




The known: In the decade preceding the “No jab, no pay” policy, childhood vaccination rates in Australia were stable at 90–92%.
The new: The linking of vaccination status with family assistance payments under the “No jab, no pay” policy was followed by considerable catch‐up vaccination activity. Nearly one in five young people not fully vaccinated against measles were vaccinated during the first two years of the policy.
The implications: Promoting catch‐up vaccination to improve coverage among children aged 5 years or more and adolescents should improve disease control. A full evaluation of the population health and social effects of the “No jab, no pay” policy and associated measures is still needed.
Childhood vaccination coverage in Australia is high by international standards.1 Coverage increased from 1997 with the introduction of vaccination incentives and improved recording in the Australian Childhood Immunisation Register (ACIR),2 especially among 12‐ and 24‐month‐old children, but plateaued at 90–92% in the decade to 2014.2,3 The proportion of 12‐month‐old children deemed fully vaccinated reached 93.9% in 2018, and that of 60‐month‐old children reached 94.0%, having increased from less than 83% in 2009.4 These figures are close to the national target of 95%, the level required for herd immunity for measles control.5
A number of initiatives for increasing vaccination coverage in children have been introduced in Australia in recent years. State‐specific “No jab, no play” policies, adopted by four of eight jurisdictions by January 2020, permit children to attend childcare only if they are fully vaccinated, enrolled in an approved catch‐up program, or have medical reasons for not being vaccinated.5
The national “No jab, no pay” policy,6,7 introduced on 1 January 2016, extended the existing vaccination requirements for receiving federal family assistance payments8 by removing non‐medical (conscientious objection) exemptions and tightening guidelines for medical exemptions.5,9 Payments with vaccination requirements — the Family Tax Benefit part A supplement and Child Care Benefit/Child Care Rebate (replaced by the Child Care Subsidy from July 2018) — may total $15 000 per child per year for lower income families.7 In 2016–17, 39% of the more than 4 million families in Australia with children received the means‐tested Family Tax Benefit part A, and 22% received the Child Care Rebate (not means‐tested at that time) or the Child Care Benefit.10,11,12
Until 2012, vaccination requirements for family assistance payments were assessed at 2 and 5 years of age, and at 1, 2, and 5 years of age during 2012–2015.8,13,14 Under “No jab, no pay”, they were initially assessed annually to the age of 20 years, but eligibility for the Child Care Subsidy has been assessed fortnightly since 1 July 2018. “No jab, no pay” was accompanied by ACIR extending its recording of vaccinations to 20 (instead of 7) years of age, and subsequently expanding to the whole‐of‐life Australian Immunisation Register (AIR) as part of a package of initiatives for strengthening the vaccination program.3
Some countries have long standing compulsory vaccination policies, and others have recently introduced or are considering them, but national monetary sanction policies are unique to Australia,15 attracting international interest.9 Evidence for their effectiveness in increasing vaccination rates is limited.8,15 Given its greater impact on socio‐economically disadvantaged families, the effectiveness of “No jab, no pay”, its impact on access to early childhood education, and other aspects of social equity have also caused concern.6,7
The effects of “No jab, no pay” have not been formally assessed. As vaccination coverage increased both before and after its introduction, its contribution to these changes cannot be assessed on the basis of standard childhood milestone reporting alone. Catch‐up vaccination — that is, later than recommended in the National Immunisation Program schedule — is also important for optimising population protection against highly contagious diseases such as measles. For example, adolescents and adults born in Australia since 1966 are less protected against measles than the preceding generation, and as many as one in five are not fully protected by two‐dose vaccination or natural infection.16
We therefore explored changes in the of rates of catch‐up vaccination of older children and adolescents during the first two years of the “No jab, no pay” policy.
Methods
The “No jab, no pay” policy was implemented on 1 January 2016. We analysed AIR data in a cross‐sectional investigation of catch‐up vaccination of people to age 20 years in the two years immediately preceding and the two years following the introduction of the policy.
