





Volume 209 - Issue 2 Supplement
Models of care for severe asthma: the role of primary care
Authors: Li Ping Chung, Paula Johnson and Quentin Summers
Med J Aust 2018; 209 (2 Suppl): S34-S40. || doi: 10.5694/mja18.00119
Published online: 17 July 2018
Published online: 17 July 2018
There are a number of barriers in primary, secondary and tertiary settings which compromise optimal care for severe asthma in Australia
Summary
- Severe asthma encompasses treatment-refractory asthma and difficult-to-treat asthma.
- There are a number of barriers in primary, secondary and tertiary settings which compromise optimal care for severe asthma in Australia.
- Guidelines recommend a multidimensional assessment of severe asthma, which includes confirming the diagnosis, severity and phenotype and identifying and treating comorbidities and risk factors. This approach has been found to improve severe asthma symptoms and quality of life and reduce exacerbations.
- Primary care providers can contribute significantly to the multidimensional approach for severe asthma by performing spirometry, optimising therapy and addressing risk factors such as non-adherence and smoking before referring the patient to a respiratory physician for review.
- Primary care practitioners are encouraged to remain engaged with the management of a patient with severe asthma following specialist review by assisting with community-based allied health referrals, managing general medical comorbidities and administering prescribed biological therapies.
- Specialists can support primary care by providing advice to individuals with indeterminate diagnosis, streamlining investigation and management of unrecognised risk factors and complex comorbidities, optimising treatment for severe or difficult asthma including assessment of suitability for and, if appropriate, initiating advanced therapies such as biological therapies.
- When discharging patients back to primary care, specialists should provide clear recommendations regarding ongoing management and should specify the indications requiring further specialist review, ideally offering a streamlined re-referral pathway.
Asthma control has improved globally in recent decades but, despite the availability of effective therapies, it still remains suboptimal.1,2 While milder forms of asthma can be treated adequately in primary care with appropriate use of inhaled corticosteroids (ICS) and bronchodilators as directed by guidelines,3 severe asthma represents a diagnostic and therapeutic challenge, and is associated with a disproportionate economic burden to the community and health care system.4-6
Severe asthma is heterogeneous; it is defined as treatment-refractory disease with persistent symptoms or frequent exacerbations despite optimised standard treatments.7 It includes patients with “difficult-to-treat” asthma, for whom various factors contribute to poor asthma control, and a smaller group of patients with “biologically severe” asthma, who continue to have poor control even after the exclusion of alternative diagnoses and optimisation of contributory factors. For some patients with biologically severe asthma, there are now effective, targeted biological therapies aimed at treating the underlying pathological mechanisms.8-10 However, many patients with difficult-to-treat asthma have comorbidities and risk factors which confound symptoms, and they can obtain significant improvement with careful management of these contributory factors.11 Therefore, it is important to develop models of care that best deal with the complex and varied needs of individuals with severe asthma, with the greater aim of improving patient outcomes for all.12
Primary care providers are at the front line of asthma management, and have the crucial role of early identification and management of uncontrolled asthma. An Australian survey reported that uncontrolled asthma in the community was as high as 45%, with frequent hospital admissions and unscheduled medical visits. Yet, only half the patients had been seen by a general practitioner within the previous year, and only 10% had been reviewed by a specialist.6 This highlights the need for both better guidance for primary care physicians to assist in managing severe or difficult asthma and clear advice about when patients should be referred for respiratory physician review. This Narrative Review will discuss how primary care providers, with support from respiratory physicians, can assist in the broad management of patients with severe asthma.
