





Volume 201 - Issue 1
Experiencing racism in health care: the mental health impacts for Victorian Aboriginal communities
Authors: Margaret A Kelaher, Angeline S Ferdinand and Yin Paradies
Med J Aust 2014; 201 (1): 44-47. || doi: 10.5694/mja13.10503
Published online: 7 July 2014
Published online: 7 July 2014
Abstract
Objectives: To examine experiences of racism in health settings and their impact on mental health among Aboriginal Australians.
Design, setting and participants: A cross-sectional survey of experiences of racism and mental health was conducted in two metropolitan and two rural Victorian local government areas (LGAs) between 1 December 2010 and 31 October 2011. Participants included 755 Aboriginal Australians aged over 18 years who had resided in the relevant LGA for at least a year. The response rate across all LGAs was 99%.
Main outcome measures: Being above or below the threshold for high or very high psychological distress on the Kessler Psychological Distress Scale.
Results: 221 participants reported experiences of racism in health settings in the past 12 months. The results suggested that people experiencing racism in health settings (OR, 4.49; 95% CI, 2.28–8.86) and non-health settings (OR, 2.66; 95% CI, 1.39–5.08) were more likely than people who did not experience racism to be above the threshold for high or very high psychological distress.
Conclusions: Experiencing interpersonal racism in health settings is associated with increased psychological distress over and above what would be expected in other settings. This finding supports the rationale for improving cultural competency and reducing racism as a means of closing the health gap between Aboriginal and other Australians. Capitalising on this investment will require explicitly evaluating the impact of these initiatives on reducing patient experiences of racism.
Racism can be broadly defined as the behaviours, practices, beliefs and prejudices that underlie avoidable and unfair inequalities across groups in society based on race, ethnicity, culture or religion.1 Racism is often conceptualised at three different levels, which overlap in practice: interpersonal racism, internalised racism and systemic or institutional racism.2,3
The link between self-reported experiences of racism and poorer physical and mental health is well documented.4 There is ample evidence that racism contributes to worse health among Aboriginal Australians.5-9 There is also evidence that there are differences in the health care provided to Aboriginal and other Australians and that these differences can contribute to worse health outcomes.10 This in turn suggests that the deleterious effects associated with exposure to racism are likely to be amplified in health settings compared with other settings because of the impacts on future health-seeking behaviour and quality of care in addition to negative psychological and physiological effects.
To date, there has been little research examining exposure to racism in health settings and its impacts on mental health, particularly in comparison with other settings.4 This research is important to informing appropriate antiracism interventions. In this paper we explore three research questions:
- How frequently do Aboriginal Australians experience racism in health settings?
- Are Aboriginal Australians in some demographic groups more likely to encounter racism in health settings than others?
- What are the mental health impacts of exposure to racism in health settings compared with exposure to racism in other settings?
Methods
Survey design
The Aboriginal Experiences of Racism surveys were conducted in two rural and two metropolitan Victorian local government areas (LGAs). These localities were selected for their high levels of cultural diversity compared with other Victorian localities, rather than because of particular concerns about racism in these communities.
Local Aboriginal community interviewers were recruited and trained to administer the surveys with support from the research team. Survey participants were recruited through the interviewers' professional and personal networks. Participants were aged 18 years or older and had lived within their locality for at least 1 year. Surveys were administered face-to-face in group or individual sessions. Interviewers kept consent forms and surveys in separate envelopes at all times in order to reassure participants that their confidentiality would be protected.
Surveys were administered between 1 December 2010 and 31 October 2011. The full survey design and methods are described in the report Mental health impacts of racial discrimination in Victorian Aboriginal communities.11 The study received ethics approval from the University of Melbourne (0932878.6).
Key variables
The key variables used in this paper include:
- demographics: Aboriginality, age, sex and education;
- types of interpersonal racism experienced in the past 12 months;
- settings within which people experienced interpersonal racism;
- mental health, assessed using the 5-item scale based on the Kessler Psychological Distress Scale (K5).12 The reliability of the scale was high among this sample (Cronbach α = 0.85).
For full survey variables used in this paper, please see Appendix 1.
