





Volume 208 - Issue 2
Frenotomy for tongue-tie in Australian children, 2006–2016: an increasing problem
Authors: Vishal Kapoor, Pamela S Douglas, Peter S Hill, Laurence J Walsh and Marc Tennant
Med J Aust 2018; 208 (2): 88-89. || doi: 10.5694/mja17.00438
Published online: 5 February 2018
Published online: 5 February 2018
The rates of surgical intervention are rising, but the evidence for benefit is limited
There is no universally accepted definition of tongue-tie or ankyloglossia, but it may be described as a congenital abnormality of the lingual frenulum that limits the range of movement of the tongue, interfering with feeding or speech.1,2 There is little consensus among health professionals about how tongue-ties should be managed,1 and little reliable evidence for the benefits of frenotomy.2 A range of techniques are employed to treat clinically significant ties surgically (frenotomy or frenectomy), including scissors and laser surgery. Increases in the number of tongue-tie diagnoses and in lingual frenotomy rates have recently been reported in Canada and the United States.3,4
Clinically significant tongue-tie in breastfeeding pairs was overlooked during the second half of the 20th century. Tongue-tie (and the newer diagnoses of upper lip tie and posterior tongue-tie) have received increased attention following the resurgent commitment of women to breastfeeding over the past decade and the growth in numbers of breastfeeding support professionals.1,5
We retrospectively investigated temporal trends in frenotomy rates in Australia for children aged 0–4 years by analysing de-identified Medicare data for the period 2006–2016 (tongue-tie surgery item codes: 30278, 30281, 52081, 52084). The population of children aged 0–4 years was estimated from Australian Bureau of Statistics census data.6 Categorical data were analysed in χ2 tests, using Stata 14.1 (StataCorp). The Children’s Health Queensland Human Research Ethics Committee granted an ethics review waiver for the study.
During 2006–2016, 52 473 Medicare frenotomy items for 0- to 4-year-old children were recorded; the rate increased from 1.22 per 1000 population in 2006 to 6.35 per 1000 in 2016. The highest rate was for the Australian Capital Territory in 2016 (16.5 per 1000 population; Box 1). The frenotomy rate increased significantly across the study period in the ACT (by 3710%), Western Australia (530%), New South Wales (487%) and Queensland (474%), but not in Tasmania (Box 2).
Our results indicate that frenotomy rates in most of Australia have increased significantly over the past decade. Increases have similarly been reported for British Columbia in Canada (2004–2013: 89% increase) and the United States (1997–2012: 866% increase).3,4 Medicare data underestimate the frenotomy rate, as this information does not capture frenotomies in public hospitals, where Medicare rebates are usually not applied. More significantly, Medicare data do not capture frenotomies performed by dentists, particularly laser frenotomy. In the ACT, however, the limited availability of laser frenotomy before 2016 means that Medicare data probably capture most procedures not undertaken in public hospitals. The almost 40-fold increase in the rate of Medicare-rebated frenotomies in the ACT was much greater than the nevertheless marked increases in other Australian states. The magnitude of this increase may provide an indication of how the national frenotomy rate will increase over the next few years, and lead us to question whether this surgical management approach is supported by sufficient evidence.
Box 1 – Frenotomy rates in Australia, 2006–2016, based on Medicare data*
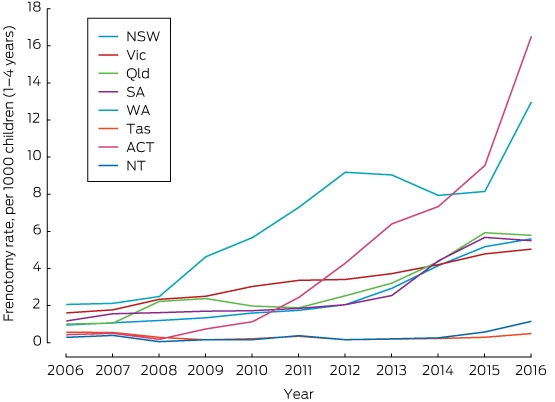
* Numbers of items coded by Medicare item codes, 30278, 30281, 52081, 52084.