Current model of care
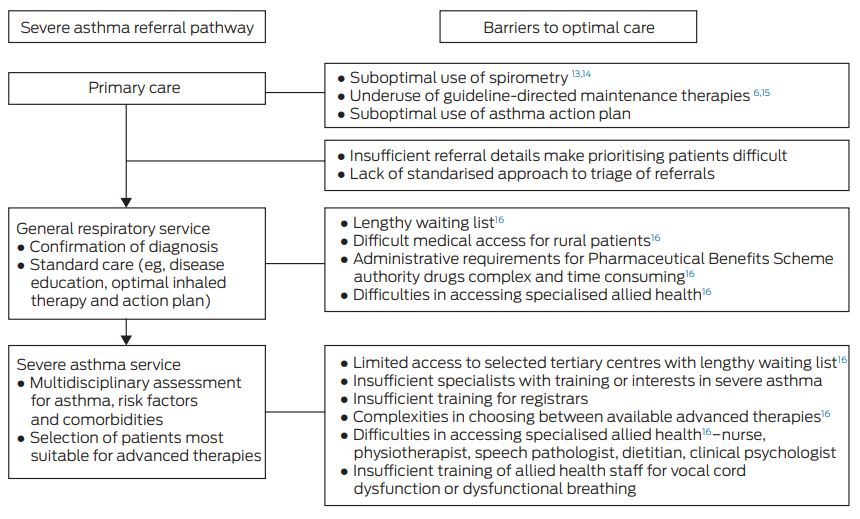
Across Australia, current models of care for severe asthma are variable in different states and hospitals. Most primary care referrals for asthma will be managed in a general respiratory clinic, with selected tertiary centres providing a subspecialised severe asthma multidimensional service (Box 1). Data from Alfred Health in Melbourne suggest that 13% of patients with asthma already seen in a general respiratory clinic would further benefit from subspecialised review for difficult-to-treat asthma.12
A subspecialised severe asthma service offers the advantage of a structured, multidimensional approach to confirm the diagnosis, asthma severity and phenotype and manage risk factors and comorbidities (Box 2).17,18 This multidimensional approach often involves a team of respiratory physicians, nurses and allied health professionals, including physiotherapists, speech therapists, dietitians and clinical psychologists, in secondary or tertiary settings. These health care providers offer physician review, lung function testing, blood tests for peripheral eosinophilia and atopy, optimisation of inhaler use and general disease education, in addition to assessment and management for common comorbidities. It allows further scope for education and self-management skills and access to advanced biological therapies. International guidelines recommend such a multidimensional approach7 based on prospective observational studies showing positive results on asthma symptom control, quality of life and reduced exacerbations.19-21
Barriers to delivery of optimal care
In the current climate, there are numerous barriers to achieving optimal care in Australia (Box 1).16 The asthma care for patients with milder disease in the primary care setting could be improved by increased use of spirometry, increased adherence to guideline-recommended maintenance therapy, and increased utilisation of asthma care plans; the referral process for those with severe or difficult asthma could also be streamlined by providing a detailed referral letter. For patients with asthma who live in rural or remote areas, access to hospital-based clinics may be difficult or impossible. Even within tertiary hospital settings, funding and resource limitations make it challenging to deliver the recommended multidimensional approach, often resulting in prolonged referral waiting times. It is therefore likely that a flexible approach based on effective communication and collaboration between specialists and GPs and between hospital- and community-based resources may be required.
Primary care contribution to the multidimensional assessment and management of severe asthma
A multidimensional approach to severe asthma is not necessarily complex and provides a structured framework for assessment and management — it is equally applicable to the management of milder forms of asthma. As such, some core elements of this approach could be delivered through primary care with help from available community or online resources (Box 3).
Is it asthma?
Multidimensional assessment starts with the diagnosis of asthma based on compatible history and spirometric evidence of variable airflow limitation. Accurate diagnosis helps to avoid unnecessary costs and adverse effects from inappropriate use of pharmacotherapy for presumed severe asthma.
Worldwide, spirometry with or without bronchodilator response is underperformed in primary care for the diagnosis of asthma.13,14 Misdiagnosis of asthma can be as high as 50% due to the suboptimal use of relevant diagnostic testing among patients referred for management of severe asthma in a specialist tertiary setting.22,23 Time constraints, staff training, equipment requirements, suboptimal remuneration and concerns about correct interpretation are common barriers to the routine use of spirometry in primary care. To assist with this problem, there are a variety of resources available in person or online for spirometry training and interpretation (Box 3). Spirometry results with confirmed variable or persistent airflow obstruction will help facilitate triaging and earlier review by specialists when included with the referral.
Is it severe asthma?
Severe asthma is defined as asthma that requires treatment with high dose ICS and one or more other maintenance medication (eg, long-acting β-agonist [LABA], long-acting muscarinic antagonists, leukotriene modifier or theophylline) or oral corticosteroids for more than half the previous year to prevent asthma from becoming uncontrolled, or disease that remains uncontrolled despite this therapy.7 Patients with uncontrolled or severe asthma should be referred for respiratory specialist review.
Is the asthma controlled?
