





Volume 210 - Issue 9
Precision health: treating the individual patient with chronic obstructive pulmonary disease
Authors: Ma'en Obeidat, Mohsen Sadatsafavi and Don D Sin
Med J Aust 2019; 210 (9): 424-428. || doi: 10.5694/mja2.50138
Published online: 20 May 2019
Published online: 20 May 2019
With the advent of better biomarkers and disease-modifying therapeutics in the near future, the era of precision health is coming of age in COPD
Summary
- Chronic obstructive pulmonary disease (COPD) is defined based on a reduced ratio of forced expiratory volume in one second (FEV1) to forced vital capacity (FVC) on spirometry. However, within this definition, there is significant heterogeneity of pathophysiological processes that lead to airflow obstruction and variation in phenotypic manifestations across patients.
- Current pharmacological treatments are based on large randomised clinical trials that apply to an “average” patient.
- Precision health enables tailoring of treatment for each individual patient by taking into account their unique characteristics.
- The number needed to treat (NNT) metric is often used to define implementation of precision health for specific interventions, with common endpoints requiring an NNT ≤ 5 to achieve precision therapy. Higher NNTs may be acceptable for rare but important endpoints such as mortality.
- Long‐acting muscarinic antagonists and inhaled corticosteroids, which are commonly used in COPD, have 1‐year treatment NNTs between 15 and 20 for exacerbation prevention in unselected patients with COPD.
- Subgroup identification using biomarkers or clinical traits may enable precision health. For example, NNT for inhaled corticosteroids is 9 in patients with a blood eosinophil count ≥ 300 cells/μL and 8 for long‐acting muscarinic antagonists in patients with a body mass index ≤ 20 kg/m2.
- Lung volume reduction surgery is associated with an NNT of 6 for survival over 5 years in patients with upper lobe‐predominant disease and low exercise capacity (whereas the NNT is 245 when no bioimaging or exercise markers are used). Continuous domiciliary oxygen therapy (for at least 15 hours/day) has an NNT of 5 for survival over 5 years in patients with resting hypoxemia (PaO2 < 60 mmHg on room air).
- Emerging areas of precision health in COPD with potential for low NNTs in specific circumstances include anti‐interleukin‐5 therapy for eosinophilic COPD, and immunoglobulin replacement therapy for patients with severe immunoglobulin deficiency.
Chronic obstructive pulmonary disease (COPD) is an inflammatory condition of the lung that affects 384 million people worldwide.1 It is a progressive disease, punctuated by periods of acute worsening of symptoms, which are referred to as acute exacerbations of COPD.2 Currently, the mainstays of pharmacologic treatment of COPD are bronchodilators and anti‐inflammatories such as inhaled corticosteroids (ICS).3 Despite their widespread use, they demonstrate no or only modest effects in many patients with COPD.4,5 With the advent of more complex and expensive inhaled triple therapies and biologics, there is a pressing need to develop a more focused strategy for treating patients. Here, we discuss the prospects and progress of precision health in COPD. To identify relevant literature on this topic, we performed a PubMed search of papers published between 1 January 2000 and 31 August 2018 using search terms “COPD”, “emphysema”, “personalized”, “personalised”, “precision”, “precision medicine”, “personalized medicine” and “personalised medicine”.