Data analysis
IBM SPSS Statistics version 21 was used to analyse the data. Descriptive analyses were conducted on the demographic composition of the sample, the proportion of people who experienced racism in different settings in the past 12 months and the types of racism experienced in health settings. Logistic regression was used to assess demographic differences between people who reported experiencing racism in health settings and people who did not. The analysis controlled for LGA. Logistic regression was used to assess the relationship between participants' experiences of racism in the past 12 months and being above the threshold for high or very high psychological distress on the K5 scale. Experiences of racism were classified into health settings, other settings and none. Scores of 12 to 25 on the K5 scale are indicative of high or very high psychological distress.12 The analysis controlled for LGA, age, sex and education.
Results
A total of 755 people participated in the Aboriginal Experiences of Racism survey, with a 99% response rate across all LGAs. Demographic data for participants is presented in Box 1. Participants from Rural Councils 1 and 2 made up most of the sample, with Metropolitan Councils 1 and 2 each having fewer than 100 participants. The proportion of the Aboriginal population over 18 years old surveyed was 27% in Rural Council 1, 32% in Rural Council 2, 14% in Metropolitan Council 1 and 7% in Metropolitan Council 2.13 Most participants were women (61.4%), with a mean age of 36 years. About one-fifth of participants held either tertiary, trade or TAFE qualifications (Box 1). The 2011 Census reports that across the four LGAs, most Aboriginal residents over 18 years old are women (55%) with a mean age of 38 years. In the 2011 Census, 11.3% of Aboriginal residents aged 15 years and over in these LGAs held tertiary, trade or TAFE qualifications.13
Experiences of racism
Nearly all participants (97%) reported at least one racist incident in the preceding 12 months, with 25% reporting between one and seven experiences, 38% reporting between eight and 11 experiences and 34% reporting 12 or more experiences.
Participants indicated that racism was most commonly experienced in shops and public spaces, as reported by 67% and 59% of participants, respectively. Nearly one-third of the sample reported experiencing racism within health settings. For details of experiences across all settings, please refer to the full report.11
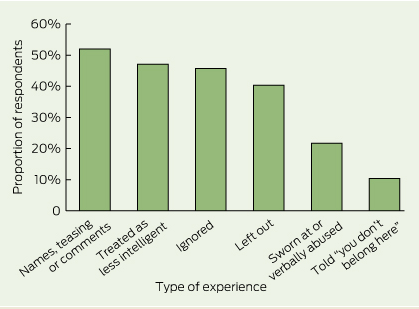
Within health settings, participants most frequently reported being a target of racist names, jokes or teasing, or hearing comments that relied on stereotypes of Aboriginal Australians. This experience was reported by 52% of respondents who reported racism in this setting. Ten per cent of respondents who reported experiencing racism in health care indicated that they had been told that they “didn't belong in Australia”, that they should “go home”, or “get out” within this setting (Box 2).
People aged more than 24 years and people educated at university level or higher were more likely to report experiencing racism within health care (Box 3). However, there were no significant differences between the proportion of men and women who experienced racism in this setting (Box 3).
People who experienced racism in health settings were more likely to be above the threshold for high or very high psychological distress compared with respondents who reported no experiences of racism. Respondents who experienced racism in non-health settings were also significantly more likely than people who did not experience racism to be above the threshold for high or very high psychological distress. The association was less marked than in health settings (Box 4).
Discussion
Almost every Aboriginal Victorian who participated in this survey had experienced at least one racist incident in the previous 12 months.