Assessment of asthma control is essential for the initiation and subsequent titration of maintenance inhaler therapy and should be completed at every opportunity. In a multinational survey, 90% of patients self-rated their asthma as well controlled, but of these only 18% were indeed controlled based on the definition in the Global Initiative for Asthma guideline.2 As per these guidelines, a patient with well controlled asthma should have no limitation of activities; no nocturnal, early morning or daytime symptoms; and minimal use of reliever therapy (less than twice per week). It is therefore important to ask direct and specific details of symptom frequency and severity, exacerbation episodes, oral corticosteroid use and emergency department visits. The Asthma Control Questionnaires (www.qoltech.co.uk/acq.html)3 and Asthma Control Test (QualityMetric/GlaxoSmithKline)3 are validated questionnaires that are accessible and easy for patients to complete. They provide a valuable objective framework that can be used to assess response to treatment over time.
Is inhaler therapy optimised?
Guideline-recommended maintenance therapy
Best practice management of severe asthma starts in primary care with guideline-based therapies, including appropriate use of inhalers. In the United Kingdom, in the national review of asthma deaths that occurred between February 2012 and January 2013, expert panels identified multiple factors that could have contributed to these deaths.1 Suboptimal implementation of guidelines was observed in 46% of deaths; there was excessive prescription of short-acting β-agonist, and, most importantly, there was underprescription of maintenance therapy — 80% patients were prescribed less than the recommended maintenance inhaler therapy in the previous year. There was also evidence of inappropriate prescription of LABA as monotherapy.
Australian studies have similarly revealed suboptimal use of asthma medications and poor asthma control in the primary care setting, and highlighted the importance of regular, ongoing education for patients and their GPs.6,15 The Australian guidelines3 have been applauded for their well rounded collaborative approach, with involvement from major stakeholders including subspecialty physicians, primary care providers, pharmacists and asthma foundations.24 Maintenance therapy using low dose ICS followed by addition of LABA should be considered for any patient who experiences daytime or night-time symptoms or who uses reliever therapy more than twice per week. Appropriate knowledge and implementation of national guidelines with improved ICS use can reduce unscheduled primary care or ED visits.25,26
Managing non-adherence and poor inhaler technique
Appropriate use of inhaler therapy is fundamental to the treatment of asthma. A significant proportion of patients referred for severe asthma assessments have poor adherence,20,27 which can and should be managed in primary care. In some Australian reports, only 10% of patients were able to use their inhaler device correctly.3 Critical mistakes are common for all inhaler devices, ranging from 12% for metered dose inhalers, 35% for Diskus (GlaxoSmithKline) and HandiHaler (Boehringer Ingelheim), and 44% for Turbuhalers (AstraZeneca).28 Poor inhaler technique is associated with increased risk of hospitalisation and increased exacerbations requiring oral corticosteroids.28
GPs face considerable challenges in managing adherence, inhaler technique and the provision of asthma action plans. Barriers include time and financial constraints as well as patient behaviour, such as presenting only when unwell and poor insight and prioritisation of their medical needs.29 However, a study showed that a group of Australian GPs were receptive to training in motivational interview-based adherence counselling using the five As framework (ie, ask, assess, advice, assist and arrange) and classic techniques such as OARS (ie, open questions, affirmation, reflective listening and summary reflections).30 Although implementation can be challenging, 96% of the participating GPs rated the training as very or extremely useful, and were able to incorporate the skills in their usual practice with confidence.
For any inhaler device prescribed, patients should be provided with clear instruction, including physical demonstration, and should have their technique checked regularly. Trained practice nurses, educators at asthma foundations or pharmacists may also be helpful in this regard.
Asthma action plan and prompt interventions of exacerbations
Asthma action plans are highly recommended as they can be useful in educating patients about early recognition of exacerbation, and guide appropriate intervention strategies to prevent further deterioration.3,18 The Australian Asthma Handbook provides guidance as to how these action plans should be completed, including specific recommendations for escalation of therapy based on their usual maintenance regime.3 There are increasing data showing that early treatment using temporary escalation of ICS may ameliorate the need for oral prednisolone in the event of an exacerbation.
