graduates for 2011–2016.11 Numbers of intern places are shown lagged by 1 year to display the relationship to the number of graduates in the previous year (eg, data shown for internships for 2003 is number of internships in 2004, which are largely taken up by 2003 graduates).
2 Vocational trainees: basic, advanced and total trainee numbers, 2000–2011*11
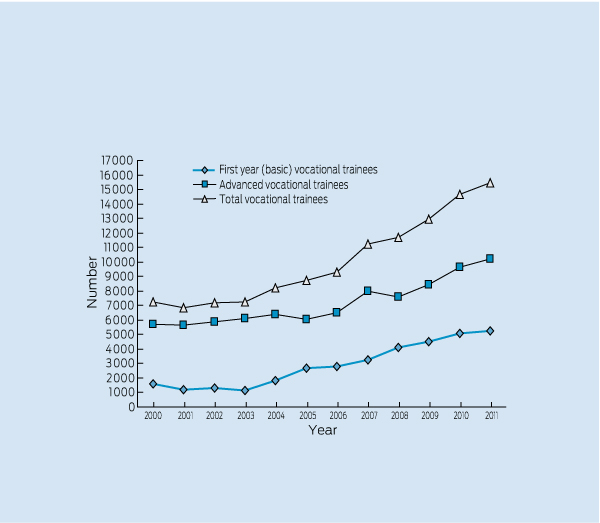
* Some colleges report number of trainees while others report number of accredited positions.
Provenance: Commissioned; externally peer reviewed.
- Catherine M Joyce1
- School of Public Health and Preventive Medicine, Monash University, Melbourne, VIC.
No relevant disclosures.
- 1. Australian Institute of Health and Welfare. Medical labour force 2009. Canberra: AIHW, 2011. (AIHW Cat. No. AUS 138; AIHW Bulletin No. 89.) http://www.aihw.gov.au/publication-detail/?id=10737419680 (accessed May 2012).
- 2. Joyce CM, Stoelwinder JU, McNeil JJ, Piterman L. Riding the wave: current and emerging trends in graduates from Australian university medical schools. Med J Aust 2007; 186: 309-312. <MJA full text>
- 3. Joyce CM, McNeil JJ, Stoelwinder JU. More doctors, but not enough: Australian medical workforce supply 2001–2012. Med J Aust 2006; 184: 441-446. <MJA full text>
- 4. Brett TD, Arnold-Reed DE, Hince DA, et al. Retirement intentions of general practitioners aged 45–65 years. Med J Aust 2009; 191: 75-77. <MJA full text>
- 5. Senate Finance and Public Administration References Committee. The administration of health practitioner registration by the Australian Health Practitioner Regulation Agency (AHPRA). Canberra: Commonwealth of Australia, 2011. http://www.aph.gov.au/Parliamentary_Business/Committees/Senate_Committees?url=fapa_ctte/health_practitioner_registration/report/index.htm (accessed May 2012).
- 6. Australian Doctors’ Fund. Proposal for senior active doctors. April 2011. http://www.adf.com.au/archive.php?doc_id=181 (accessed Oct 2011).
- 7. Markwell AL, Wainer Z. The health and wellbeing of junior doctors: insights from a national survey. Med J Aust 2009; 191: 441-444. <MJA full text>
- 8. Shrestha D, Joyce CM. Aspects of work-life balance of Australian general practitioners: determinants and possible consequences. Aust J Prim Health 2011; 17: 40-47.
- 9. Dorsey ER, Jarjoura D, Rutecki GW. The influence of controllable lifestyle and sex on the specialty choices of graduating US medical students, 1996-2003. Acad Med 2005; 80: 791-796.
- 10. Brett TD, Arnold-Reed DE, Phan CT, et al. Work intentions and opinions of general practice registrars [letter]. Med J Aust 2009; 191: 73-74. <MJA full text>
- 11. Medical Training Review Panel. Fifteenth report. Canberra: Commonwealth of Australia, 2012. http://www.health.gov.au/internet/main/publishing.nsf/Content/work-pubs-mtrp-15 (accessed May 2012).
- 12. Crotty BJ, Brown T. An urgent challenge: new training opportunities for junior medical officers. Med J Aust 2007; 186 (7 Suppl): S25-S27.
- 13. Fox GJ, Arnold SJ. The rising tide of medical graduates: how will postgraduate training be affected? Med J Aust 2008; 189: 515-518. <MJA full text>
- 14. Birrell B. Australia’s new health crisis — too many doctors. Melbourne: Centre for Population and Urban Research, Monash University, 2011. http://arts.monash.edu.au/cpur/--downloads/australias-new-health-crisis.pdf (accessed May 2012).
- 15. Australian Government Department of Health and Ageing. Report on the audit of health workforce in rural and regional Australia, April 2008. Canberra: Commonwealth of Australia, 2008. http://www.health.gov. au/internet/main/publishing.nsf/Content/work-res-ruraud (accessed May 2012).
- 16. National Health Workforce Taskforce. Health workforce in Australia and factors for current shortages, April 2009. Sydney: KPMG, 2009. http://www.ahwo.gov.au/documents/NHWT/The%20health%20 workforce%20in%20Australia%20and%20factors%20influencing% 20current%20shortages.pdf (accessed May 2012).
- 17. Australian Health Ministers’ Conference. National health workforce strategic framework. Sydney: AHMC, 2004. http://www.ahwo.gov.au/documents/Publications/2004/National%20Health%20Workforce% 20-%20Strategic%20Framework.pdf (accessed May 2012).
- 18. Rural Workforce Agency of Victoria. Future of the GP procedural workforce. Melbourne: RWAV, 2010.
- 19. Joyce CM, Schurer S, Scott A, et al. Australian doctors’ satisfaction with their work: results from the MABEL longitudinal survey of doctors. Med J Aust 2011; 194: 30-33. <MJA full text>
- 20. Sivey P, Scott A, Witt J, et al. Why junior doctors don’t want to become general practitioners: a discrete choice experiment from the MABEL longitudinal study of doctors. Working paper no. 17/10. Melbourne: Melbourne Institute of Applied Economic and Social Research, 2010.
- 21. Joyce CM, Piterman L, Wesselingh SL. The widening gap between clinical, teaching and research work. Med J Aust 2009; 191: 169-172. <MJA full text>
- 22. Harris MF, Zwar NA, Walker CF, Knight SM. Strategic approaches to the development of Australia’s future primary care workforce. Med J Aust 2011; 194 (11 Suppl): S88-S91. <MJA full text>
Summary
Key trends in Australian medical workforce supply include increasing overall supply levels and an increasing number of medical graduates, but also reduced workforce effort and a large cohort of doctors approaching traditional retirement age.
Although prevocational and vocational training programs are beginning to expand, there are significant bottlenecks in the postgraduate training pathway for the sizeable cohorts of new graduates.
The primary health care workforce needs continued development, including team-based approaches to care and increased use of technology.
Increasing our understanding of system-level and individual-level determinants of doctors’ choices and implementing innovative strategies to accommodate the increasingly diverse work patterns of doctors are critical to ensuring that in future there are sufficient doctors, with the right skills, in the right places.