Nearly a third of people in the study reported racism in health settings in the past 12 months, suggesting considerable room for improvement in creating safe spaces for Aboriginal people. Our study adds to the existing literature on health care provider racism14-16 by showing that experiencing racism in health settings is associated with psychological distress. It is innovative in suggesting that racism in health settings may have a more negative impact than racism in other settings. Racism in health settings may contribute to poorer health through stress-mediated pathways as well as through reduced quality of health care and limited access to health services and other resources that protect and promote health (Appendix 2).17,18
Experiences of racism were less common in health settings than in most other settings, which may in part reflect investment in reducing racism as part of the pathway to improving health care. The need to improve the capacity of mainstream services to meet the needs of Aboriginal Australians has been recognised in National Partnership Agreements to close the gap in Indigenous health outcomes through initiatives to improve cultural competency among mainstream services providers.19,20 However, there has been a lack of effort to evaluative these initiatives and where evaluation has been undertaken, it has thus far focused on changes in providers' attitudes, rather than examining impacts on patient experiences of racism.21 There is therefore little evidence about effective ways of reducing patient exposure to racism within health care settings, including within Australia.22 Nevertheless, a number of evidence-based principles for reducing racial bias in health care providers are supported by social-cognitive psychology, including a focus on individual attributes rather than categorical stereotypes, an improved understanding of bias, enhancement of providers' confidence in interacting with members of dissimilar groups, and improvement in perspective-taking and affective empathy.23 There is also some evidence that developing comprehensive models of care that are orientated to Aboriginal people can have positive impacts on the quality of care.24 Future systematic assessment of cultural competency initiatives will be essential for understanding how best to improve patient experiences in health care settings, and how to conceptualise the intervening steps between practitioner training and patient perspectives.
The results suggest that some Aboriginal Australians are more likely to report experiences of racism than others. Aboriginal Australians who have higher levels of formal education reported higher levels of discrimination than their peers with lower levels of education. This effect was particularly marked for the small number of Aboriginal Australians with university education in the sample. The finding that more educated people in minority groups report higher exposure to racism is consistent with the research literature and is considered to result from a combination of both greater exposure to racism and a higher likelihood of perceiving and reporting experiences of racism.25 People aged over 25 years were more likely to be exposed to racism than younger people. This may reflect differences in actual experiences or be associated with greater use of health services among people aged over 25.
The study has a number of limitations. The survey was cross-sectional, so it is possible that reverse causation is a factor in some of the associations reported. However, existing longitudinal studies suggest that racism is associated with worse health rather than the converse.
While random sampling was not used in this study, the sample demographic profile across the four LGAs closely matches the combined Census profiles.13 The purpose of this study was to explore the associations between experiences of racism and mental health outcomes, rather than examining the prevalence of racism within or between the four localities. Selection into the study was not based on either exposure to racism or mental health status; accordingly, the validity of the relationship observed between experiences of racism and mental health status would not be expected to be affected by the selection process.
The study did not examine characteristics of perpetrators in depth. It is therefore unknown whether racist incidents in health settings were initiated by health care staff, patients or others. Additionally, the study did not assess the type of health services where the racism occurred. Studies providing more setting-specific detail and data about perpetrators would greatly add to the existing literature.
Our study highlights that experiencing interpersonal racism in health settings is associated with increased psychological distress which itself is an indicator of increased risk of mental illness. Such a finding supports the rationale for improving cultural competency and reducing racism as a means of closing the health gap between Aboriginal and non-Aboriginal Australians. Capitalising on this investment will require explicitly evaluating the impact of these initiatives on reducing patient experiences of racism.