Optimising referral and discharge pathways
Referral to a specialist should be initiated for patients with severe or difficult asthma or suspicion of alternative or coexisting disease, including chronic obstructive pulmonary disease (Box 4). Barriers to timely respiratory physician review may include unclear reason for referral, travel distance, patient factors and lengthy waiting lists.31 GPs hold an important role as advocates for their patients in securing a prioritised review at the appropriate clinic, especially in a tertiary hospital setting. The inclusion of details such as asthma symptom severity, exacerbation frequency, past and current therapies and spirometry results are important. Earlier specialist review is more likely for patients who have undergone appropriate assessments and treatments for milder asthma before referral.16
It is equally important that clear recommendations and support from specialists are in place to facilitate transfer back to primary care when severity, symptoms or lung function are stabilised. However, only a third of attendees at a round table meeting for severe asthma were either able to or comfortable with discharging patients under these circumstances. A further 11% indicated they would never refer patients back to primary care,16 which may not be sustainable in any tertiary or private specialist setting. Recommendations from the specialist about ongoing management and the indications requiring future specialist review and their urgency may be useful (Box 3).
Management of comorbidities in primary care
In patients with poorly controlled asthma, there is a high prevalence of comorbidities (Box 5) that contribute to symptoms, affect quality of life and increase the risk of exacerbations.23,32-34 Opinion leaders have recently proposed that many comorbidities and risk factors associated with severe asthma are considered “treatable traits” and that their treatment may lead to positive clinical outcomes.12,35,36
Overall, GPs are better placed to assist in and coordinate the management of the range of comorbidities contributing to severe asthma, including corticosteroid-related morbidities.37 Many of these comorbidities are chronic in nature and require regular ongoing assessments that are better facilitated in a primary care setting. Referral and access to a community-based dietitian and clinical psychologist is often invaluable and more convenient for patients when provided nearer to home. Furthermore, the concept of comorbidities and confounding illnesses are equally relevant in patients with milder asthma routinely managed in primary care. Access to the various allied health services in the primary care setting could be facilitated by use of existing GP Management Plans and Team Care Arrangements or Mental Health Treatment Plans.
Some comorbidities such as vocal cord dysfunction and dysfunctional breathing, however, require input from speech pathologists and physiotherapists with more specific skills and experience, who are likely only to be accessible in a tertiary setting.
Role of primary care in the administration of biological therapies for asthma
Until recently, the primary choice of therapy for recurrent exacerbations was repeated or long term use of corticosteroids. New treatments such as omalizumab (Pharmaceutical Benefits Scheme [PBS]-listed anti-IgE therapy for severe atopic asthma), mepolizumab (PBS-listed anti-interleukin [IL]-5 therapy for severe eosinophilic asthma) and benralizumab (Therapeutic Goods Administration-approved anti-IL-5 therapy for severe eosinophilic asthma) dramatically improve symptom control and reduce exacerbations and oral corticosteroid use in patients with severe refractory asthma.10
At present, according to strict PBS criteria, these therapies can only be initiated by a respiratory physician. It is possible that some patients with severe asthma requiring biological therapies could be more effectively comanaged by GPs or their referral physician working outside a dedicated asthma service. Both omalizumab and mepolizumab can be safely administered subcutaneously in a primary care setting after an initial period of observation at a hospital or specialist setting.18 Using omalizumab as an example, leaving aside the complexity of the approval process and drug cost, up to a third of respiratory physicians during a round table discussion also identified limited service availability or travel distance to access treatment as barriers to therapy for eligible patients.16 The exact extent of this problem is unclear without systematic collection of data, but it is an important area to address in order to avoid disadvantaging patients with severe asthma who live in rural areas. One strategy would be to work with local primary or secondary care providers who are geographically closer to the patient. There are resources available to assist specialists and primary care providers with this transition.18 GPs’ ability to assist with administration of biological therapies and surveillance for adverse events would be invaluable in reducing the burden on specialist severe asthma services, and would free up specialist capacity to offer their services to more patients. It is also advantageous for GPs to remain involved in the care of these patients, as biological therapies will be increasingly prescribed in the coming years across many disciplines of medicine.
Nursing support
Evidence for nurse-led asthma clinics in the primary care setting is inconclusive. The quality of evidence in this area is probably affected by patients’ poor clinic attendance, and practice nurses may not be adequately trained or supported to deliver the necessary self-management education.38 A GP asthma clinic involving a trained specialist nurse followed by GP consultation was shown to be potentially be cost-effective in the Australian setting if it could translate to broad benefits in reducing ED presentations, unscheduled GP visits, hospitalisations and days off work.39 However, this proposal was based on a small intervention trial with outdated cost estimates from 2003, and may not reflect the true costs of national implementation.
