




Electronic cigarettes, or e-cigarettes, are battery-powered devices that produce a vapour (often containing nicotine) which the user inhales, simulating the act of cigarette smoking. Invented in 2003,1 their popularity in the United States and Europe has soared over the past decade.2,3 The public health community has divergent views on the role of e-cigarettes in tobacco control. Proponents argue that they could greatly reduce tobacco harm as a smoking cessation aid, and should therefore be widely available and accessible.4,5 Others question their safety and efficacy as a cessation aid, highlighting their unknown long term health effects, and are concerned that e-cigarettes could re-normalise smoking and, through dual use, reduce the motivation of smokers to quit smoking.6,7 The Australian National Health and Medical Research Council (NHMRC) position statement on e-cigarettes recommends that health authorities should “act to minimise harm until evidence of safety, quality and efficacy can be produced”.8
Although there is increasing international evidence about e-cigarette use, Australian data remain scarce. Recent estimates suggest that 30% of tobacco smokers in the US are currently using e-cigarettes,2,9 and 20% in the United Kingdom,10 reflecting widespread marketing in these countries. The most common reason given for using e-cigarettes is as an aid in quitting smoking,9 despite limited evidence about the effectiveness of e-cigarettes as cessation aids,6,11 especially when compared with more extensively studied options.
Data from the International Tobacco Control (ITC) surveys show that e-cigarette use among current and former Australian smokers increased from 0.6% in 2010 to 7% in 2013.12 In 2014, 8.4% of the New South Wales population had tried e-cigarettes and 1.3% were current users, with smokers being more likely than non-smokers to be users.13 There is no evidence to date, however, about which Australian tobacco smokers are using e-cigarettes, why they are using them, or where they are purchasing them. There is an urgent need for reliable local data that can inform the public health debate, assist in policy development, and guide the development of information for consumers and health practitioners.
E-cigarette regulations concern the product itself, the retail environment in which it is sold, its marketing, or the application of smoke-free policies.14 In Australia, there is currently no national regulation of the ingredients of e-cigarette products, with laws relating to poisons and therapeutic goods applying. Nicotine is legally classified as a dangerous poison,15 and each state and territory has local regulations for the sale of such substances (eg, the NSW Poisons and Therapeutic Goods Regulation 2008).16 As e-cigarettes containing nicotine have not yet been approved by the Therapeutic Goods Administration (TGA), their sale is currently illegal in all Australian jurisdictions; only non-nicotine-containing e-cigarettes can be lawfully sold and used. Each Australian state and territory has differing regulations relating to e-cigarette sales, marketing, and use in smoke-free areas. Amendments to the NSW Public Health (Tobacco) Act17 were passed in June 2015 to include bans on retail displays, print advertising, promotions and sponsorships, and to prohibit supplying of e-cigarettes to minors, harmonising the laws covering e-cigarettes with the relevant tobacco legislation.
Our study assessed how adult tobacco smokers and recent quitters in NSW are using e-cigarettes, tracking changes over an 18-month period in 2014–2015, during which there were no specific NSW regulations relating to the sale, promotion, or use of e-cigarettes. We aimed to identify demographic and smoking-related characteristics of e-cigarette users, to ascertain reasons for using e-cigarettes and commonly reported points of purchase.
Methods
Study design and participants
The Cancer Institute Tobacco Tracking Survey (CITTS) is a serial cross-sectional telephone survey, with 40 interviews conducted in NSW each week. The CITTS monitors smoking-related cognitions and behaviours among adult (18 years and older) current tobacco smokers and recent quitters (quit in the past 12 months). Computer-assisted telephone interviews were conducted using a dual-frame survey design incorporating samples generated by random digit dialling to landline and mobile phone numbers (50/50 split). When calling a landline, a random selection procedure was used to recruit participants within households (selecting the nth oldest eligible adult). When calling a mobile phone, the individual answering the call was considered the target for screening. The screening procedure includes questions relating to current and past smoking. Current smokers are defined as those who currently smoke cigarettes, pipes or other tobacco products daily, at least weekly, or less often than weekly. Recent quitters are those who smoked tobacco products in the past 12 months, but who no longer smoke. Analyses for this study were limited to respondents interviewed between January 2014 and June 2015. The study was funded by the Cancer Institute NSW.
E-cigarette use
All respondents were read a description of e-cigarettes and asked, “How often, if at all, do you currently use e-cigarettes?” (response options: daily, weekly, monthly, less than monthly, not at all). E-cigarette use was coded both as a binary variable (no use v any use) and as a three-level variable (no use, infrequent use [monthly or less often], or frequent use [weekly/daily]). E-cigarette users were asked, “What are the main reasons you currently use e-cigarettes?”, with the response options (a) to cut down on the number of cigarettes I smoke; (b) to help me quit cigarettes; (c) they taste better than cigarettes; (d) they are not as bad for your health as cigarettes; (e) they are cheaper than cigarettes; and (f) so I can smoke in places where smoking cigarettes is not allowed. Multiple responses were allowed. There was also an “other” option, for which responses were recorded verbatim and back-coded to the original code-frame if possible. Users were asked where they bought their last e-cigarette cartridge or liquid, with the options (a) tobacconist; (b) internet; (c) convenience store or petrol station; (d) somewhere else.
