





Volume 187 - Issue 11
Sharing the secrets of success: conversations with the Medical Journal of Australia / Wyeth Research Award winners, 1995–2006
Authors: Ann T Gregory, Ruth M Armstrong, Tanya D Grassi and Martin B Van Der Weyden
Med J Aust 2007; 187 (11): 637-644. || doi: 10.5694/j.1326-5377.2007.tb01455.x
Published online: 3 December 2007
Published online: 3 December 2007
Have you ever wondered what makes a good research paper? Since 1995, the best original research paper published each year in the Medical Journal of Australia (MJA), as judged by the Journal’s Content Review Committee, has been awarded the MJA/Wyeth Research Award. To date, 12 papers have won the award ($10 000 and a commemorative trophy), representing a diverse range of research methodologies, practice settings, professional disciplines, and subsequent citation rates (Box 1).
We recently interviewed key researchers associated with this distinguished dozen, inviting them to tell us the behind-the-scenes stories of their papers and the impact their work has had since publication. In the course of our discussions, we heard 12 very different but often strikingly similar stories — stories of curiosity, innovation, purpose, determination and teamwork, as well as some significant concerns about the future of medical research in Australia.
1995: Gastric emptying is not needed after acute oral overdose in adults
As you administered a particularly unpleasant medical intervention, have you ever wondered whether it was really necessary? Susan Pond, an Australian medical graduate, found herself working in the United States as a Fellow in Clinical Pharmacology at San Francisco General Hospital in the 1970s. Following on from the Haight-Ashbury hippie days of the previous decade, drug overdose was a major problem in the city.
At that time, the treatment of overdose was quite empirical, and Pond set about collecting evidence for the ways in which charcoal could be used to remove poisons. Adapting the well known tradition of self-experimentation, Pond co-opted a couple of her six children to test out “easy” formulations of activated charcoal (Box 2).
“One of them was game enough to swallow this awful black stuff, and he threw up within minutes ... the mess was just terrible”, Pond said.
Referring to standard treatment, she added: “Not only were we making overdose patients vomit with ipecac, but we were also giving them activated charcoal, after which they promptly vomited again. It seemed to me to be very pointless”.
Pond returned to Australia in the 1980s, where the opportunity arose, at Princess Alexandra Hospital in Brisbane, to challenge the long-established routine care for poisoning through a prospective, randomised controlled trial, comparing activated charcoal with a combination regimen of gastric emptying plus charcoal. In designing the study, Pond spent a long time talking with an American toxicologist, Ken Kulig, who had reported that acutely poisoned patients could be effectively treated without gastric emptying. Pond wanted to build on Kulig’s earlier research but without running into the same pitfalls: insufficient patient numbers and allocation bias.1
The Australian trial involved 876 eligible patients who presented to the emergency department at Princess Alexandra Hospital between January 1988 and June 1990. No significant differences were detected between the two treatment arms, and Pond and colleagues concluded that gastric emptying could be omitted from the treatment regimen for adults after acute oral overdose.
Published in the MJA in October 1995, it did not take long for the study results to filter through to clinical practice — in 1997, the American Academy of Clinical Toxicology issued a position statement on ipecac syrup, which concluded that gastric emptying by ipecac should not be administered routinely in the management of poisoned patients.2
“The field was ready for a big study and it [our study] served to crystallise the thinking”, Pond said. “Very rapidly, the issue became whether or not charcoal needed to be administered, and the field moved on quite rapidly to suggest that even that’s not necessary in many cases of poisoning.”
In 1997, Pond joined Johnson & Johnson Research Pty Ltd in Sydney to pursue the application of the genomics revolution to therapeutics. Her current research involves discovery and development of RNA and DNA molecules that regulate gene function and expression. The most advanced product, currently in clinical trial, is an anti-HIV RNA molecule inserted into bone marrow stem cells of patients infected with HIV.
1996: A public health investigation detects Japanese encephalitis virus in Australia
How would you go about investigating the mysterious deaths of two members of a small island community? When such a tragedy occurred on the outer Torres Strait island of Badu in March–April 1995, the residents welcomed a wide range of investigators from the Australian mainland, led by public health physician Jeffrey Hanna.
Scott Ritchie, medical entomologist on the project, told us that Murray Valley encephalitis was initially thought to be the most likely culprit but, before long, virological studies on samples from the encephalitis cases, and serological surveys of other asymptomatic residents revealed evidence of Japanese encephalitis (JE) virus infection. The researchers found themselves investigating an outbreak of a virus that had never been found in Australia before — a classic, emerging, infectious disease.
Ritchie said the various teams — medical, public health, entomological, veterinary, and laboratory — worked away for days at a time, applying known “shoe-leather” epidemiological methods to get the information they needed. When not working, they watched late-night test cricket and slept on mattresses at the health centre. The whole investigation took about a month.
In addition to infection in the residents, the investigators also identified recent JE virus infection among domestic pigs (one of the viral hosts) on the outer islands of the Torres Strait. Virus isolations and mosquito surveys on Badu Island implicated the mosquito Culex annulirostris as the major vector in the outbreak.