Partnership with pharmacists
There is good evidence in Australia that community pharmacists can be upskilled to take on a greater scope of practice, which includes identification and referral of patients with poorly controlled asthma who may otherwise not present to other health care providers. Trained pharmacists can improve asthma control by ascertaining and communicating to GPs the risk factors contributing to poor control, such as insufficient use of maintenance ICS/LABA therapy, poor inhaler technique and smoking.40,41
Potential use of electronic records to improve asthma care
General practices are increasingly adopting software systems that allow the use of reminders and facilitate preventive care. In a randomised controlled trial in a UK primary care setting, a novel approach using an electronic asthma risk registry was found to reduce asthma hospitalisations, ED presentation and unscheduled GP visits by 50%, 26% and 21%, respectively. There was also increased prescription of recommended preventive therapies, which was considered cost-effective.42 The at-risk registry identified potential patients with severe or difficult-to-control asthma based on the British asthma guidelines.42 Electronic alerts were added to the medical records of at-risk patients at participating primary care practices. This was coupled with practice-based training about the use of alerts to improve patient access and opportunistic management of asthma at every possible contact.
The increasing use of the MyHealth electronic health record may provide another means of streamlining the care of patients with severe asthma by allowing improved communication between primary and specialist care physicians.
Conclusion
The majority of patients with asthma are managed in primary care, and GPs play a pivotal role in the diagnosis and management of the disease in its milder form and in early referral of patients with severe asthma. A model of care that offers a multidimensional approach to severe asthma may improve patient symptoms and quality of life and reduce exacerbations. There is scope today for better collaboration between specialists and primary care providers in the management of risk factors and comorbidities, in the coordination of community access to allied health input, and in the administration of biological therapies for severe asthma. Further work is still required to streamline and standardise referral and discharge pathways for severe asthma.
Box 2 – Checklist for the systematic assessment of severe asthma
|
Clinical question |
Assessment |
||||||||||||||
|
|
|||||||||||||||
|
Is it asthma? |
|
||||||||||||||
|
Is it severe? |
|
||||||||||||||
|
Is treatment optimal? |
|
||||||||||||||
|
Are self-management skills optimal? |
|
||||||||||||||
|
Are trigger factors identified and managed? |
|
||||||||||||||
|
Is comorbidity identified and managed? |
|
||||||||||||||
|
What is the pattern of airway inflammation? |
|
||||||||||||||
|
What is the optimal individualised management plan? |
|
||||||||||||||
|
|
|||||||||||||||
|
FeNO = fractional exhaled nitric oxide. Source: developed within the National Health Medical Research Council Centre of Excellence in Severe Asthma, reproduced with permission.18 |
|||||||||||||||
Box 3 – The role of primary care in the multidimensional model of care for asthma
|
|
|||||||||||||||
|
Assessment of airway pathology |
|||||||||||||||
|
Is it asthma? |
|
||||||||||||||
|
Is it severe asthma? |
|
||||||||||||||
|
Is the asthma controlled? |
|
||||||||||||||
|
Management |