1 Demographics of 755 survey participants
Variable | Participants* | ||||||||||||||
Local government area | |||||||||||||||
Rural Council 1 | 313 (41.5%) | ||||||||||||||
Metropolitan Council 1 | 90 (11.9%) | ||||||||||||||
Metropolitan Council 2 | 57 (7.5%) | ||||||||||||||
Rural Council 2 | 295 (39.1%) | ||||||||||||||
Sex | |||||||||||||||
Male | 284 (38.6%) | ||||||||||||||
Female | 451 (61.4%) | ||||||||||||||
Age, years | |||||||||||||||
18–24 | 178 (26.4%) | ||||||||||||||
25–34 | 175 (26%) | ||||||||||||||
35–44 | 174 (25.9%) | ||||||||||||||
45–54 | 90 (13.4%) | ||||||||||||||
55+ | 56 (8.3%) | ||||||||||||||
Education | |||||||||||||||
Below year 10 | 111 (17.2%) | ||||||||||||||
Year 10 | 249 (38.7%) | ||||||||||||||
Year 12 | 108 (16.8%) | ||||||||||||||
TAFE/trade | 128 (19.9%) | ||||||||||||||
University | 48 (7.5%) | ||||||||||||||
Number of experiences | |||||||||||||||
None | 26 (3.4%) | ||||||||||||||
Low (1–7) | 191 (25.3%) | ||||||||||||||
Medium (8–11) | 285 (37.7%) | ||||||||||||||
High (12 +) | 253 (33.5%) | ||||||||||||||
* Denominators vary due to missing data. | |||||||||||||||
3 Demographic characteristics of survey participants and experiences of racism in health care settings in the past 12 months
Demographic characteristics of participants | Experienced racism in a health care setting in past 12 months | Proportion of respondents | Odds ratio | P | |||||||||||
Under 24 years old | Yes | 25.0% | 0.53 (0.35–0.80) | < 0.001 | |||||||||||
No | 33.5% | ||||||||||||||
University education | Yes | 47.9% | 2.60 (1.37–4.97) | < 0.001 | |||||||||||
No | 29.6% | ||||||||||||||
Female | Yes | 32.6% | 0.79 (0.56–1.12) | 0.18 | |||||||||||
No | 29.4% | ||||||||||||||
* Odds ratio adjusted for local government area. | |||||||||||||||
4 Experiences of racism in the past 12 months by setting and being above the threshold for high or very high psychological distress
Experiences of racism by setting | Over the threshold for high or very high psychological distress | Odds ratio | P | ||||||||||||
None | 24.1% | 1.00† | |||||||||||||
In health care setting | 62.4% | 4.49 (2.28–8.86) | < 0.001 | ||||||||||||
In other setting | 47.3% | 2.66 (1.39–5.08) | 0.03 | ||||||||||||
* Odds ratio adjusted for local government area, age, sex and education. † Reference category. | |||||||||||||||
Competing interests
No relevant disclosures.
Acknowledgements
The Aboriginal Experiences of Racism survey was funded by the Lowitja Institute, Australia's National Institute for Aboriginal and Torres Strait Islander Health, the Victorian Health Promotion Foundation (VicHealth) and beyondblue. VicHealth also funded Angeline Ferdinand through its research practice leader program. Margaret Kelaher was supported by an Australian Research Council Future Fellowship. We would like to thank the community workers for their invaluable support in administering the surveys. We would also like to thank Peter Streker and Pamela Rodriguez for their support and advice.
References
- Paradies Y, Chandrakumar L, Klocker N, et al. Building on our strengths: a framework to reduce race-based discrimination and support diversity in Victoria. Full report. Melbourne: Victorian Health Promotion Foundation, 2009. 1
- Berman G, Paradies Y. Racism, disadvantage and multiculturalism: towards effective anti-racist praxis. Ethnic Racial Stud 2010; 33: 214-232. _ENREF_2
- Jones CP. Levels of racism: a theoretic framework and a gardener's tale. Am J Public Health 2000; 90: 1212-1215. _ENREF_3
- Paradies Y. A systematic review of empirical research on self-reported racism and health. Int J Epidemiol 2006; 35: 888-901. _ENREF_4
- Paradies Y, Cunningham J. The DRUID study: racism and self-assessed health status in an Indigenous population. BMC Public Health 2012; 12: 131. _ENREF_5
- Paradies Y, Cunningham J. The DRUID study: exploring mediating pathways between racism and depressive symptoms among Indigenous Australians. Ethnic Racial Stud 2009; 32: 548-573. _ENREF_6
- Priest NC, Paradies YC, Gunthorpe W, et al. Racism as a determinant of social and emotional wellbeing for Aboriginal Australian youth. Med J Aust 2011 194: 546-550. _ENREF_7
- Priest N, Paradies Y, Stewart P, Luke J. Racism and health among urban Aboriginal young people. BMC Public Health 2011; 11: 568. _ENREF_8
- Priest N, Paradies Y, Stevens, M, Bailie R. Exploring relationships between racism, housing and child illness in remote Aboriginal communities. J Epidemiol Community Health 2012; 66: 440-447. _ENREF_9
- Cunningham J, Cass A, Arnold PC. Bridging the treatment gap for Indigenous Australians. Demands for efficiency should not be met at the expense of equity. Med J Aust 2005; 182: 505-506. _ENREF_10
- Ferdinand A, Paradies Y, Kelaher M. Mental health impacts of racial discrimination in Victorian Aboriginal communities. Melbourne: Lowitja Institute, 2013. http://www.lowitja.org.au/lowitja-publishing/L023 (accessed Mar 2014).