The researchers speculated that migratory birds and/or windblown mosquitoes had imported the virus into the Torres Strait, possibly from Papua New Guinea, and that a combination of environmental factors — including large numbers of domestic pigs kept in “wet” pigpens close to human dwellings and mosquito-breeding sites (Box 3) — had facilitated the outbreak.
“It fit the pattern of JE virus overseas. In South-East Asia, you have rice paddies and people with pigpens in the backyard. In the Torres Strait, it’s quite low and swampy, and pigs are abundant”, Ritchie said.
Ritchie is certain that lives were saved as a result of the public health response to this research. After the Badu Island outbreak, an inactivated JE vaccine was offered to the inhabitants of the outer Torres Strait islands. On Badu Island, pigs were moved from backyards to a piggery out of town, and swamps were drained.
“JE virus is now detected nearly every summer in sentinel pigs on Badu Island, but there haven’t been any other human cases since a second outbreak in 1998. If we hadn’t vaccinated, I think we would have definitely seen more human cases”, Ritchie said.
Hanna and colleagues have continued to publish papers on disease outbreaks, including the 1998 JE outbreak and the Noah Beach malaria outbreak in Far North Queensland;3,4 the cross-agency collaboration continues to this day.
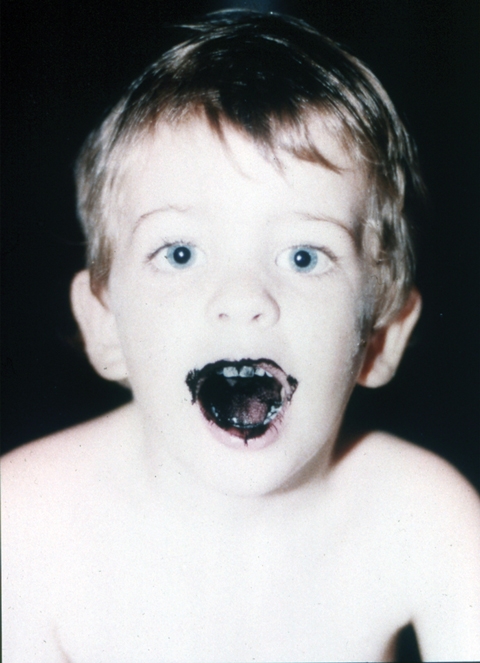
1997: Photographic surveillance can effectively detect melanoma in patients with multiple dysplastic naevi
How you would respond if you were questioned about your everyday clinical practice because it was different from that of your peers? In the 1980s, when Melbourne dermatologist John Kelly was asked why he was using total body photographic surveillance to follow a group of melanoma-prone patients with multiple dysplastic naevi (MDN), instead of undertaking the then widely used practice of prophylactic excision, he decided to conduct a study to determine the value, including cost-effectiveness, of his approach.
Several years earlier, while working in a melanoma clinic in San Francisco, Kelly had been involved in a case–control study that found that MDN were a strong and independent risk factor for the development of melanoma.5 “It seemed logical that if these people were most at risk for melanoma, then they were the people to put into a follow-up program to find the melanoma in the future”, Kelly said.
But what if the case–control study had been flawed? He wanted to reassure himself as well as others. Kelly enlisted the assistance of several colleagues and his sister-in-law (a clinical photographer) and followed a high-risk cohort of 278 patients with MDN, using photographic surveillance, for an average of 42 months. All the patients had presented at his private dermatological practice between March 1985 and November 1992.
Over the course of the study, 20 new melanomas were detected in 16 patients, corresponding to an age-adjusted incidence of melanoma in these patients that was 46 times that of the general population.
“The use of the photographs enabled earlier diagnosis because we were able to detect new and changed lesions that were early melanomas but that were not yet showing typical clinical features. The median tumour thickness was much lower than for tumours reported to the State Cancer Registry at the time”, Kelly said. Further, more than 60% of the melanomas were de-novo, rather than arising from dysplastic naevi, suggesting that prophylactic excision of dysplastic naevi was not a satisfactory alternative to follow-up.
This study, along with others, helped to confirm the very high rates of melanoma in patients with dysplastic naevi and to “guide guidelines” for the use of total body photography, said Kelly.
With others, Kelly has conducted further research along similar lines with a new cohort of patients, confirming the previous findings and showing that a new or changed pigmented lesion is more likely to be a melanoma in patients older, rather than younger, than 50 years of age.6
Internationally, photographic surveillance is now the standard practice in managing people with MDN.
1998: Outdoor air pollution is linked to night-time cough and chest colds in children
How would you go about assessing the effects of the environment on child health in an industrial city? Ongoing community concern about a possible link between childhood asthma and air pollution in the steel cities of New South Wales — Newcastle and Wollongong — helped Peter Lewis and Michael Hensley and their colleagues achieve high participation rates in their 1993 cross-sectional survey of children’s respiratory symptoms and home environment.
The existing body of work had been done primarily in the US and Europe, but there were some significant differences in aspects of air quality and air-quality basins in Australia. “We had some lower levels of pollution, in particular, particulate pollution”, said Hensley.