Box 2 – Changes in frenotomy rates in Australia, 2006–2016, by state, derived from Medicare data*
|
Region |
2006 |
2016 |
Change in rate, |
||||||||||||
|
Children |
Frenotomies |
Rate per 1000 children (0–4 yrs) |
Children |
Frenotomies |
Rate per 1000 children (0–4 yrs) |
||||||||||
|
|
|||||||||||||||
|
Australian Capital Territory |
20 781 |
9 |
0.43 |
27 816 |
459 |
16.5 |
3710%‡ |
||||||||
|
Western Australia |
129 770 |
267 |
2.06 |
175 292 |
2274 |
13.0† |
530%‡ |
||||||||
|
New South Wales |
431 534 |
411 |
0.95 |
495 452 |
2771 |
5.59† |
487%‡ |
||||||||
|
Queensland |
263 024 |
265 |
1.01 |
319 561 |
1849 |
5.79† |
474%‡ |
||||||||
|
South Australia |
89 004 |
104 |
1.17 |
101 567 |
558 |
5.49† |
370%‡ |
||||||||
|
Northern Territory |
17 561 |
5 |
0.28 |
19 171 |
22 |
1.15† |
303%‡ |
||||||||
|
Victoria |
312 581 |
502 |
1.61 |
396 693 |
1999 |
5.04† |
214%‡ |
||||||||
|
Tasmania |
30 123 |
17 |
0.56 |
30 615 |
15 |
0.49† |
–13% |
||||||||
|
Australia |
1 294 378 |
1580 |
1.22 |
1 566 167 |
9947 |
6.35 |
420% |
||||||||
|
|
|||||||||||||||
|
* Medicare item codes: 30278, 30281, 52081, 52084. † Compared with rate for Australian Capital Territory: P < 0.001. ‡ Calculations used unrounded rates for 2006 and 2016. For all states and territories, except Tasmania: P < 0.001. |
|||||||||||||||
Competing interests
No relevant disclosures.
References
- Power R, Murphy J. Tongue-tie and frenotomy in infants with breastfeeding difficulties: achieving a balance. Arch Dis Child 2015; 100: 489-494.
- O’Shea JE, Foster JP, O’Donnell CPF, et al. Frenotomy for tongue-tie in newborn infants. Cochrane Database Syst Rev 2017; (3): CD011065.
- Walsh J, Links A, Boss E, Tunkel D. Ankyloglossia and lingual frenotomy: national trends in inpatient diagnosis and management in the United States, 1997–2012. Otolaryngol Head Neck Surg 2017; 156: 735-740.
- Joseph KS, Kinniburg B, Metcalfe A, et al. Temporal trends in ankyloglossia and frenotomy in British Columbia, Canada, 2004–2013: a population-based study. CMAJ Open 2016; 4: e33-e40.
- Douglas PS. Rethinking “posterior” tongue-tie. Breastfeed Med 2013; 8: 503-506.
- Australian Bureau of Statistics [website]. 3101.0-Australian Demographic Statistics, Sept 2016. http://www.abs.gov.au/AUSSTATS/abs@.nsf/DetailsPage/3101.0Sep%202016?OpenDocument (viewed June 2017).
Linked content
-
MJA Editorial: Tongue-tie and frenotomy: what evidence do we have and what do we need?
Beds Still Burning: Suicide Should Not Be in the Vocabulary of Children
Rudi Louis Taylor-Bragge
Progressing Cross-Sector Collaboration for People With Eating Disorders and Higher Weight: Priority Actions From an Expert Roundtable Using a Modified Nominal Group Technique
Hiba Jebeile, Leah Brennan, Tracy Burrows, Xochitl de la Piedad Garcia, Angelique F. Ralph, Supreet Saluja, Evan Atlantis, Sarah P. Garnett, Carmel J. Harrison, Eve T. House, Natalie B. Lister, Lisa Moran, Milan K. Piya, Elizabeth Rieger, Evelyn Smith, Phillipa Hay, Sarah Trobe
Intergenerational Child Protection Contact and Child Development Outcomes: A Whole Population Linked Data Study
Meredith Forsyth, Alicia Montgomerie, Kathleen Falster, Deepa Jeyaseelan, Paul Hotton, John Lynch, Rhiannon M. Pilkington
Impact of the 2025 New South Wales Respiratory Syncytial Virus Prevention Program on Infant Notifications and Hospitalisations: A Population-Based Analysis
Janaki Amin, Sally L. Ellis, Christopher Lambeth, Jessica Gugusheff, Christine Selvey
Australian Guidelines for Assessment and Diagnosis of Fetal Alcohol Spectrum Disorder: Overview of the Development Process and Revised Diagnostic Criteria
Natasha Reid, Nicole Hewlett, Nicole Hayes, Zachary Munn, Haydn Till, Delyse Hutchinson, James Stewart, Max Naglazas, Andrea Crawford, Raewyn C. Mutch, Carmela F. Pestell, Rowena Friend, Lisa K. Akison, Chelsea Vanderpeet, Prue Walker, Matthew Gullo, Doug Shelton, Elizabeth J. Elliott, Fiona Kay, Katrina Harris, Jayden Logan, Storm Anderson, Natalie R. Kippin, Seema Padencheri, Sophie Harrington, Diana Barnett, Kelly Skorka, Robyn Doney, Philippa Middleton
Strengthening Care for Children (SC4C), an Integrated Paediatrician‒General Practitioner Model for Reducing Hospital Referral Rates: a Stepped-Wedge Cluster Randomised Controlled Trial
Harriet Hiscock, Cecilia Moore, Sonia Khano, Lena A. Sanci, Kim M. Dalziel, Gary Freed, Douglas I. R. Boyle, Tammy Meyers Morris, Siaw-Teng Liaw, Jane Le, Yvonne A. Zurynski, Susan Woolfenden, Raghu Lingam