




The re-emergence of mild iodine deficiency in Tasmania in the late 1990s1 led the state government to introduce a voluntary bread fortification program in 2001, under which the baking industry replaced regular salt in bread with iodised salt. This interim measure preceded the binational response to the widespread re-emergence of iodine deficiency in Australia and New Zealand, where iodisation of bread has been mandatory since 2009.
The impact of voluntary and mandatory fortification has been assessed in urinary iodine surveys of school children in Tasmania,2 consistent with the guidelines of the World Health Organization, the United Nations Children’s Fund, and the International Council for the Control of Iodine Deficiency Disorders.3 Representative samples of school children are assessed as a proxy group for the general population. Population iodine nutrition is considered adequate when the median urinary iodine concentration (UIC) is in the range 100–200 μg/L and fewer than 20% of samples have values under 50 μg/L.
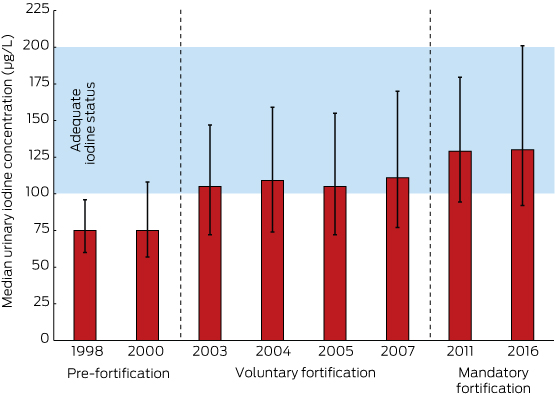
The latest post-mandatory fortification survey was conducted during May–September 2016 (Human Research Ethics Committee [Tasmania] Network, reference, H0015521). Spot morning urine samples collected from 413 school children aged 8–10 years were analysed at the Institute for Clinical Pathology and Medical Research, Westmead (ISO-IEC 17025 accreditation). The median UIC was 130 μg/L; UIC was below 100 μg/L in 124 samples (30.0%) and below 50 μg/L in 13 (3.2%).
Iodine status in 2016 was not significantly different from the 2011 level (129 μg/L; < 50 μg/L: 11 of 320 samples [3.4%]; P = 0.45). In contrast, the median UIC in 2016 was significantly higher than during the voluntary fortification period (2003–2007 surveys: median, 108 μg/L; < 50 μg/L: 142 of 1511 samples [9.4%], P < 0.001) and before fortification (1998, 2000 surveys: median, 75 μg/L; < 50 μg/L: 67 of 411 samples [16%]; P < 0.001) (Box).
Similar changes in iodine status accompanying mandatory fortification have been reported in Australia and New Zealand. For example, the median UIC in 8–10-year-old children improved between the 2003–04 National Iodine Nutrition Survey and the 2011–12 National Health Measures Survey4 from mild or borderline iodine deficiency to adequacy in New South Wales (89.0 to 177.0 μg/L), Victoria (73.5 to 162.5 μg/L), and South Australia (101.0 to 149.9 μg/L). The median UIC in children also increased in the iodine-adequate states of Queensland (136.5 to 165.9 μg/L) and Western Australia (142.5 to 261.3 μg/L).4 In New Zealand, the median UIC in school children increased from 68 μg/L prior to fortification to 113 μg/L (2010–11) and 116 μg/L (2015).5
Improved iodine nutrition in regions formerly affected by mild iodine deficiency shows the success of fortifying bread with iodised salt as a method of population prophylaxis. After 7 years of mandatory fortification, the consistent median UIC from Tasmanian surveys indicates that the outcome of this public health initiative is stable and potentially sustainable. However, these conclusions cannot be extrapolated to all population groups, particularly pregnant and lactating women, as their greater requirement for iodine is unlikely to be met by mandatory fortification alone. The history of iodine nutrition in Tasmania indicates that ongoing monitoring of population iodine nutrition is needed to prevent a return to iodine deficiency.
Received 21 June 2017, accepted 9 August 2017
- 1. Hynes KL, Blizzard CL, Venn AJ, et al. Persistent iodine deficiency in a cohort of Tasmanian school children: associations with socio-economic status, geographical location and dietary factors. Aust N Z J Public Health 2004; 28: 476-481.
- 2. Depaoli K, Seal J, Burgess J, et al. Improved iodine status in Tasmanian schoolchildren after fortification of bread: a recipe for national success. Med J Aust 2013; 198: 492-494. <MJA full text>
- 3. World Health Organization, United Nations Children’s Fund, International Council for Control of Iodine Deficiency Disorders (ed). Assessment of iodine deficiency disorders and monitoring their elimination. A guide for programme managers. 3rd edition. Geneva: WHO, 2007. http://whqlibdoc.who.int/publications/2007/9789241595827_eng.pdf (viewed Oct 2017).
- 4. Australian Bureau of Statistics. 4364.0.55.006. Australian Health Survey: biomedical results for nutrients, 2011-12 [webpage]. Dec 2013. http://www.abs.gov.au/ausstats/abs@.nsf/Lookup/4364.0.55.006main+features12011-12 (viewed June 2017).
- 5. Jones E, McLean R, Davies B, et al. Adequate iodine status in New Zealand school children post-fortification of bread with iodised salt. Nutrients 2016; 8: E298.
The 2016 Urinary Iodine Survey of Tasmanian Schoolchildren was funded by the Tasmanian Department of Health and Human Services.
The Menzies Institute for Medical Research, University of Tasmania, received funding from the Tasmanian State Government Department of Health and Human Services to conduct the 2016 Urinary Iodine Survey of Tasmanian School Children. John Burgess (chair), Judy Seal and Monique Reardon are members of the Tasmanian Ministerial Thyroid Advisory Committee.