The researchers consulted widely and often with the community. They surveyed primary school children living in suburbs close to the steelworks, as well as children from surrounding suburbs further away, who acted as “normals” exposed to “background” levels of pollution. The study found that particulate pollution was associated with respiratory symptoms such as head cold and coughs but not with asthma. They also found that the effects on health were seen at lower levels of particulate pollution than had previously been thought.
In 1999, the Newcastle steelworks closed, principally for economic reasons, said Lewis. “However, this paper was one of several studies that contributed to how air quality guidelines should be set in Australia”, he said. “It certainly strengthened the case that the levels of air pollution we were experiencing are not without their potential side effects.”
Hensley, with co-researchers, has gone on to publish related papers about indoor air quality, including the effects of environmental tobacco smoke and bronchial reactivity among children,7,8 and is now Dean of Medicine at the University of Newcastle.
Lewis has taken his environmental epidemiological research approach to public health work on the Central Coast of NSW and is now involved with measuring the impact on health of such diverse entities as bushfires, fluoridation of the water supply, and retirement village living.
1999: Comprehensive screening and treatment program reduces prevalence of STIs in remote Aboriginal communities
Who do you think has made a contribution to the control of sexually transmitted infections (STIs) in Aboriginal Australia that is greater than the sum of everyone else’s? For this accolade, Paul Torzillo would not hesitate to pick Penny Miller, a primary care doctor who created a program in the mid 1990s that aimed to improve access to and delivery of STI services in remote Aboriginal communities on the expansive Anangu Pitjantjatjara (AP) Lands in the far north-west of South Australia, with a view to reducing transmission not only of STIs but also HIV.
“At the time, it was widely touted that community-wide STI screening would be virtually impossible, let alone unethical, because the Aboriginal communities would not want it; and, if it did occur, it would be ineffective”, Torzillo said.
But the Aboriginal communities did want it. Nganampa Health Council is the independent, Aboriginal-controlled health service that provides primary health care to nearly 3000 Aboriginal people living on the AP Lands. The Council’s Aboriginal board of management, which is also the ethics committee, approved Miller’s project. Annual community-wide screening for syphilis was already well established in the AP Lands, and community participation in the new program was voluntary and high.
Miller’s community-based program took full advantage of technological advances in screening for gonorrhoea and chlamydial infections, with urine polymerase chain reaction tests replacing diagnosis by urethral swab in men and by vaginal and cervical swabs in women. The urine testing made mass screening both more acceptable and more feasible. The program also involved more than a dozen further interventions, including presumptive treatment (before diagnosis was confirmed by pathology results), single-dose rather than multidose therapy, and reporting back to the community.
The program was effective. Coauthored with Torzillo and Wayne Hateley, an Aboriginal health worker who until recently lived and worked in the communities, Miller’s paper reported that, in the short period of 2 years, the prevalence of gonorrhoea in people aged 12–40 years was significantly reduced — in fact, almost halved — from 14.3% in 1996 to 7.7% in 1998. The service also achieved reductions in chlamydia and syphilis.
The paper weakened a general resistance at the time to applying public health principles to Aboriginal health. “In retrospect, the resistance was clearly because inadequate screening and treatment isn’t effective, but comprehensive screening and treatment can be”, Torzillo said.
Miller now works in the field of international HIV research. Torzillo continues to work for the Nganampa Health Council, as he has done since it was first established in 1983. He also maintains an appointment as a respiratory and intensive care consultant at Sydney’s Royal Prince Alfred Hospital.
Today, aggressive public health approaches to STIs are considered the “norm” in Aboriginal communities. On the AP Lands, this program and others, like women’s health and child immunisation programs, continue to operate. New STI program initiatives continue to emerge, like Ushma Scales’ song about condom use, Take your shield to town, with lyrics in Pitjantjatjara.9
2000: Systematic chronic disease treatment program reduces rates of renal failure and death in Aboriginal communities
What would you do if your research revealed a whole community with untreated early disease whose progression could be slowed by a simple intervention? When working in New Mexico in the US, Wendy Hoy, with co-researchers, demonstrated that end-stage renal disease was a significant problem in Native American tribes. On her return to Australia, she investigated a burgeoning epidemic of renal failure in Aboriginal people in the Northern Territory and found probably the world’s highest recorded rates of renal failure in the communities of the Tiwi Islands, north of Darwin.
There was also a great reservoir of early disease, including hypertension and albuminuria. Hoy said: “I knew from existing literature that the progression of renal disease could be reduced by treatment with angiotensin-converting enzyme inhibitors. This treatment needed to be widely applied in the Tiwi community, but the health services were very scantily resourced at that time and couldn’t do it”.
Another barrier was a prevailing attitude that if you gave Aboriginal people a pill, they wouldn’t take it; and that if they did take it, it wouldn’t have an effect because their biology was different.
“You’ve got people with a deadly disease for which treatment guidelines are out there in the international literature, with known very beneficial outcomes. It would have been wrong to allow it to go unattended”, Hoy said.
So the research team delivered a service offshoot that was embraced by the community — a systematic chronic disease treatment program to modify renal and cardiovascular disease, involving antihypertensive agents to achieve blood pressure goals and attempts to improve the control of blood glucose and lipid levels. After 2 years of treatment, Hoy and colleagues were able to report a rapid, dramatic improvement in clinical profiles and a fall in death rates.