Cross‐sectional data analyses
We analysed AIR data on catch‐up vaccination during the two two‐year periods 1 January 2013 – 31 December 2014 (ie, prior to “No jab, no pay”; baseline) and 1 December 2015 – 31 December 2017. We selected 1 December 2015 as the start of the “No jab, no pay” period because preliminary analysis of AIR data identified that catch‐up vaccination of older children increased during December 2015 and was notified to the expanded register from 1 January 2016.
To assess baseline catch‐up vaccination activity, we analysed data for children aged 5 to less than 7 years (age on 31 December 2014) who received catch‐up vaccination with the third dose of the diphtheria–tetanus–acellular pertussis vaccine (DTPa3) and the first dose of the measles–mumps–rubella vaccine (MMR1). As only vaccination of children under 7 years was recorded in the ACIR prior to “No jab, no pay”, baseline vaccination data were not available for 7–20‐year‐old people, precluding before‐and‐after comparisons.
For the “No jab, no pay” period, three age groups (age at 31 December 2017) were assessed for selected vaccine doses: 5 to less than 7 years (DTPa3, MMR1); 7 to less than 10 years (second MMR vaccine dose [MMR2], DTPa3); and 10 to less than 20 years (MMR2, third dose of the diphtheria–tetanus–acellular pertussis vaccine as an age‐appropriate vaccine with lower diphtheria/pertussis antigen content [dTpa] than DTPa). MMR2 catch‐up vaccination of children aged 5 to less than 7 years was not assessed because the scheduled vaccination time point was age 4 years until 1 July 2013 (ie, too close to the assessment age) and because of schedule changes during the “No jab, no pay” period (MMR2 recommended at 18 months from July 1 2013). “No jab, no pay” catch‐up vaccination estimates for specified doses were calculated as proportions of people without the relevant dose recorded in the ACIR at 30 November 2015 for whom the dose was subsequently recorded by 31 December 2017.
Catch‐up vaccination by socio‐economic status, Indigenous status, and geographic characteristics
We analysed MMR2 catch‐up vaccinations by jurisdiction, Indigenous status (the 0.4% of people in the AIR with unspecified Indigenous status were classified as non‐Indigenous), socio‐economic status (Australian Bureau of Statistics Socio‐Economic Indexes for Areas [SEIFA] Index of Education and Occupation17), and remoteness of area of residence (Accessibility/Remoteness Index of Australia [ARIA++]18). We focused on MMR2 vaccination because, unlike dTpa vaccination, it is not delivered by jurisdictional school‐based programs, for which vaccination data were not systematically transferred to AIR during the study period, and because MMR2 vaccination is a prerequisite for family assistance payments for people aged 10–19 years (unlike MMR1 vaccination). All statistical analyses were undertaken in SAS 9.4.
Ethics approval
Our analysis of de‐identified surveillance data with the approval of the Australian Department of Health was exempted from formal ethics approval by the Sydney Children's Hospitals Network Human Research Ethics Committee.
Results
Catch‐up vaccination of children aged 5 to less than 7 years (DTPa3, MMR1)
The proportion of children aged 5 to less than 7 years who received catch‐up DTPa3 vaccination was 9.4% (3366 of 35 673 unvaccinated children) during the baseline period and 15.5% (4732 of 30 595 unvaccinated children) during the “No jab, no pay” period (Box 1; Supporting Information, table 1). DTPa3 catch‐up vaccination activity was higher during the “No jab, no pay” period in all jurisdictions. The proportion of children aged 5 to less than 7 years who received catch‐up MMR1 vaccination was 13.6% (4719 of 34 793 unvaccinated children) during the baseline period and 12.9% (4169 of 32 321 unvaccinated children) during the “No jab, no pay” period.