Traditional patient management versus precision health
The traditional approach to medical practice emphasises the use of evidence from well designed therapeutic studies. These studies often contain data generated from thousands of patients in randomised clinical trials, and therapeutic efficacy is assessed based on differences in the mean value of the primary endpoint between the experimental and control groups. Clinicians are then asked to apply these “mean” or “average” data to individual patients in their practice. The main limitation of this approach is that it disregards the obvious realities of patient care: that there is no such thing as an “average” patient and that every patient is “special” with a unique set of genotype, features and traits. Thus, metrics such as relative risks or hazard ratios or even P values are not particularly useful for guiding patient care at an individual level. For a given patient, therapeutic decisions and outcomes are binary and can be answered by a simple question: does it work? (yes or no). For chronic, progressive disorders such as COPD, therapeutic evaluation and decision making are made difficult by the fact that in many cases, there is no immediate (perceived) symptomatic benefit to the patients and thus the primary motivation for sustained therapy is the belief that over time patients would be better off taking the medications than not taking them. This epistemological approach is inefficient, and very problematic for therapies that have a broad application but are associated with modest effect sizes, are costly or have significant potential to cause harm. In response to this clinical challenge, there has been an explosion of interest in pursuing “precision medicine”, “personalised medicine” and “precision health” in COPD and other therapeutic areas. Although there are subtle but important differences between these terms, in this article, we use “precision health” to define an “approach for disease treatment and prevention that takes into account individual variability in genes, environment, and lifestyle for each person”.6 Simply, precision health is treating the right patient with the right therapy all the time. A key enabling metric for precision health is number needed to treat (NNT), which is defined as the number of patients that need to be treated for one patient to experience benefit. The ideal NNT is 1. However, in reality, most common (preventive) therapeutic products have an NNT of 10–25.4 Although there is no consensus on what constitutes precision health, the upper limit of NNT to achieve precision therapy is likely 5 or less4 for most clinical endpoints and higher for rare but important endpoints such as mortality.
A barrier to precision health: heterogeneity of phenotypes and endotypes
A major challenge of enabling precision health in COPD is its heterogeneity. For simplicity and practical purposes, COPD is defined based on the presence of a single physiological abnormality: reduced ratio of forced expiratory volume in one second (FEV1) to forced vital capacity (FVC), which can be detected reliably on spirometry.3 However, there are likely many different and distinct pathophysiological processes that lead to airflow obstruction. To further complicate matters, there is large variation in the phenotypic manifestations across patients. For instance, patients who have airflow limitation on spirometry can demonstrate a variable mix (or predominance) of emphysema (centrilobular, panlobular, and/or paraseptal), bronchiolitis, bronchiectasis or even fibrosis on chest imaging.3 Patients can also have a wide variety of symptoms: cough, shortness of breath and sputum production, which may not necessarily align with any of the findings on imaging. The belief is that these phenotypic manifestations of patients are by‐products of distinct functional or pathological mechanisms that result from a complex set of interactions between the environment and genes.7 The term “endotype” is now commonly used to describe the molecular processes that lead to or are associated with a particular phenotype of interest. Traditionally, pharmaceutical companies have treated these differences in endotypes as “noise” and used large sample sizes to “drown out” this noise, especially in pivotal phase 3 trials. Accordingly, most of the evidence to support the current management of COPD applies to an average patient and not to the individual patient in clinical practice.4 Given the heterogeneity of COPD, some have suggested possible abandonment of the diagnostic label “COPD” to focus on treatable traits, which are pulmonary and non‐pulmonary phenotypes and even social and psychological issues for which effective treatment exists.8
Non‐pharmacological therapies
Despite these challenges, there are some examples of precision health in COPD. One application is in lung volume reduction surgery. While there were no overall differences in survival between surgically and medically treated patients, patients with predominantly upper lobe emphysema on chest imaging and low exercise capacity (≤ 25 W) experienced a significant survival benefit from a surgical approach with an NNT of 6–7 to prevent one death over 5 years.9 In patients with persistent resting hypoxemia (< 8 KPa) and signs of right‐sided heart failure, the use of continuous domiciliary oxygen therapy improves survival, with an NNT of 5–7 to prevent one death over 5 years.10 In patients who had a recent COPD hospitalisation, pulmonary rehabilitation is associated with an NNT of 5–6 to prevent another hospitalisation over 1 year.11
Preventive health versus precision health
Precision health should not be confused with preventive health. As discussed above, precision health therapies are targeted at specific and usually small subpopulations of patients in order to maximise the benefit–risk ratio for a given individual patient. In contrast, the primary goal of preventive health is to maximise public health benefits to society by applying an intervention to a broad range of patients. A prime example of a preventive health measure is yearly influenza vaccination. While at an individual level, the benefits may be small and unpredictable, resulting in an NNT for exacerbation prevention that may be very high, vaccination is offered to all patients with COPD regardless of their clinical trait or biomarkers, because it is generally safe, relatively inexpensive, effective in all subgroups and, importantly, prevents transmission to others in the community by enabling herd immunity.12 Other examples of preventive health in COPD include smoking cessation (which has an NNT of 200 to prevent one death in COPD over 10 years),13 balanced nutrition and regular aerobic exercise.