|||||||||||||||
|
Is inhaler therapy optimised? |
|
||||||||||||||
|
Asthma action plan3 |
|
||||||||||||||
|
Smoking cessation advice |
|
||||||||||||||
|
Ongoing coordinated care |
|||||||||||||||
|
Comorbidities |
|
||||||||||||||
|
Targeted therapies |
|
||||||||||||||
|
Collaboration between primary and specialist care |
|
||||||||||||||
|
|
|||||||||||||||
|
ACQ = Asthma Control Questionnaire. ACT = Asthma Control Test. ALF = Australian Lung Foundation. GORD = gastroesophageal reflux disease. ICS = inhaled corticosteroid. LABA = long-acting β-agonist. NAC = National Asthma Council. OSA = obstructive sleep apnoea. * For example, www.toolkit.severeasthma.org.au. † See www.asthmahandbook.org.au/resources/tools/control-questionnaires (Sources: ACT, QualityMetric and GlaxoSmithKline. ACQ, Juniper EF, O’Byrne PM, Guyatt GH, et al. Development and validation of a questionnaire to measure asthma control. Eur Respir J 1999; 14: 902-907). |
|||||||||||||||
Box 4 – Referral for respiratory physician review
|
|
|||||||||||||||
|
When to refer |
|
||||||||||||||
|
Details to include in referral letter (to enable appropriate triage of patients) |
|
||||||||||||||
|
|
|||||||||||||||
|
ICS = inhaled corticosteroids. LABA = long-acting β-agonist. |
|||||||||||||||
Box 5 – Average prevalence of comorbidity conditions across different studies
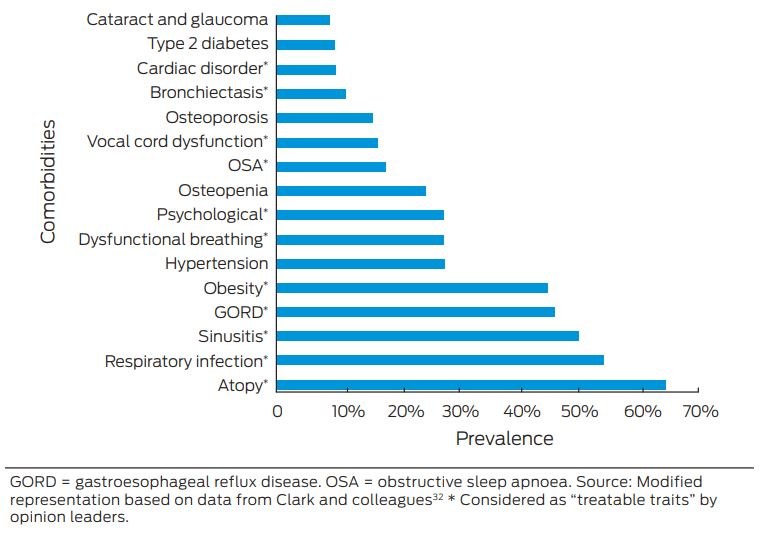
GORD = gastroesophageal reflux disease. OSA = obstructive sleep apnoea. Source: Modified representation based on data from Clark and colleagues32 * Considered as “treatable traits” by opinion leaders.
Competing interests
No relevant disclosures.
Acknowledgements
We thank John Upham for his advice on the overall direction and content for this article, and Irene Dolan for reviewing the article from a GP's perspective.
References
- Royal College of Physicians. Why asthma still kills: the National Review of Asthma Deaths (NRAD). Confidential Enquiry Report, May 2014. London: RCP, 2014. http://www.rcplondon.ac.uk/projects/outputs/why-asthma-still-kills (viewed Apr 2018).
- Price D, David-Wang A, Cho SH, et al. Time for a new language for asthma control: results from REALISE Asia. J Asthma Allergy 2015; 8: 93-103.
- National Asthma Council Australia. Australia Asthma Handbook [website]. www.asthmahandbook.org.au (viewed May 2018).
- Chipps BE, Zeiger RS, Borish L, et al. Key findings and clinical implications from the Epidemiology and Natural History of Asthma: Outcomes and Treatment Regimens (TENOR) study. J Allergy Clin Immunol 2012; 130: 332-342.
- Australian Institute of Health and Welfare: Australian Centre for Asthma Monitoring 2009. Burden of disease due to asthma in Australia 2003. Cat. no. ACM 16. Canberra: AIHW; 2003. https://www.aihw.gov.au/getmedia/cc80b5d0-bb8a-4ddc-a8ac-a60c665c8fff/acm-16-10749.pdf.aspx?inline=true (viewed May 2018).
- Reddel HK, Sawyer SM, Everett PW, et al. Asthma control in Australia: a cross-sectional web-based survey in a nationally representative population. Med J Aust 2015; 202: 492-496.
- Chung KF, Wenzel SE, Brozek JL, et al. International ERS/ATS guidelines on definition, evaluation and treatment of severe asthma. Eur Respir J 2014; 43: 343-373.
- Bel EH, ten Brinke A. New anti-eosinophil drugs for asthma and COPD. Chest 2017; 152: 1276-1282.
- Grainge CL, Maltby S, Gibson PG, et al. Targeted therapeutics for severe refractory asthma: monoclonal antibodies. Expert Rev Clin Pharmacol 2016; 9: 927-941.
- Upham JW, Chung LP. Optimising treatment for severe asthma. Med J Aust 209 (2 Suppl): S22-S27.