Catch‐up vaccination of children aged 7 to less than 10 years (DTPa3, MMR2)
Of the 42 793 children aged 7 to less than 10 years who had not received DTPa3 by 30 November 2015 (4.4% of children in age group), 5365 (12.5%) had received catch‐up DTPa3 by 31 December 2017. Of the 68 501 children who had not received MMR2 by 30 November 2015 (7.0% of age group), 15 283 (22.3%) had received catch‐up MMR2 by 31 December 2017 (Box 2).
Catch‐up vaccination of people aged 10 to less than 20 years (dTpa3, MMR2)
Of the 296 259 people aged 10 to under 20 years who did not receive DTPa3 by 30 November 2015 (9.7% of age group), 26 146 (8.8%) had received catch‐up dTpa3 by 31 December 2017. Of the 407 332 people who did not receive MMR2 by 30 November 2015 (13.4% of age group), 71 502 (17.6%) had received catch‐up MMR2 by 31 December 2017 (Box 3), increasing overall coverage for this age group to 89.0%.
Socio‐economic status, Indigenous status, and geographic location
The proportion of incompletely vaccinated people who received catch‐up MMR2 during 1 December 2015 – 31 December 2017 was higher in areas of lowest socio‐economic status than in those of highest socio‐economic status, both for children aged 7 to less than 10 years (32.3% v 14.6%) and for young people aged 10 to less than 20 years (29.1% v 7.6%) (Box 4; Supporting Information, table 2).
The proportion of incompletely vaccinated Indigenous Australians who received catch‐up MMR2 during 1 December 2015 – 31 December 2017 was greater than that for non‐Indigenous Australians, both for children aged 7 to less than 10 years (43.4% v 21.9%) and for young people aged 10 to less than 20 years (35.8% v 17.1%) (Box 5; Supporting Information, table 3).
The proportion of incompletely vaccinated children aged 7 to less than 10 years who received catch‐up MMR2 during 1 December 2015 – 31 December 2017 was lower in remote areas than in major cities (18.3% v 22.7%) and regional areas (21.5%). The proportion of incompletely vaccinated people aged 10 to less than 20 years who received catch‐up MMR2 during 1 December 2015 – 31 December 2017 was lower in remote areas than in major cities (15.8% v 17.1%) and regional areas (19.5%) (Supporting Information, table 4).
The number of MMR2 catch‐up doses administered to young people aged 10 to less than 20 years during 1 December 2015 – 31 December 2017 was markedly higher mid‐year (Box 6). Less marked but similar patterns characterised MMR2 catch‐up vaccination of children aged 7 to less than 10 years and dTpa3 catch‐up vaccination of young people aged 10 to less than 20 years (Supporting Information, figures 1 and 2).
Discussion
We report the first AIR data analysis to evaluate changes in catch‐up vaccination of children and adolescents in Australia after the introduction of the “No jab, no pay” policy. We found substantial catch‐up vaccination activity among children against selected vaccine‐preventable diseases after the implementation of this policy. Catch‐up DTPa3 vaccination activity was 65% higher during the first two years of “No jab, no pay” than during the baseline period (15.5% v 9.4%). In the two years immediately following its introduction, people aged 7 to less than 20 years received nearly 87 000 catch‐up MMR2 doses and about 31 500 catch‐up DTPa3/dTpa3 doses. The marked mid‐year peaks in catch‐up vaccination activity in 2016 and 2017 suggest a link with “No jab, no pay”, as vaccination requirements for all relevant family assistance payments were assessed at the end of each financial year (July; but fortnightly for Child Care Subsidy since 1 July 2018). The lower level of peak catch‐up activity in 2017 than in 2016 suggests that the major impact of the new policy was in its initial year.