Pharmacological therapies
Bronchodilators are the mainstay of chronic COPD management.3 The most commonly used bronchodilators for symptom reduction and exacerbation prevention are long‐acting muscarinic antagonists (LAMAs), which predominantly target the M3 muscarinic acetylcholine receptors in airway smooth muscles; and long‐acting β2 adrenergic agonists (LABAs). The overall impact of long‐acting bronchodilators in preventing acute exacerbations of COPD is significant, with relative risk reductions of 15–25% compared with placebo over 12 months.14,15 This translates to an NNT of about 16 patients for 1 year to prevent one or more exacerbations,16 based on the patient‐based method for NNT calculation. Another approach to NNT calculation is the event‐based method. The NNT to prevent a patient from exacerbation for LABAs and combined ICS–LABA is similar to LAMAs at about 15–20 patients over 1 year of treatment.17 The event‐based method produces a lower NNT of 4 for ICS–LABA therapy. It should be noted that the original NNT calculations were based on dichotomous events and not recurring events. Because exacerbations can be a recurring event in a given individual, the event‐based NNT method tends to produce a lower NNT than the patient‐based method and may therefore exaggerate the benefits of the therapeutic product. In general, patient based NNTs are preferred.18
Chronic prophylactic daily therapy with azithromycin (250 mg/d) is used for patients who are frequent exacerbators despite being treated with triple or dual inhaler therapy (either LABA–LAMA or ICS–LABA). It is associated with an approximate 25% relative risk reduction in the rate of acute exacerbations of COPD, with an NNT of about 9 over 12 months.19 However, daily low dose azithromycin is associated with reduction in hearing acuity; thus, there is another metric (beyond NNT) that needs to be considered before clinical implementation: the number needed to harm (NNH; the number of patients needed to treat before one patient experiences an important adverse effect from the drug). The estimated NNH is 18 patients treated over 1 year.19 Together, these data indicate that the current drugs for COPD are very imprecise and associated (in some cases) with significant adverse effects.
Clinical implementation of precision health
One important pathway towards precision health in COPD is identifying subgroups most likely to benefit from therapeutic products and those unlikely to benefit. For this purpose, a biomarker is required. Biomarkers are broadly defined as “factors that are objectively measured and evaluated as indicators of normal biological or pathological processes, or pharmacological responses to therapeutic interventions”.20 Although biomarkers have been traditionally synonymous with a biochemical or genomic test, in practice a biomarker can be a physiological measurement (eg, FEV1), an anthropometric parameter (eg, body mass index [BMI]), a combination of variables manifested as a risk score (eg, Fracture Risk Assessment Tool [FRAX] score for risk of fractures), or even a single or combination of clinical or demographic variables (eg, age and sex), so long as these features relate to disease and response to treatment. In general, biomarkers can be broadly categorised into response biomarkers (which can be further divided into pharmacodynamic biomarkers and surrogate endpoint biomarkers), prognostic biomarkers (correlated with clinical outcome but not necessarily directly related to specific mechanisms) and predictive biomarkers (which predict response to specific targeted drug interventions).21 The use of these biomarkers in enabling more targeted therapy and therefore precision health is illustrated in Box 1. Some common examples of biomarkers and clinical traits improving the precision of COPD therapies are provided in Box 2.