- Australian Bureau of Statistics. Inclusion of the K5 in ABS surveys. http://www.abs.gov.au/ausstats/abs@.nsf/Lookup/84330C2EDC3DB940CA2579D50015D74E?opendocument (accessed Jun 2012).
- Australian Bureau of Statistics. 2011 Census community profiles. http://www.abs.gov.au/websitedbs/censushome.nsf/home/communityprofiles?opendocument&navpos=230 (accessed Jun 2012).
- Harris R, Cormack D, Tobias M, et al. The pervasive effects of racism: experiences of racial discrimination in New Zealand over time and associations with multiple health domains. Soc Sci Med 2012; 74: 408-415. _ENREF_14
- Lyles CR, Karter AJ, Young BA, et al. Correlates of patient-reported racial/ethnic health care discrimination in the Diabetes Study of Northern California (DISTANCE). J Health Care Poor Underserved 2011; 22: 211-225. _ENREF_15
- Paradies Y, Truong M, Priest N. A systematic review of the extent and measurement of healthcare provider racism. J Gen Intern Med 2014; 29: 364-387. _ENREF_16
- van Ryn M, Burgess DJ, Dovidio JF, et al. The impact of racism on clinician cognition, behavior, and clinical decision making. Du Bois Rev 2011; 8: 199-218. _ENREF_17
- Shavers VL, Fagan P, Jones D, et al. The state of research on racial/ethnic discrimination in the receipt of health care. Am J Public Health 2012; 102: 953-966. _ENREF_18
- Council of Australian Governments. National partnership agreement on closing the gap in Indigenous health outcomes. Canberra: COAG, 2009. http://www.federalfinancialrelations.gov.au/content/npa/health_indigenous/ctg-health-outcomes/national_partnership.pdf (accessed Mar 2014).
- Commonwealth of Australia. Closing the Gap Indigenous chronic disease package information for general practice, Aboriginal community controlled health services and Indigenous health services (2010). Canberra: Department of Health and Ageing, 2010. http://www.healthinfonet.ecu.edu.au/key-resources/promotion-resources/?lid=20011 (accessed Mar 2014).
- Williams DR, Mohammed SA. Racism and health II: a needed research agenda for effective interventions. Am Behav Sci 2013; 57: 1200-1226. _ENREF_21
- Downing R, Kowal E, Paradies Y. Indigenous cultural training for health workers in Australia. Int J Qual Health Care 2011; 23: 247-257. _ENREF_22
- Burgess D, van Ryn M, Dovidio J, Saha S. Reducing racial bias among health care providers: lessons from social-cognitive psychology. J Gen Intern Med 2007; 22: 882-887. _ENREF_23
- Liaw ST, Lau P, Pyett P, et al. Successful chronic disease care for Aboriginal Australians requires cultural competence. Aust N Z J Public Health 2011; 35: 238-248. _ENREF_24
- Kelaher M, Paul S, Lambert H, et al. Discrimination and health in an English study. Soc Sci Med 2008; 66: 1627-1636. _ENREF_25
Unshrouding Social Determinants: A Case for Standardised Data in Australia's Health Information Ecosystem
Christopher Ryan, Christine T. Shiner, Rebecca J. Harris, Carrie Lethborg, Vijaya Sundararajan
Inequity Is Our Biggest Killer: Looking Upstream to Tackle the Burden of Disease in Australia
Meggan J. Devery, Katie Brooker, Kitty-Rose Foley
Inequity Is Our Biggest Killer: Looking Upstream to Tackle the Burden of Disease in Australia
Lucio Naccarella, Katrina Plamondon, Alison Brown, Alexandra Kent, Sana Shahram, Donya Eghrari, Nicole M. Rankin, Stephanie Best, Marlena Klaic, Zoe Fehlberg, Michelle Lambert, Sue Crengle
Inequity Is Our Biggest Killer: Looking Upstream to Tackle the Burden of Disease in Australia
Saman Khalatbari-Soltani, Edward Jegasothy, Seye Abimbola, Anita van Zwieten
Target Trial Emulation and the TARGET Guideline to Advance Rural and Remote Health Research
Tanvir Kapoor, Harrison J. Hansford, Brooke A. Spaeth, Adam D. Irwin, Aidan G. Cashin