Their paper declared: “These results show that Aboriginal people are interested in health issues and receptive to health messages, and will take medications over the long term to protect against future health risk, with excellent response”.
Over the past decade, there has been increasing acceptance and practice of the principles of chronic disease surveillance and rigorous management in Aboriginal communities.
“Endorsement, intellectually, of chronic preventable disease strategies is no longer the issue; now, it’s resources and staffing to execute them in remote areas where the people have disastrous disease profiles”, said Hoy. After handover of the treatment program to the local health board in the Tiwi Islands, the intensity of the program declined and compliance with medicines use fell for a time, due to inadequate resources.10
However, Hoy is optimistic about the future of Indigenous health. “The spotlight on Aboriginal health here is becoming brighter, and dialogue encouraging government to be, one, more receptive; and, two, more accountable in terms of delivering good services is only going to intensify.”
2001: Quality improvement project reduces inhospital deaths in patients with acute myocardial infarction
How would you respond to the suggestion that patients hospitalised with acute myocardial infarction (AMI) at your hospital might have a higher mortality rate than similar patients at peer hospitals? In the mid 1990s, Ian Scott, then Director of Medicine at Queensland’s Ipswich Hospital, responded by initiating a quality improvement project that aimed to achieve, among other things, a reduced time to thrombolysis and an increased number of patients who were taking lipid-lowering agents when they left the hospital. He wrote local guidelines for coronary care practice, started an echocardiography service, and got together with the local Division of General Practice to set up a cardiac rehabilitation program, as well as providing sequential feedback to health care providers.
A before–after time-series study suggested that quality of care at the hospital did improve as a result of the project.11 This evidence was soon bolstered when hard outcomes data on inhospital deaths, from the Queensland Hospitals Admitted Patient Data Collection, came to Scott’s attention. Using this state-based data, Scott and colleagues were able to demonstrate a significant reduction in the mortality rate for AMI at Ipswich Hospital, from 12.5% in 1994–1995 (pre-intervention) to 8.8% in 1996–1999 (post-intervention). The rates at a group of control hospitals in Queensland showed no significant change (remaining at about 12.8%) over the same period of time.
“The study has given a higher profile to quality improvement science by showing that we can improve and evaluate practice on a reasonable scientific footing, with real data to support what we are saying”, said Scott.
The quality improvement interventions have now been rolled out, with beneficial effects, across more Queensland hospitals.12 “I think it’s been a real success story. We’ve gone from a small community hospital to a collaborative of about 21 hospitals across the state, accounting for close to 80% of all AMI admissions.”
Now based at Brisbane’s Princess Alexandra Hospital, Scott has continued to pursue further quality improvements in relation to the management of AMI and heart failure. Recently, together with colleagues, he reported on “risk–treatment mismatching”, where much more treatment goes to lower- or moderate-risk patients than high-risk patients.13
2002: Serious doctor–patient and health care worker–patient miscommunication may be compromising Indigenous health outcomes
Have you ever struggled to communicate with a patient? What if the patient didn’t speak much English — what would you do? Working in Darwin with Indigenous patients who had kidney disease, Alan Cass and colleagues found themselves operating across what seemed to be a significant cultural and, often, linguistic divide. At the same time, people working as linguists and community researchers in Arnhem Land were also becoming aware that, despite everyone’s best intentions, there were communication problems they didn’t understand.
“It was a somewhat fortuitous coming together of people from very different backgrounds, including some of the patients themselves, who wanted to think about how we could work together in undertaking some cross-cultural research to try to understand the issues”, Cass said.
The group considered various possible methodologies before settling on the qualitative approach of participatory action research — using video to capture interactions, then analysing them to identify issues. They also conducted post-interaction interviews in the health care workers’ and patients’ first language to clarify what each person had understood to be communicated. In the setting of a satellite dialysis unit, where many of the carers were fairly well known to the patients and vice versa, the researchers videotaped five clinical interactions concerning diagnosis, treatment and management in diverse individual patients from the Yolngu language group of north-east Arnhem Land.
In their “Sharing the true stories” study, the researchers found that miscommunication was pervasive, even when both the health care worker and the patient perceived the communication to be effective. Multiple issues were identified — beyond the limited use of interpreters — including “gratuitous concurrence” (when patients tell the health care worker what they think the worker wants to hear); problems with culturally specific understanding and ways of explaining health and illness (eg, health professionals would frequently describe health states using quantification such as percentages of kidney function, which had little meaning for most Yolngu people); and a lack of staff training in cross-cultural communication.
Cass said the paper has engendered a powerful response from people working in all kinds of cross-cultural health settings. “So, I think communication — or miscommunication — issues talk very broadly”, he said.
The study has been presented and cited not only nationally but internationally, leading to ongoing relationships with doctors and educational videomakers in the US. A “Sharing the true stories” website has been developed, with links to further education resources (Box 4). There is also now greater systematic use of interpreters in Indigenous health settings.
Cass is currently involved in several research programs related to Indigenous health. He remains committed to developing and fostering universally available, high-quality education and training in cross-cultural care.