Improving precision of long‐acting muscarinic antagonists
For LAMAs, an intriguing marker of therapeutic response is BMI. In the POET‐COPD study,25 which compared daily use of tiotropium (LAMA) with salmeterol (LABA), LAMA therapy was associated with an overall 17% relative risk reduction in exacerbation, with an NNT to prevent an exacerbation of 25 (over 1 year). Interestingly, the largest benefit was observed in patients with a BMI < 20 kg/m2 who experienced a relative risk reduction of 0.66 (NNT, 8). Additional studies will be required to validate this observation.
Improving precision of inhaled corticosteroids
A pressing need is for biomarkers to predict therapeutic responses to ICS. Compared with LABA alone, combination ICS–LABA reduces exacerbation by about 10% (NNT, 34 patients per year).22 The impact of ICS and ICS–LABA on hospitalisation is modest, with NNT of 100 and 50 patients per year, respectively, compared with placebo.26 Although to date there is no universally accepted predictive biomarker of ICS, there is growing enthusiasm for using peripheral blood eosinophils to guide ICS therapy. The relationship between blood and sputum eosinophil counts is relatively weak, and blood eosinophil counts do not predict future risk of exacerbations.27 However, they may have some role in predicting responses to ICS in COPD. The FORWARD trial28 showed that treating patients with COPD with a blood eosinophil count ≥ 280 cells/μL with a ICS–LABA combination (beclomethasone and formoterol) inhaler was associated with a 46% reduction in exacerbations over 1 year compared with treatment with formoterol alone (P < 0.001). However, among those with blood eosinophil count < 110 cells/μL, the relative risk reduction was only 22%, which was not significant (P = 0.113).28 Similar findings have been noted by others.29,30 Interestingly, in the recent FLAME study, the use of a LABA–LAMA (indacaterol–glycopyronium) inhaler significantly reduced exacerbation rates compared with ICS–LABA (fluticasone–salmeterol) therapy in patients with COPD whose blood eosinophil count was < 150 cells/μL.31 Above this threshold, the rates of exacerbation were similar between the ICS–LABA and LABA–LAMA groups. In the most recent IMPACT trial, the beneficial effects of ICS–LABA–LAMA (fluticasone–umeclinidium–vilaterol) combination compared with LABA–LAMA (umeclinidium–vilanterol) therapy were greater in patients with a blood eosinophil count ≥ 150 cells/μL compared with those who had counts below this level (relative reduction, 32% v 12%).32 Together, these data suggest that on average, patients with COPD with blood eosinophil counts above ~ 200 cells/μL are more likely to respond to ICS‐containing therapies than patients with eosinophil counts below this level. Those with counts < 150 cells/μL are unlikely to benefit from ICS, and ICS should therefore be avoided in such patients.
Precision therapies for the future
Blood eosinophil counts have also been used to develop biologic drugs that target eosinophils in the pathogenesis of COPD exacerbations. The most discussed are humanised monoclonal antibodies that block interleukin (IL)‐5, which is involved in eosinophil trafficking and maturation. However, recent studies of mepolizumab, a humanised antibody that binds IL‐5 and blocks its signalling, failed to demonstrate that this drug reduces serious exacerbations in patients with COPD. The only subgroup that experienced a significant benefit was patients who had a blood eosinophil count ≥ 300 cells/μL.33 Other IL‐5 pathway modulators are currently being tested in patients with COPD, although preliminary reports suggest that they are largely ineffective in reducing clinically significant acute exacerbations.34
It is now well established that respiratory viral pathogens are the most common triggers of acute exacerbations of COPD. Patients with COPD challenged with rhinovirus are more likely to experience symptoms of dyspnoea and cough and a marked reduction in lung function compared with control subjects who receive the same inoculum of rhinovirus.35 One of the first lines of defence against viral infections is immunoglobulins (IgG), which can be pathogen‐specific or broadly neutralising. A study using two large independent cohorts showed that one in four to one in five patients with COPD have reduced serum (total) IgG levels, consistent with immunodeficiency.36 Most importantly, those who are immunodeficient have a 50–100% increase in the risk of serious exacerbations leading to hospitalisation, independent of other known risk factors for exacerbation. A case series has indicated that treatment of these individuals with IgG replacement therapy significantly reduces the risk of exacerbations.37 In patients with IgG immunodeficiency, who experience recurrent hospitalisations despite maximal inhaler therapy and chronic prophylactic azithromycin therapy, intravenous IgG replacement therapy may be considered.