We found that MMR2 catch‐up vaccination increased coverage among people aged 10 to less than 20 years from 86.6% in 2015 to 89.0% to 2017; this was an important increase, although to a level still below the 95% coverage across all age groups needed to prevent the spread of measles. A considerable proportion of cases in the largest recent measles outbreak in Australia (Sydney, 2012) were in this age group (49 of 168, 29%).19 While endemic measles has been eliminated in Australia, outbreaks linked to imported disease still occur. Maximising MMR vaccination coverage across all age groups is important for maintaining elimination, particularly given the large increases in measles case numbers in many countries during 2018–19.20
High MMR coverage is also needed to maintain the elimination of endemic rubella in Australia, certified by the World Health Organization in 2018;21 catch‐up rubella vaccination of adolescent girls is particularly important to prevent the severe effects on fetuses of congenital rubella infection.
We focused on two vaccines as proxies for catch‐up vaccination in general, but other vaccines that may be missed in early childhood or are required by people with particular medical conditions are also important but insufficiently delivered to adults.22 Vaccination of young people and adults should be more readily monitored as the AIR matures, including through the transfer of data from jurisdictional school‐based vaccination programs.
We found that MMR2 catch‐up vaccination after the introduction of “No jab, no pay” was markedly higher in the lowest than in the highest socio‐economic status areas. This is consistent with a larger proportion of families in disadvantaged areas being eligible for means‐tested family assistance and for whom the “No jab, no pay” policy was therefore relevant. That catch‐up vaccination activity was twice as high among Indigenous as among non‐Indigenous children and young people is similarly attributable to the greater proportion of Indigenous families eligible for family assistance payments; average disposable income for Indigenous people aged 15 years or more is 30% lower than for non‐Indigenous Australians.23 The lower rate of catch‐up activity in remote areas may indicate poorer access to vaccination services. Our data confirm that the financial penalties of the “No jab, no pay” policy have an unequal impact on Australian families, with smaller gains in vaccination coverage of children of higher socio‐economic status. Investigating regional and sub‐regional impacts of the policy, especially in areas with persistently lower coverage, would be useful.
Limitations
Given the cross‐sectional design of our study, changes in catch‐up vaccination activity may not be attributable to the “No jab, no pay” policy alone. For example, some children may have been vaccinated for other reasons, such as overseas travel, pre‐enrolment requirements for further study (eg, in health‐related professions), or because of changes in attitude to vaccination unrelated to “No jab, no pay”. We could not determine whether catch‐up activity among young people over 7 years of age increased with “No jab, no pay” because pre‐2016 data were not available for this age group.
We may have overestimated the number of older children and adolescents who were not up to date with vaccinations at the start of the “No jab, no pay” period, as some may have received catch‐up vaccinations not recorded by the age‐limited ACIR before 2016. However, we probably underestimated the number of catch‐up vaccinations after 2016, as some may not be recorded in the AIR. Taking these factors together, the estimated proportions of older children and adolescents receiving catch‐up vaccinations are probably conservative.
Further, we could not separate the effects of “No jab, no pay” monetary sanctions from those of other measures, some of which were introduced at the same time as “No jab, no pay”, including expanding the availability of free catch‐up vaccines for older children and adolescents. State‐based “No jab, no play” policies should not have affected our findings as they target children under 5 years of age. Finally, the AIR does not include information on socio‐demographic factors such as ethnic background, country of birth, and family size. Linkage with other large databases containing such information is essential for fully evaluating the effects of population‐level vaccination policies.