2003: Non-toxic treatment is effective for chronic suppurative otitis media
What would you do if the only treatment your community could access for a particular condition was a product that was potentially toxic in your circumstances? Until recently, Aboriginal health services were faced with treating chronic suppurative otitis media (CSOM) in patients who had a perforated tympanic membrane with aminoglycoside ear drops, which are potentially ototoxic.
In 2001–2002, Sophie Couzos, a public health physician with the National Aboriginal Community Controlled Health Organisation (NACCHO), led the NACCHO Ear Trial, which set out to assess the effectiveness of non-toxic fluoroquinolone ear drops compared with the usual treatment.
Couzos said Dr Puggy Hunter, then NACCHO Chair, had wanted the organisation to instigate and undertake a research project to benefit the Aboriginal community. “Hearing issues were a big priority, and particularly runny ears due to chronic otitis media. The community needed a non-toxic alternative for treating the condition”, she said.
The methodology was to be that of a double-blind randomised controlled trial, so that it would be scientifically meaningful. But the study also had to be community-based, designed in such a way that the Aboriginal organisations had leadership. At the time, Hunter coined the phrase, “We are not just participants, we are in charge”.
As well as providing “real-world” results, the trial was designed to build capacity in the communities so that the intervention would be sustainable and transferable. Thus, the researchers opted for a challenging multicentre approach rather than putting all their investment into only one or two sites. Aboriginal health workers, rather than research assistants, were trained to undertake the trial protocol as part of core primary health care.
Far from resisting the research project, health services were eager to be part of it. “Some services had to be turned away, because of the limited study budget or because they could not meet explicit criteria, such as having a doctor employed within the service”, Couzos said.
Hunter died soon after the NACCHO Ear Trial was underway, but the trial went on to show that non-ototoxic fluoroquinolone drops were more effective than aminoglycoside drops in achieving cure for CSOM.
The paper has had an impact in several key areas. Firstly, thanks to NACCHO’s advocacy role, said Couzos, remote area Aboriginal health services can now provide non-ototoxic ear drops to their clients for free, under Section 100 of the National Health Act 1953 (Cwlth). Secondly, the trial was pivotal to the listing of ototopical fluoroquinolone drops on the Pharmaceutical Benefits Schedule, which means that health care providers in non-remote areas can also provide subsidised medicine. Australian prescribing recommendations have also endorsed the use of fluoroquinolone ear drops in the presence of tympanic membrane perforation.14,15 Finally, in terms of research policy, the NACCHO Ear Trial has provided a real-world example of successful, community-based participatory research.16
2004: The Australian Medical Sheepskin halves incidence of pressure ulcers in lower-risk patients
If you had a product you thought would benefit patients in hospital, how would you get the attention of hospital managers and clinicians? Having developed a sheepskin that they were confident would reduce the incidence of pressure ulcers in low- to moderate-risk patients, staff of the Commonwealth Scientific and Industrial Research Organisation (CSIRO) Leather Research Centre approached Don Campbell at the Royal Melbourne Hospital (RMH) about generating some clinical evidence of efficacy.
“Here was an Australian industry initiative; here was a large public health problem and an opportunity to collaborate. It was a very attractive proposition”, said Campbell. After gaining some initial data from a small trial conducted in a high-risk group setting in Western Australia,17 the research partnership was granted National Health and Medical Research Council (NHMRC) funding for an open-label randomised controlled trial, conducted at the RMH in 2000.
The Australian Medical Sheepskin was designed with a fibre length and density sufficient to perform a pressure distribution function, to minimise shear and friction, and to withstand high-temperature cleansing. In the trial, the sheepskins were used without covering as a partial mattress overlay, in accordance with their design. Sheepskin elbow and heel protectors were also used, as necessary. Of the 441 patients enrolled in the trial, 58 developed pressure ulcers. However, patients randomly assigned to the sheepskin group were less than half as likely to develop pressure ulcers as those in the usual care group.
“Our evidence showed that we had a piece of technology that was clearly of demonstrable benefit. But the sheepskin hasn’t been widely taken up into practice. The real tragedy is that it hasn’t been capitalised on from an Australian perspective”, Campbell said. Sales of the sheepskin have mostly been incidental, for use in non-clinical environments and for people who are bed-bound or in wheelchairs.
In retrospect, Campbell and the study’s first author, medical statistician Damien Jolley, would have liked the trial to have had sufficient funding to incorporate two further features: a third treatment arm, comparing the sheepskin “head to head” with pressure mattresses; and a proper cost-effectiveness analysis, including effects on hospital length of stay. However, what was missing and is still needed for real translation of their study findings into clinical hospital practice, they said, is an industry partner of sufficient size to manage advertising, sales and distribution requirements.
But there is good news too. Recognising that pressure ulcers are a clinical indicator of quality of care, the Victorian Quality Council identified their reduction as a key objective for health care services in Victoria. Since state-wide surveys of the prevalence of pressure ulcers within Victoria’s acute and subacute health services began in 2003, progress has been made in implementing elements of a comprehensive program of pressure ulcer prevention and management. There has been a 33% reduction in the proportion of patients with pressure ulcers, from 26.5% in 2003 to 17.6% in 2006.18
2005: Hand hygiene program reduces nosocomial MRSA rates
Have you ever said you’d like to embark on an ambitious project, not really expecting to be given the opportunity? After an unexpected change in Victorian state government, the infection control team at a Melbourne hospital, Austin Health, suddenly found themselves the recipients of new infection control staff and an opportunity to apply for a state government Quality Improvement Fund grant. Their plan was to try to cut nosocomial methicillin-resistant Staphylococcus aureus infection (MRSA) at Austin Health by 30% over a 3-year period.