Can we enable precision health to reduce disease activity in COPD?
Another challenge is developing prognostic biomarkers of disease activity. In COPD, disease activity is generally defined as rapid decline in lung function over time. In general, there are three distinct patterns of lung function trajectory in patients with COPD: accelerated decline, especially after 40 years of age; reduced lung growth during childhood but normal decline as an adult; and a mix of the two trajectories (reduced lung growth and accelerated decline), which leads to severe disease at a younger age. Although these patterns are distinct at the population level, there is tremendous heterogeneity and overlap of patterns over time at an individual level. To date, there is no single blood‐ or lung‐based biomarker that can predict the trajectory of lung function decline in a single individual. In the absence of such tools, it is not surprising that there are no current therapies (aside from smoking cessation) that can modify disease progression or mortality in COPD. As noted previously, while there are many genes that have been reproducibly associated with COPD risk, there are no identified genes (apart from the α1 anti‐trypsin gene) that are associated with disease progression and FEV1 decline.
In a recent study, clinical variables associated with rapid decline in lung function were used to develop a calculator to predict progression of disease at an individual level for patients with mild to moderate COPD.38 The study showed that five clinical features (smoking status, baseline FEV1, BMI, sex, and airway hyper‐responsiveness) were responsible for one‐third of the variation in FEV1 values over time within a single individual. The investigators exploited this knowledge and created an online tool where clinicians can input these parameters and obtain the probability that their patient will progress to higher grades (increase severity) of COPD over 10 years (http://resp.med.ubc.ca/software/ipress/epic/fev1pred/). Data from this tool can be used by clinicians to target high risk patients (ie, those who are likely to progress) with intense smoking cessation programs (where appropriate) or pharmacological (eg, LAMA) and non‐pharmacological therapies (eg, pulmonary rehabilitation) for disease modification. The effects of these interventions can be serially and dynamically assessed using this online tool to determine whether the interventions have made any material difference to the patients’ overall risk over time.
Summary
COPD is (finally) entering the era of precision medicine. Fit‐for‐purpose biomarkers are being developed to predict therapeutic responses and gauge disease activity. Some are already available and should be used by clinicians to manage their patients with COPD. The use of observable characteristics to develop prediction scores for various aspects of disease progression and outcomes should also be considered. Phenotyping of patients is required (Box 1) and, where possible, treatment should target the predominant phenotype/endotype of patients. With the advent of better biomarkers and disease‐modifying therapeutics in the near future, the era of precision health will soon come of age in COPD.