Conclusion
A considerable degree of catch‐up vaccination activity followed the introduction of “No jab, no pay” in Australia. This should help facilitate disease control, including protecting against a resurgence of measles. Our findings suggest that, while monetary sanctions are effective in promoting catch‐up vaccination, their impact varies with socio‐economic disadvantage. A number of overseas governments have shown interest in various types of compulsory vaccination policy.24 Many factors contribute to incomplete vaccination; a comprehensive suite of measures, particularly for reducing barriers to access and incorporating systematic reminders, is therefore essential for improving coverage.15,24 Finally, the ethical aspects and unintended consequences of “No jab, no pay” and “No jab, no play” policies should also be carefully examined, as recommended for any country considering such measures.7,25
Box 1 – Proportions of incompletely vaccinated children aged 5 to less than 7 years who received catch‐up DTPa3 vaccination, Australia, before and after the introduction of “No jab, no pay”, by jurisdiction*
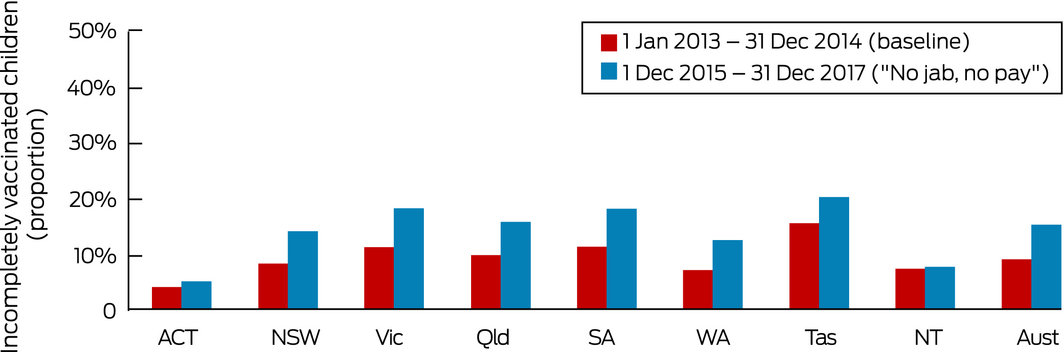
DTPa3 = third dose of diphtheria–tetanus–acellular pertussis vaccine.
Baseline period: children born 1 January 2008 – 31 December 2009 who received catch‐up vaccinations 1 January 2013 – 31 December 2014. “No jab, no pay” period: children born 1 January 2011 – 31 December 2012 who received catch‐up vaccination 1 December 2015 – 31 December 2017. Source: Australian Immunisation Register, data as at 31 December 2014 and 31 December 2017. For absolute numbers, see the online Supporting Information, table 1.
Box 2 – Catch‐up vaccination of children aged 7 to less than 10 years* without recorded vaccine doses before “No jab, no pay” period”, 1 December 2015 – 31 December 2017, by jurisdiction
|
|
|
MMR2 vaccine |
DTPa3 vaccine |
||||||||||||
|
Total number of children |
Not recorded by 30 Nov 2015* |
Catch‐up doses, 1 Dec 2015 – 31 Dec 2017 |
Not recorded by 30 Nov 2015* |
Catch‐up doses, 1 Dec 2015 – 31 Dec 2017 |
|||||||||||
|
|
|||||||||||||||
|
Australian Capital Territory |
16 871 |
1090 |
230 (21.1%) |
666 |
57 (8.6%) |
||||||||||
|
New South Wales |
312 960 |
21 277 |
3999 (18.8%) |
13 094 |
1394 (10.7%) |
||||||||||
|
Northern Territory |
11 096 |
739 |
178 (24.1%) |
548 |
49 (8.9%) |
||||||||||
|
Queensland |
208 851 |
14 941 |
3099 (20.7%) |
9684 |
1199 (12.4%) |
||||||||||
|
South Australia |
63 550 |
4626 |
1444 (31.2%) |