- Bel EH, Sousa A, Fleming L, et al; Unbiased Biomarkers for the Prediction of Respiratory Disease Outcome (U-BIOPRED) Consortium. Diagnosis and definition of severe refractory asthma: an international consensus statement from the Innovative Medicine Initiative (IMI). Thorax 2011; 66: 910-917.
- Agustí A, Bafadhel M, Beasley R, et al. Precision medicine in airway diseases: moving to clinical practice. Eur Respir J 2017; 50: 1701655.
- Dennis SM, Price JD, Vickers MR, et al. The management of newly identified asthma in primary care in England. Prim Care Respir J 2002; 11: 120-122.
- Dennis SM, Zwar NA, Marks GB. Diagnosing asthma in adults in primary care: a qualitative study of Australian GPs’ experiences. Prim Care Respir J 2010; 19: 52-56.
- Bosnic-Anticevich S, Kritikos V, Carter V, et al. Lack of asthma and rhinitis control in general practitioner-managed patients prescribed fixed-dose combination therapy in Australia. J Asthma 2017: 1-11.
- McDonald VM, Maltby S, Reddel HK, et al. Severe asthma: current management, targeted therapies and future directions — a roundtable report. Respirology 2017; 22: 53-60.
- Gibson PG, McDonald VM. Management of severe asthma: targeting the airways, comorbidities and risk factors. Intern Med J 2017; 47: 623-631.
- Centre of Excellence in Severe Asthma [website]. 2017 www.severeasthma.org.au (viewed May 2018).
- Tay TR, Lee J, Radhakrishna N, et al. A structured approach to specialist-referred difficult asthma patients improves control of comorbidities and enhances asthma outcomes. J Allergy Clin Immunol Pract 2017; 5: 956-964.
- van der Meer A-N, Pasma H, Kempenaar-Okkema W, et al. A 1-day visit in a severe asthma centre: effect on asthma control, quality of life and healthcare use. Eur Respir J 2016; 48: 726-733.
- Gibeon D, Heaney LG, Brightling CE, et al. Dedicated Severe asthma services improve health-care use and quality of life. Chest 2015; 148: 870-876.
- von Bülow A, Backer V, Bodtger U, et al. The level of diagnostic assessment in severe asthma: a nationwide real-life study. Respir Med 2017; 124: 21-29.
- Heaney LG, Conway E, Kelly C, et al. Predictors of therapy resistant asthma: outcome of a systematic evaluation protocol. Thorax 2003; 58: 561-566.
- Becker AB, Abrams EM. Asthma guidelines: the Global Initiative for Asthma in relation to national guidelines. Curr Opin Allergy Clin Immunol 2017; 17: 99-103.
- Carlton BG, Lucas DO, Ellis EF, et al. The status of asthma control and asthma prescribing practices in the United States: results of a large prospective asthma control survey of primary care practices. J Asthma 2005; 42: 529-535.
- Cloutier MM, Wakefield DB, Sangeloty-Higgins P, et al. Asthma guideline use by pediatricians in private practices and asthma morbidity. Pediatrics 2006; 118: 1880-1887.
- Gamble J, Stevenson M, McClean E, Heaney LG. The prevalence of nonadherence in difficult asthma. Am J Respir Crit Care Med 2009; 180: 817-822.
- Melani AS, Bonavia M, Cilenti V, et al; Gruppo Educazionale Associazione Italiana Pneumologi Ospedalieri. Inhaler mishandling remains common in real life and is associated with reduced disease control. Resp Med 2011; 105: 930-938.
- Watkins K, Fisher C, Misaghian J, et al. A qualitative evaluation of the implementation of guidelines and a support tool for asthma management in primary care. Asthma Res Pract 2016; 2: 8.
- Foster JM, Smith L, Usherwood T, et al. General practitioner-delivered adherence counseling in asthma: feasibility and usefulness of skills, training and support tools. J Asthma 2016; 53: 311-320.
- Fradgley EA, Paul CL, Bryant J. A systematic review of barriers to optimal outpatient specialist services for individuals with prevalent chronic diseases: what are the unique and common barriers experienced by patients in high income countries? Int J Equity Health 2015; 14: 52-67.
- Clark VL, Gibson PG, Genn G, et al. Multidimensional assessment of severe asthma: a systematic review and meta-analysis. Respirology 2017; 22: 1262-1275.