The only hitch was that they had no real idea how to achieve their grand goal. “It was kind of exciting and scary at the same time”, said Paul Johnson, one of the study authors.
Around the same time, while in Geneva at a World Health Organization meeting, Johnson arranged to meet Didier Pittet, who had recently published a landmark Swiss study in the Lancet showing that when staff regularly used a hand hygiene solution before and after every patient, contact rates of hospital infections, including MRSA, could be substantially cut.19 The “secret” of encouraging staff to use the solution was to include, along with the antibacterial alcohol and chlorhexidine, an emollient to protect the skin.
“The other insight they had, partly I think because of their French culture, was that you have to engage people at an emotional level as well as cognitive, and one of the ways they set out to do this was by using art — they had these posters that were created as works of art by the staff of each ward to introduce the program ... they called them ‘talking walls’ in Geneva”, said Johnson.
Pittet encouraged the Austin Health group to develop a similar program, and so they did — the multifaceted Operation Clean Start (OCS) program — developing their own hand hygiene solution (DeBugTM) and even adapting the concept of the “talking walls” (Box 5). The hospital staff and, in particular, nurses in infection control were incredibly supportive of OCS. “After we’d introduced it [the program] in one area, there was a real demand to introduce it into the next area, and so on. It just took off like wildfire”, said Johnson.
Run over 3 years, OCS showed that staff’s compliance with hand hygiene improved. The Australian researchers also added an innovation of their own to the project design: by analysing large datasets in the hospital using interrupted time-series analysis, they were able to show a significant reduction in hospital rates of MRSA infections.
After their paper was published, the OCS researchers were approached by the Victorian Quality Council, who were keen to replicate the reduction in MRSA infections state-wide. An alcohol-chlorhexidine hand hygiene program was rolled out initially in six major hospitals and then across the whole of Victoria. At the time of our interview with Johnson, coauthor Lindsay Grayson was in Geneva with Pittet, working with the WHO on aspects of hygiene policy for the world.
2006: Hot water immersion for 20 minutes can relieve the pain of a bluebottle sting
Have you ever imagined conducting your research on a beach in summer? More importantly, what if that research were to turn a time-honoured treatment on its head? It might sound ideal, but Geoff Isbister and colleagues in the coastal NSW city of Newcastle weathered several difficulties in conducting their randomised controlled trial comparing hot water immersion with ice packs for relieving the pain of bluebottle stings.
For example, in addition to the usual ethics committee approval, there was the not-so-small matter of local council approval, particularly in an era when public liability has become a major issue. Then there was the sporadic nature of bluebottle stings — 35 subjects were recruited in a day; 4 weeks went by with no one stung. And what about beach user behaviour — once a sting had eased with treatment, why sit around for the full 20 minutes required by the study protocol?
Although it was organisationally challenging, the actual study was very simple and successfully challenged the existing belief that ice was the best way to relieve pain in this situation. The researchers suggested that the mechanism of reducing pain with heat treatment was the inactivation of venom.
It is still early days since publication. Although local practice has changed on the beaches where the study was conducted, national changes in clinical practice as a result of this study are yet to be fully implemented. However, Isbister hopes that the Australian Resuscitation Council’s recent adoption of the new evidence in their treatment recommendations will mean hot water immersion becomes more widely available, and that cost and safety issues related to installing hot-water plumbing at surf lifesaving clubs around Australia can be resolved. And, after all, people can control the way they choose to treat their own jellyfish stings.20
Isbister is actively involved in much more “bites and stings” research. He said, “Within medicine, there are so many myths and, particularly in my area of research, so little research, that for just about anything you do in clinical practice, you can ask the research question and do it [the research]”.
Twelve winners, one voice
Each year in the MJA we publish over a hundred research papers. Each one has a story: a reason for being, a unique setting, colourful protagonists, a narrative, a resolution and, in many cases, the possibility of development and continuation. As we spoke to the authors of each of the MJA/Wyeth Research Award-winning papers, however, it often seemed as though they were speaking with one voice — the engaged, thoughtful tones of a focused, committed, intelligent and passionate individual, working in the interests of both science and humanity. None had set out to win an award in doing their work; they had all simply wanted to answer a real question in a real area of need.
So what did we learn about what makes a good research paper? Having a question whose answer will have a real impact on public health or clinical practice would seem to be a good start, as would using appropriate, pragmatic methodology. Our MJA/Wyeth winners’ research was also well planned, and each came to embrace the power of collaborative teamwork in conducting their research, not only across medical disciplines but across a diverse range of fields, and often, critically, with study participants.
Accessing funding for good clinical research was not easy for many of our winners, several of whom suggested that Australia needs a formal mechanism within the health and medical research environment to specifically fund applied clinical research.