Box 1 – Implementing precision health for patients with chronic obstructive pulmonary disease
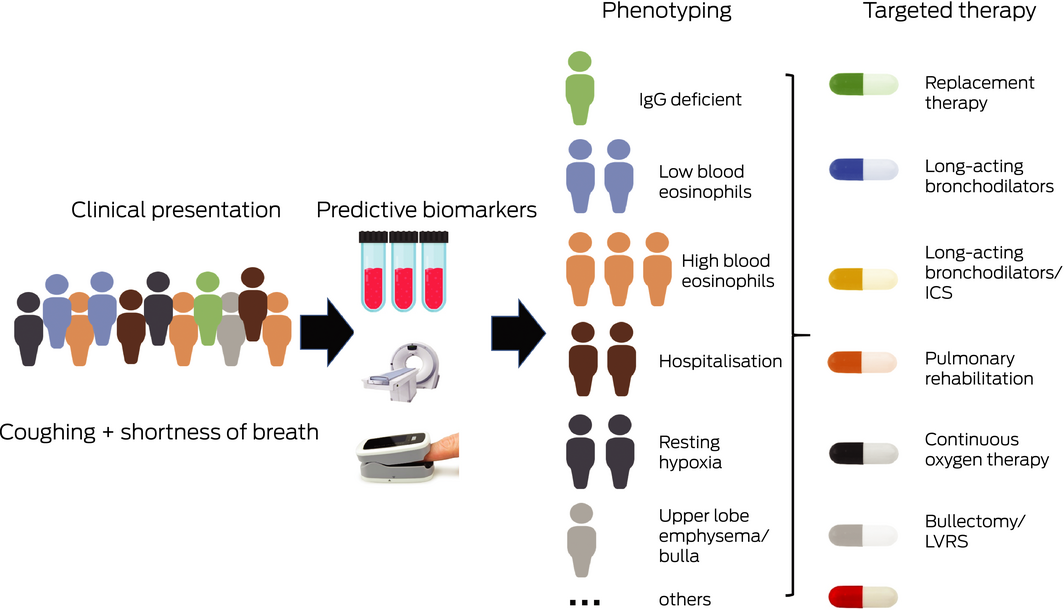
ICS = inhaled corticosteroids; LVRS = lung volume reduction surgery. Chronic obstructive pulmonary disease is a heterogeneous disorder and as such the first step in enabling precision health is to deeply phenotype these patients using a variety of predictive biomarkers, which will allow identification of subgroups of patients who will most likely respond to specific therapies. Biomarkers can be a blood test, lung function measurement, imaging, or clinical prediction tools such as the Lung Function Predictor for COPD Patients (http://ipress.resp.med.ubc.ca/FEV1Pred2/). This will segregate patients into subgroups, which can be targeted with specific therapies.
Box 2 – Examples of precision health in subgroups of patients with chronic obstructive pulmonary disease identified through the use of clinical traits or blood or bioimaging markers
Intervention |
Subgroup |
NNT |
Endpoint prevented |
Treatment period (years) | |||||||||||
LAMA v LABA22 |
Overall |
24 |
Exacerbation |
1 |
|||||||||||
BMI ≤ 20 kg/m2 |
8 |
Exacerbation |
1 |
||||||||||||
GOLD 4* |
7 |
Exacerbation |
1 |
||||||||||||
ICS–LABA–LAMA v LABA–LAMA23 |
Overall |
38 |
Exacerbation |
1 |
|||||||||||
Blood eosinophil ≥ 300 cells/μL |
9 |
Exacerbation |
1 |
||||||||||||
LVRS v no LVRS9 |
Overall |
245 |
Mortality |
5 |
|||||||||||
Upper lobe predominant emphysema and low exercise capacity† |
6 |
Mortality |
5 |
||||||||||||
Domiciliary oxygen v no oxygen therapy |
Overall24 |
56 |
Mortality |
1–6 |
|||||||||||
PaO2 < 60 mmHg10 |
5 |
Mortality |
3 |
||||||||||||
BMI = body mass index; ICS = inhaled corticosteroids; LABA = long‐acting β2‐agonist; LAMA = long‐acting muscarinic antagonist; LVRS = lung volume reduction surgery; NNT = number needed to treat to prevent at least one endpoint in one patient; PaO2 = oxygen tension on room air. * Global Initiative for Chronic Obstructive Lung Disease (GOLD) grade 4 represents FEV1 < 30% of predicted. † 25 W for women and 40 W for men on cardiopulmonary exercise test. | |||||||||||||||
Competing interests
Don Sin has received personal fees for sitting on COPD advisory boards of Sanofi‐Aventis, AstraZeneca and Boehringer Ingelheim, and for speaking engagements from AstraZeneca and Boehringer Ingelheim, outside of the submitted work.