2965 |
553 (18.7%) |
||||||||||
|
Tasmania |
19 977 |
1042 |
272 (26.1%) |
720 |
122 (16.9%) |
||||||||||
|
Victoria |
239 709 |
16 004 |
4074 (25.5%) |
9623 |
1479 (15.4%) |
||||||||||
|
Western Australia |
107 275 |
8782 |
1987 (22.6%) |
5493 |
512 (9.3%) |
||||||||||
|
Australia |
980 289 |
68 501 |
15 283 (22.3%) |
42 793 |
5365 (12.5%) |
||||||||||
|
|
|||||||||||||||
|
DTPa3 = third dose of diphtheria–tetanus–acellular pertussis vaccine; MMR2 = second dose of measles–mumps–rubella vaccine. Source: Australian Immunisation Register (status: 31 December 2017). * Children born 1 January 2008 – 31 December 2010. |
|||||||||||||||
Box 3 – Catch‐up vaccination of people aged 10 to less than 20 years* without recorded vaccine doses before “No jab, no pay” period”, 1 December 2015 – 31 December 2017, by jurisdiction
|
|
|
MMR2 vaccine |
dTpa3 vaccine |
||||||||||||
|
Total number of children |
Not recorded by |
Catch‐up doses, |
Not recorded by |
Catch‐up doses, |
|||||||||||
|
|
|||||||||||||||
|
Australian Capital Territory |
49 146 |
6389 |
897 (14.0%) |
4520 |
262 (5.8%) |
||||||||||
|
New South Wales |
966 624 |
121 483 |
18 652 (15.4%) |
87 224 |
7241 (8.3%) |
||||||||||
|
Northern Territory |
34 769 |
4798 |
743 (15.5%) |
3337 |
226 (6.8%) |
||||||||||
|
Queensland |
653 015 |
91 996 |
15 837 (17.2%) |
67 388 |
4962 (7.4%) |
||||||||||
|
South Australia |
204 277 |
27 640 |
7266 (26.3%) |
17 962 |
2665 (14.8%) |
||||||||||
|
Tasmania |
65 309 |
5893 |
1435 (24.4%) |
3568 |
526 (14.7%) |
||||||||||
|
Victoria |
736 164 |
88 368 |
17 678 (20.0%) |
65 257 |
7733 (11.9%) |
||||||||||
|
Western Australia |
331 158 |
60 765 |
8994 (14.8%) |
47 003 |
2531 (5.4%) |
||||||||||
|
Australia |
3 040 462 |
407 332 |
71 502 (17.6%) |
296 259 |
26 146 (8.8%) |
||||||||||
|
|
|||||||||||||||
|
dTpa3 = third dose of diphtheria–tetanus–acellular pertussis booster vaccine; MMR2 = 2nd dose of measles–mumps–rubella vaccine. Source: Australian Immunisation Register (status: 31 December 2017). * Children born 1 January 1998 – 31 December 2007. |
|||||||||||||||
Box 4 – MMR2 catch‐up vaccination of children aged 7 to less than 10 years* and people aged 10 to less than 20 years† without recorded vaccine doses before the “No jab, no pay” period, 1 December 2015 – 31 December 2017, by socio‐economic status
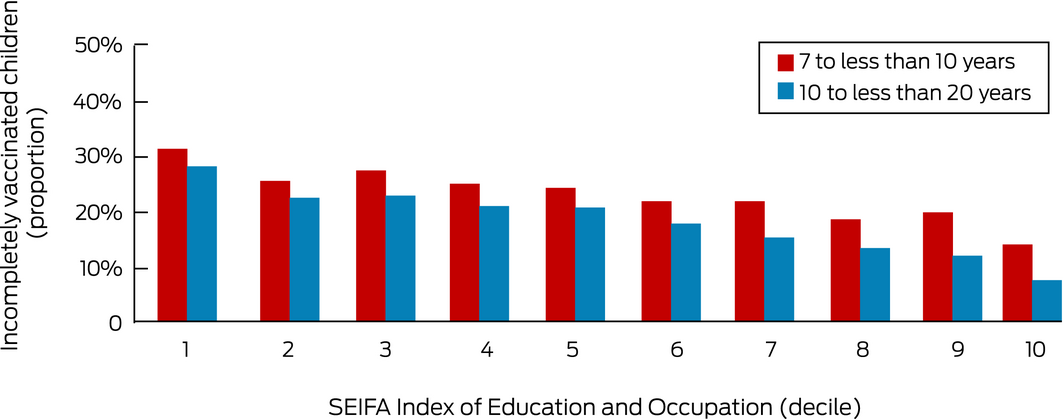
MMR2 = second dose of measles–mumps–rubella vaccine; SEIFA = Socio‐Economic Indexes for Areas: 1 = lowest, 10 = highest socio‐economic status.