- Tay TR, Radhakrishna N, Hore-Lacy F, et al. Comorbidities in difficult asthma are independent risk factors for frequent exacerbations, poor control and diminished quality of life. Respirology 2016; 21: 1384-1390.
- Boulet LP. Influence of comorbid conditions on asthma. Eur Respir J 2009; 33: 897-906.
- Agusti A, Bel E, Thomas M, et al. Treatable traits: toward precision medicine of chronic airway diseases. Eur Respir J 2016; 47: 410-419.
- Bardin PG, Rangaswamy J, Yo SW. Managing comorbid conditions in severe asthma. Med J Aust 209 (2 Suppl): S11-S17.
- Sweeney J, Patterson CC, Menzies-Gow A, et al; British Thoracic Society Difficult Asthma Network. Comorbidity in severe asthma requiring systemic corticosteroid therapy: cross-sectional data from the Optimum Patient Care Research Database and the British Thoracic Difficult Asthma Registry. Thorax 2016; 71: 339-346.
- Cranston JM, Crockett AJ, Ross JR, et al. Models of chronic disease management in primary care for patients with mild to moderate asthma or COPD: a narrative review. Med J Aust 2008; 188: S50-S52.
- Mogasale V, Vos T. Cost-effectiveness of asthma clinic approach in the management of chronic asthma in Australia. Aust N Z J Public Health 2013; 37: 205-210.
- Armour CL, Lemay K, Saini B, et al. Using the community pharmacy to identify patients at risk of poor asthma control and factors which contribute to this poor control. J Asthma 2011; 48: 914-922.
- Garcia-Cardenas V, Armour C, Benrimoj SI, et al. Pharmacists’ interventions on clinical asthma outcomes: a systematic review. Eur Respir J 2016; 47: 1134-1143.
- Smith JR, Noble MJ, Musgrave S, et al. The at-risk registers in severe asthma (ARRISA) study: a cluster-randomised controlled trial examining effectiveness and costs in primary care. Thorax 2012; 67: 1052-1060.
Provenance: Commissioned; externally peer reviewed.
Treatment and Survival Outcomes for Indigenous and Non-Indigenous Australians Within the Victorian Lung Cancer Registry: A Retrospective Cross-Sectional Cohort Study
Melanie Wong, Mike Lloyd, Jessie Zeng, Sanuki Tissera, Kalinda E. Griffiths, Justine Clark, Jonathan Gillies, Lisa Briggs, Jacqueline Lesage, Tom Wood, Craig Underhill, Sagun Parakh, Louis B. Irving, Wasek Faisal, Rob Blum, Gary E. Richardson, Phillip Parente, Michelle Caldecott, Inger Olesen, Javier Torres, Evangeline Samuel, Christopher Lyne, Katharine See, David Langton, Thomas John, Gavin Wright, Matthew Conron, James Bartlett, Golsa Adabi, Maggie Moore, Susan Harden, Zoe K. McQuilten, John R. Zalcberg, Rob Stirling
Worsening Asthma Outcomes in Australian Adults: A Comparison of Stratified Sample Surveys in 2012 and 2021
Helen K. Reddel, Maria R. Ampon, Leanne M. Poulos, Sharon R. Davis, Brett G. Toelle, Guy B. Marks, Taehoon Lee
Impact of the 2025 New South Wales Respiratory Syncytial Virus Prevention Program on Infant Notifications and Hospitalisations: A Population-Based Analysis
Janaki Amin, Sally L. Ellis, Christopher Lambeth, Jessica Gugusheff, Christine Selvey
Spatial and Temporal Patterns in Childhood and Adolescent Asthma Hospitalisations in Queensland, Australia: A 20-Year Ecological Study Across Climate Zones
Jialu Wang, Javier Cortes-Ramirez, Janet Davies, Wenbiao Hu
The CURE Asthma roadmap
Gary P Anderson, Anthony Flynn, Phil G Bardin, John D Blakey, Shyamali C Dharmage, Paul Foster, Peter G Gibson, Adam Jaffe, Alan James, Christine R Jenkins, Sundram Sivamalai, Peter D Sly, Guy B Marks, Vanessa M McDonald, Judy Wetttenhall
Defining “cure” for the asthmas
Dennis Thomas, Vanessa M McDonald, Peter G Gibson, Richard Y Kim