References
- Adeloye D, Chua S, Lee C, et al. Global and regional estimates of COPD prevalence: systematic review and meta‐analysis. J Glob Health 2015; 5: 020415.
- Yang IA, Brown JL, George J, et al. COPD‐X Australian and New Zealand guidelines for the diagnosis and management of chronic obstructive pulmonary disease: 2017 update. Med J Aust 2017; 207: 436–442. https://www.mja.com.au/journal/2017/207/10/copd-x-australian-and-new-zealand-guidelines-diagnosis-and-management-chronic
- Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease 2017 Report: GOLD executive summary. Eur Resp J 2017; 49; https://doi.org/10.1183/13993003.00214-2017.
- Schork NJ. Personalized medicine: time for one‐person trials. Nature 2015; 520: 609–611.
- Li X, Obeidat M, Zhou G, et al. Responsiveness to ipratropium bromide in male and female patients with mild to moderate chronic obstructive pulmonary disease. EBioMedicine 2017; 19: 139–145.
- National Institutes of Health. What is precision medicine? https://ghr.nlm.nih.gov/primer/precisionmedicine/definition (viewed June 2018).
- Rennard SI, Vestbo J. The many “small COPDs”: COPD should be an orphan disease. Chest 2008; 134: 623–627.
- Agusti A, Bel E, Thomas M, et al. Treatable traits: toward precision medicine of chronic airway diseases. Eur Resp J 2016; 47: 410–419.
- Fishman A, Martinez F, Naunheim K, et al. A randomized trial comparing lung‐volume‐reduction surgery with medical therapy for severe emphysema. N Engl J Med 2003; 348: 2059–2073.
- Long term domiciliary oxygen therapy in chronic hypoxic cor pulmonale complicating chronic bronchitis and emphysema. Report of the Medical Research Council Working Party. Lancet 1981; 1: 681–686.
- Puhan MA, Gimeno‐Santos E, Cates CJ, Troosters T. Pulmonary rehabilitation following exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst Rev 2016; (12): CD005305.
- Psaty BM, Dekkers OM, Cooper RS. Comparison of 2 treatment models: precision medicine and preventive medicine. JAMA 2018; 320: 751–752.
- Anthonisen NR, Skeans MA, Wise RA, et al. The effects of a smoking cessation intervention on 14.5‐year mortality: a randomized clinical trial. Ann Intern Med 2005; 142: 233–239.
- Kew KM, Mavergames C, Walters JA. Long‐acting beta2‐agonists for chronic obstructive pulmonary disease. Cochrane Database Syst Rev 2013; (10): CD010177.
- Sin DD, McAlister FA, Man SF, Anthonisen NR. Contemporary management of chronic obstructive pulmonary disease: scientific review. JAMA 2003; 290: 2301–2312.
- Suissa S. Number needed to treat: enigmatic results for exacerbations in COPD. Eur Resp J 2015; 45: 875–878.
- Suissa S. Number needed to treat in COPD: exacerbations versus pneumonias. Thorax 2013; 68(6): 540–3.
- Aaron SD, Fergusson DA. Exaggeration of treatment benefits using the “event‐based” number needed to treat. CMAJ 2008; 179: 669–671.
- Albert RK, Connett J, Bailey WC, et al. Azithromycin for prevention of exacerbations of COPD. N Engl J Med 2011; 365: 689–698.
- Biomarkers Definitions Working Group. Biomarkers and surrogate endpoints: preferred definitions and conceptual framework. Clin Pharmacol Ther 2001; 69: 89–95.
- Kelloff GJ, Sigman CC. Cancer biomarkers: selecting the right drug for the right patient. Nat Rev Drug Discov 2012; 11: 201–214.
- Dransfield MT, Bourbeau J, Jones PW, et al. Once‐daily inhaled fluticasone furoate and vilanterol versus vilanterol only for prevention of exacerbations of COPD: two replicate double‐blind, parallel‐group, randomised controlled trials. Lancet Respir Med 2013; 1: 210–223.