* Children born 1 January 2008 – 31 December 2010 who received catch‐up vaccinations 1 December 2015 – 31 December 2017.
† Young people born 1 January 1998 – 31 December 2007 who received catch‐up vaccinations 1 December 2015 – 31 December 2017. Source: Australian Immunisation Register (status: 31 December 2017).
For absolute numbers, see the online Supporting Information, table 2.
Box 5 – MMR2 catch‐up vaccination of children aged 7 to less than 10 years* and young people aged 10 to less than 20 years† without recorded vaccine doses before the “No jab, no pay” period, 1 December 2015 – 31 December 2017, by Indigenous status
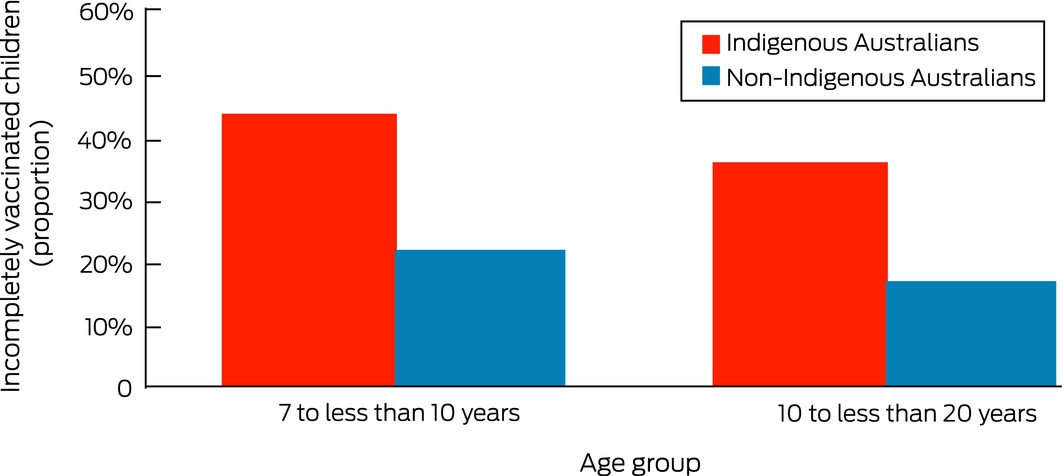
MMR2 = second dose of measles–mumps–rubella vaccine.
* Children born 1 January 2008 – 31 December 2010 who received catch‐up vaccinations 1 December 2015 – 31 December 2017.
† Young people born 1 January 1998 – 31 December 2007 who received catch‐up vaccinations 1 December 2015 – 31 December 2017. Source: Australian Immunisation Register (status: 31 December 2017).
For absolute numbers, see the online Supporting Information, Box 3.