Publication was also often a thorny issue — when the time came to submit their papers, many award winners reported pressure from their institutions or funding bodies to publish in “high impact” journals, preferably overseas. In the long run, however, they had considered that the MJA was the right journal with the right readership for communicating messages of relevance to Australian clinicians, particularly when local or national health policy needed to be “influenced”. Several interviewees said, in almost precisely the same definite way, that the intent of their research had been to benefit people and patients rather than to further their careers.
Nearly all the award winners were gratified with the impact their work has made since publication. Several were concerned that the long-term sustainability of successful programs was at risk due to funding inadequacies or health service management restructuring beyond their control.
Can a single piece of research change the world? There are a few spectacular examples where this may have been the case but, in the end, as many of our winners acknowledged, most research papers contribute only a fragment to the “big picture” of health and health care. As a powerful example, we leave you with Sophie Couzos’ perspective after completing the NACCHO Ear Trial, the first double-blind randomised controlled trial conducted in, and controlled by, Aboriginal communities:
While healing the tympanic membrane will improve hearing, if you have recurrent infections because your living circumstances aren’t right, then using ear drops will not totally solve the problem. It will create an environment where healing can occur, but the solution to Aboriginal health problems is not just medicines. Although improved access to medicines is vital, the solutions are holistic.
1 The Medical Journal of Australia/Wyeth Research Award-winning articles, 1995–2006, with ISI citations to date*
Gastric emptying in acute overdose: a prospective randomised controlled trial. Susan M Pond, David J Lewis-Driver, Gail M Williams, Adèle C Green, Noel W Stevenson. Med J Aust 1995; 163: 345-349. |
|||||||||||||||
An outbreak of Japanese encephalitis in the Torres Strait, Australia, 1995. Jeffrey N Hanna, Scott A Ritchie, Debra A Phillips, Jack Shield, M Clare Bailey, John S Mackenzie, Michael Poidinger, Bradley J McCall, Phillip J Mills. Med J Aust 1996; 165: 256-260. <eMJA full text> |
|||||||||||||||
A high incidence of melanoma found in patients with multiple dysplastic naevi by photographic surveillance. John W Kelly, Josephine M Yeatman, Cheryl Regalia, Grahame Mason, Amanda P Henham. Med J Aust 1997; 167: 191-194. <eMJA full text> |
|||||||||||||||
Outdoor air pollution and children’s respiratory symptoms in the steel cities of New South Wales. Peter R Lewis, Michael J Hensley, John Wlodarczyk, Ruth C Toneguzzi, Victoria J Westley-Wise, Trevor Dunn, Dennis Calvert. Med J Aust 1998; 169: 459-463. <eMJA full text> |
|||||||||||||||
Impact of improved diagnosis and treatment on prevalence of gonorrhoea and chlamydial infection in remote Aboriginal communities on Anangu Pitjantjatjara Lands. Penny J Miller, Paul J Torzillo, Wayne Hateley. Med J Aust 1999; 170: 429-432. |
|||||||||||||||
Reducing premature death and renal failure in Australian Aboriginals: a community-based cardiovascular and renal protective program. Wendy E Hoy, Philip R Baker, Angela M Kelly, Zhiqiang Wang. Med J Aust 2000; 172: 473-478. <eMJA full text> |
|||||||||||||||
The effects of quality improvement interventions on inhospital mortality after acute myocardial infarction. Ian A Scott, Michael D Coory, Catherine M Harper. Med J Aust 2001; 175: 465-470. |
|||||||||||||||
Sharing the true stories: improving communication between Aboriginal patients and healthcare workers. Alan Cass, Anne Lowell, Michael Christie, Paul L Snelling, Melinda Flack, Betty Marrnganyin, Isaac Brown. Med J Aust 2002; 176: 466-470. <eMJA full text> |
|||||||||||||||
Effectiveness of ototopical antibiotics for chronic suppurative otitis media in Aboriginal children: a community-based, multicentre, double-blind randomised controlled trial. Sophie Couzos, Traven Lea, Reinhold Mueller, Richard Murray, Margaret Culbong. Med J Aust 2003; 179: 185-190. <eMJA full text> |
|||||||||||||||
Preventing pressure ulcers with the Australian Medical Sheepskin: an open-label randomised controlled trial. Damien J Jolley, Robyn Wright, Sunita McGowan, Mark B Hickey, Don A Campbell, Rodney D Sinclair, Kenneth C Montgomery. Med J Aust 2004; 180: 324-327. <eMJA full text> |
|||||||||||||||
Efficacy of an alcohol/chlorhexidine hand hygiene program in a hospital with high rates of nosocomial methicillin-resistant Staphylococcus aureus (MRSA) infection. Paul D R Johnson, Rhea Martin, Laurelle J Burrell, Elizabeth A Grabsch, Susan W Kirsa, Jason O’Keeffe, Barrie C Mayall, Deidre Edmonds, Wendy Barr, Christopher Bolger, Humsha Naidoo, M Lindsay Grayson. Med J Aust 2005; 183: 509-514. <eMJA full text> |
|||||||||||||||
A randomised controlled trial of hot water (45°C) immersion versus ice packs for pain relief in bluebottle stings. Conrad Loten, Barrie Stokes, David Worsley, Jamie E Seymour, Simon Jiang, Geoffrey K Isbister. Med J Aust 2006; 184: 329-333. <eMJA full text> |
|||||||||||||||
* As of August 2007. ISI = Institute for Scientific Information (now Thomson Scientific). | |||||||||||||||
3 Backyard pigpens on the outer Torres Strait islands
 |
|
Pigpens (A) adjacent to swampy conditions or (B) situated over standing water were found to breed Culex annulirostris mosquitoes. |
4 Artwork from the “Sharing the true stories” website
 |
|
Courtesy: Phyllis Batumbil, Matamata, Northern Territory. http://www.sharingtruestories.com. |
Competing interests
None identified.