- Cazzola M, Rogliani P, Calzetta L, Matera MG. Triple therapy versus single and dual long‐acting bronchodilator therapy in chronic obstructive pulmonary disease: a systematic review and meta‐analysis. Eur Resp J 2018; 52: 1801586.
- The Long‐Term Oxygen Treatment Trial Research Group. A Randomized Trial of Long‐Term Oxygen for COPD with Moderate Desaturation. New Engl J Med 2016; 375: 1617–1627.
- Vogelmeier C, Hederer B, Glaab T, et al. Tiotropium versus salmeterol for the prevention of exacerbations of COPD. N Engl J Med 2011; 364: 1093–1103.
- Barnes PJ, Bonini S, Seeger W, et al. Barriers to new drug development in respiratory disease. Eur Resp J 2015; 45: 1197–1207.
- Hastie AT, Martinez FJ, Curtis JL, et al. Association of sputum and blood eosinophil concentrations with clinical measures of COPD severity: an analysis of the SPIROMICS cohort. Lancet Resp Med 2017; 5: 956–967.
- Siddiqui SH, Guasconi A, Vestbo J, et al. Blood eosinophils: a biomarker of response to extrafine beclomethasone/formoterol in chronic obstructive pulmonary disease. Am J Resp Crit Care Med 2015; 192: 523–525.
- Pascoe S, Locantore N, Dransfield MT, et al. Blood eosinophil counts, exacerbations, and response to the addition of inhaled fluticasone furoate to vilanterol in patients with chronic obstructive pulmonary disease: a secondary analysis of data from two parallel randomised controlled trials. Lancet Resp Med 2015; 3: 435–442.
- Bafadhel M, Peterson S, De Blas MA, et al. Predictors of exacerbation risk and response to budesonide in patients with chronic obstructive pulmonary disease: a post‐hoc analysis of three randomised trials. Lancet Respir Med 2018; 6: 117–126.
- Roche N, Chapman KR, Vogelmeier CF, et al. Blood eosinophils and response to maintenance chronic obstructive pulmonary disease treatment. data from the FLAME trial. Am J Respir Crit Care Med 2017; 195: 1189–1197.
- Lipson DA, Barnhart F, Brealey N, et al. Once‐daily single‐inhaler triple versus dual therapy in patients with COPD. N Engl J Med 2018; 378: 1671–1680.
- Pavord ID, Chanez P, Criner GJ, et al. Mepolizumab for eosinophilic chronic obstructive pulmonary disease. N Engl J Med 2017; 377: 1613–1629.
- AstraZeneca. Update on TERRANOVA phase III trial for Fasenra in chronic obstructive pulmonary disease. https://www.astrazeneca.com/media-centre/press-releases/2018/update-on-terranova-phase-iii-trial-for-fasenra-in-chronic-obstructive-pulmonary-disease-30052018.html (viewed June 2018).
- Mallia P, Message SD, Gielen V, et al. Experimental rhinovirus infection as a human model of chronic obstructive pulmonary disease exacerbation. Am J Respir Crit Care Med 2011; 183: 734–742.
- Leitao Filho FS, Won Ra S, Mattman A, et al. Serum IgG and risk of exacerbations and hospitalizations in chronic obstructive pulmonary disease. J Allergy Clin Immunol 2017; 140: 1164–1167.e6.
- Cowan J, Gaudet L, Mulpuru S, et al. A retrospective longitudinal within‐subject risk interval analysis of immunoglobulin treatment for recurrent acute exacerbation of chronic obstructive pulmonary disease. PLOS One 2015; 10: e0142205.
- Zafari Z, Sin DD, Postma DS, et al. Individualized prediction of lung‐function decline in chronic obstructive pulmonary disease. CMAJ 2016; 188: 1004–1011.
Provenance: Commissioned; externally peer reviewed.