Box 6 – MMR2 catch‐up vaccination of young people aged 10 to less than 20 years* without recorded vaccine doses before the “No jab, no pay” period, 1 December 2015 – 31 December 2017, by month/year of administration
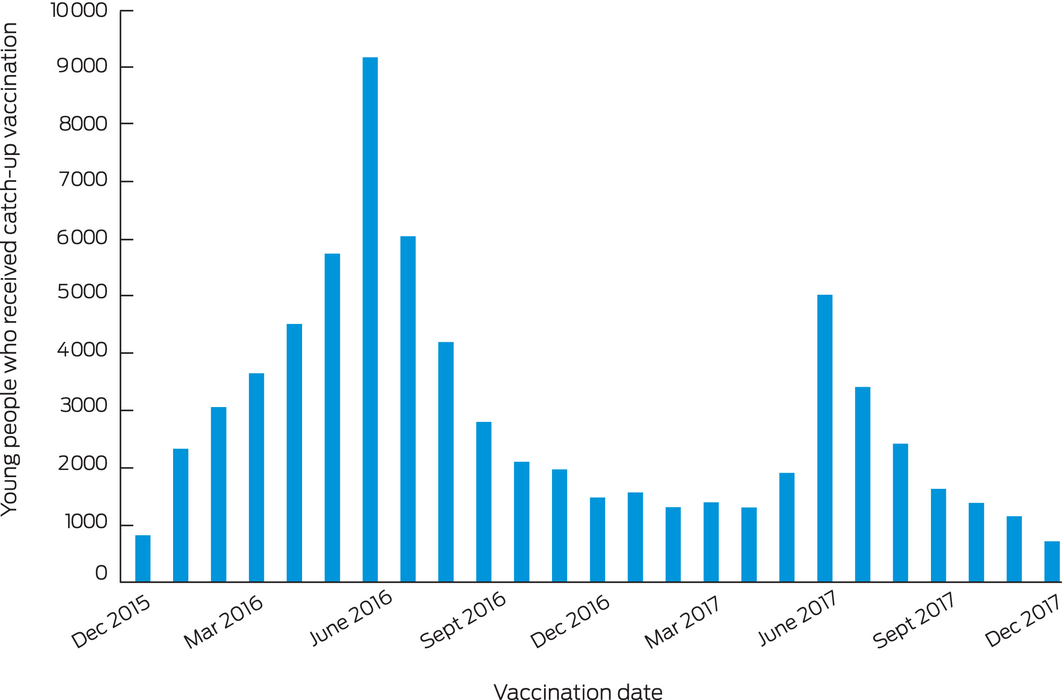
MMR2 = second dose of measles–mumps–rubella vaccine.
† Young people born 1 January 1998 – 31 December 2007 and who received catch‐up vaccination 1 December 2015 – 31 December 2017. Source: Australian Immunisation Register (status: 31 December 2017).
Received 18 December 2019, accepted 15 May 2020

Abstract
Objectives: To assess catch‐up vaccination of older children and adolescents during the first two years of the “No jab, no pay” policy linking eligibility for federal family assistance payments with childhood vaccination status.
Design, setting, participants: Cross‐sectional analysis of Australian Immunisation Register data on catch‐up vaccination of children aged 5 to less than 7 years before (January 2013 – December 2014; baseline) and during the first two years of “No jab, no pay” (December 2015 – December 2017), and of children aged 7 to less than 10 years and young people aged 10 to less than 20 years (“No jab, no pay” period only).
Main outcomes: Catch‐up vaccination rates for measles–mumps–rubella vaccine second dose (MMR2), by age group, Indigenous status, and socio‐economic status; catch‐up vaccination of children aged 5 to less than 7 years (third dose of diphtheria–tetanus–pertussis vaccine [DTPa3], MMR1), before and after introduction of “No jab, no pay”.
Results: The proportion of incompletely vaccinated children aged 5 to less than 7 years who received catch‐up DTPa3 was higher under “No jab, no pay” than during the baseline period (15.5% v 9.4%). Of 407 332 incompletely vaccinated people aged 10 to less than 20 years, 71 502 (17.6%) received catch‐up MMR2 during the first two years of “No jab, no pay”, increasing overall coverage for this age group from 86.6% to 89.0%. MMR2 catch‐up activity in this age group was greater in the lowest socio‐economic status areas than in the highest status areas (29.1% v 7.6%), and also for Indigenous than for non‐Indigenous Australians (35.8% v 17.1%). MMR2 catch‐up activity in 2016 and 2017 peaked mid‐year.
Conclusions: Linking family assistance payments with childhood vaccination status and associated program improvements were followed by substantial catch‐up vaccination activity, particularly in young people from families of lower socio‐economic status.