Acknowledgements
We would like to thank Wyeth Australia for their generous support of this award for the past 12 years, and the interviewees for their time and willing participation.
References
- Kulig K, Bar-Or D, Cantrill SV, et al. Management of acutely poisoned patients without gastric emptying. Ann Emerg Med 1985; 14: 562-567. 0_i1092094
- Krenzelok EP, McGuigan M, Lheur P. Position statement: ipecac syrup. American Academy of Clinical Toxicology; European Association of Poisons Centres and Clinical Toxicologists. J Toxicol Clin Toxicol 1997; 35: 699-709. 0_i1092096
- Hanna JN, Ritchie SA, Phillips DA, et al. Japanese encephalitis in north Queensland, Australia, 1998. Med J Aust 1999; 170: 533-536. 0_i1092098
- Hanna JN, Ritchie SA, Eisen DP, et al. An outbreak of Plasmodium vivax malaria in Far North Queensland, 2002. Med J Aust 2004; 180: 24-28. 0_i1092100
- Holly EA, Kelly JW, Shpall SN, Chiu SH. Number of melanocytic nevi as a major risk factor for malignant melanoma. J Am Acad Dermatol 1987; 17: 459-468. 0_i1092102
- Banky JP, Kelly JW, English DR, et al. Incidence of new and changed nevi and melanomas detected using baseline images and dermoscopy in patients at high risk for melanoma. Arch Dermatol 2005; 141: 998-1006. 0_i1092104
- Hensley MJ, Chalmers A, Clover K, et al. Symptoms of asthma: comparison of a parent-completed retrospective questionnaire with a prospective daily symptom diary. Pediatr Pulmonol 2003; 36: 509-513. 0_i1092106
- Gibson PG, Simpson JL, Chalmers AC, et al. Airway eosinophilia is associated with wheeze but is uncommon in children with persistent cough and frequent chest colds. Am J Respir Crit Care Med 2001; 164: 977-981. 0_i1092108
- Nganampa Health Council. Programs — STD. http://www.nganampahealth.com.au/std.php (accessed Nov 2007).
- Hoy WE, Kondalsamy-Chennakesavan SN, Nicol JL. Clinical outcomes associated with changes in a chronic disease treatment program in an Australian Aboriginal community. Med J Aust 2005; 183: 305-309. 0_i1092112
- Scott IA, Eyeson-Annan ML, Huxley SL, West MJ. Optimising care of acute myocardial infarction: results of a regional quality improvement project. J Qual Clin Pract 2000; 20: 12-19. 0_i1092114
- Scott IA, Darwin IC, Harvey KH, et al. Multisite, quality-improvement collaboration to optimise cardiac care in Queensland public hospitals. Med J Aust 2004; 180: 392-397. 0_i1092116
- Scott IA, Derhy PH, O’Kane D, et al. Discordance between level of risk and intensity of evidence-based treatment in patients with acute coronary syndromes. Med J Aust 2007; 187: 153-159. 0_i1092118
- Black RJ, Cousins VC, Chapman P, et al. Ototoxic ear drops with grommet and tympanic membrane perforations: a position statement [letter]. Med J Aust 2007; 186: 605-606. 0_i1092120
- Antibiotic Expert Group. Therapeutic guidelines. Antibiotic. 13th ed. Melbourne: Therapeutic Guidelines Limited, 2006: 236-240. 0_i1092122
- Couzos S, Lea T, Murray R, Culbong M. ‘We are not just participants — we are in charge’: the NACCHO ear trial and the process for Aboriginal community-controlled health research. Ethn Health 2005; 10: 91-111. 0_i1092124
- McGowan S, Montgomery K, Jolley D, Wright R. The role of sheepskins in preventing pressure ulcers in elderly orthopaedic patients. Primary Intention 2000; 8: 127-134. 0_i1092126
- Strachan V, and Clinical Epidemiology and Health Services Evaluation Unit, Melbourne Health. PUPPS 3 — Pressure ulcer point prevalence survey. Statewide report 2006. Melbourne: Victorian Department of Human Services, 2006. http://www.health.vic.gov.au/pressureulcers/pupps.htm (accessed Nov 2007).
- Pittet D, Hugonnet S, Harbarth S, et al. Effectiveness of a hospital-wide programme to improve compliance with hand hygiene. Infection Control Programme. Lancet 2000; 356: 1307-1312. 0_i1092132
- Avorn J. The sting of ignorance [op-ed]. The New York Times 2006; 16 Sep. 0_i1092133