Covariates
Data on sex, age and education (low = did not complete high school; moderate = high school diploma or vocational college; high = tertiary education) were included. Postcodes were used to code socio-economic status according to the Socio-Economic Indices for Areas (SEIFA) derived at the 2011 census by the Australian Bureau of Statistics;18 quintiles 4–5 were coded as low socio-economic status, quintiles 1–3 as moderate to high socio-economic status. Postcodes were also used to determine metropolitan or non-metropolitan area of residence. Current tobacco smokers were classified as daily or non-daily smokers, and average daily cigarette consumption and time to first cigarette were combined in the validated Heaviness of Smoking Index (HSI) scores.19
Statistical analyses
We tested for an increase in any and in frequent e-cigarette use across the study period using χ2 tests for linear trends in proportions. To investigate differences in e-cigarette use according to demographic and smoking characteristics, we conducted logistic regression analyses predicting any e-cigarette use (v no use), and frequent use (v infrequent use). For each outcome, two analyses were undertaken. The first used the full sample of smokers and quitters, including demographic characteristics and smoking status as predictors (Model 1). The second used the smoker sample only, and included demographic data, smoking frequency, and HSI scores as predictors (Model 2). The results for demographic predictors were the same for Models 1 and 2; we therefore report the results for smoking characteristics from Model 2 only.
We calculated the proportions of the sample who cited each reason for using e-cigarettes, and of the places of purchase mentioned (with 95% confidence intervals). We used χ2 analyses to assess differences in these responses by subgroups found in previous studies to differ in their patterns of use or their reasons for using e-cigarettes: subgroups defined by age, smoking status, and frequency of use.2,10,13,20 In light of the small number of older adult e-cigarette users, age was categorised in these analyses as 18–29 years v 30 years or older.
Stata 11 (StataCorp) was used for all analyses. Statistical significance was defined as P < 0.05 (two-sided), and was adjusted for multiple comparisons in the subgroup analyses using Bonferroni correction. Because of the slight over-representation of men and mid-aged respondents in the CITTS sample compared with the general NSW population,21 weights were constructed for age, sex, and region of residence. Data weights also accounted for a participant's relative chance of inclusion in the landline or mobile phone sample frame, their chance of selection based on the number of landlines in each household, and the number of in-scope people per household. Weights were applied in logistic regression analyses as p-weights.
Ethics approval
The CITTS is approved by the NSW Population Health Services Research Ethics Committee (reference HREC/10/CIPHS/13).
Results
Over the study period, 283 489 telephone numbers were randomly selected for the survey, 136 392 (48%) were assessed for eligibility (there was no response at the other numbers, or they were non-contactable), and 3345 (2%) of these reached an individual eligible for the study. Of these, 2966 (89%) consented to participate (Box 1).
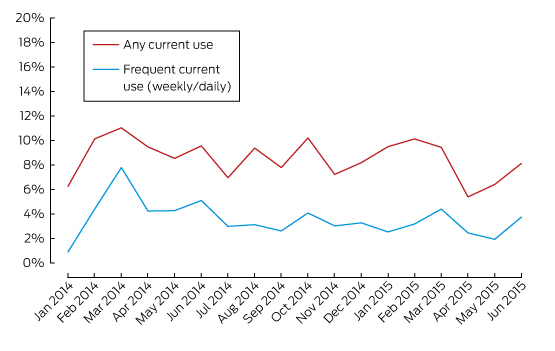
Over the 18 months, 254 respondents reported any current use of e-cigarettes (9% of the sample; 95% CI, 7–10%). Ninety-eight respondents used them less often than monthly, 52 used them monthly, 38 weekly, and 66 daily; that is, infrequent use was more common (57%; 95% CI, 50–64%) than frequent use (43%; 95% CI, 36–49%). Box 2 shows monthly rates of use; trend analyses found no changes in rates of any use (χ2 test for linear trend: P = 0.287) or frequent use (P = 0.130).
Box 3 shows the results of logistic regression analyses predicting e-cigarette use on the basis of demographic and smoking characteristics. Sixteen percent of younger adults (18–29 years) reported being current e-cigarette users; both mid-aged and older adults were less likely to be current users than younger adults (each, P < 0.001). Current smokers were more likely to be users than recent quitters (adjusted odds ratio [aOR], 1.55; P = 0.039). Mid-aged and older users were more likely to be frequent users than younger adults (55 years and older v 18–29 years: aOR, 4.43; P = 0.002), and current smokers were less likely than recent quitters to be frequent users (aOR, 0.38; P = 0.020).
Reasons for using e-cigarettes are shown in Box 4. The most common were “to help me quit smoking” (32%) and “to cut down on the number of cigarettes I smoke” (26%). Frequent users were significantly more likely than infrequent users to report that they used e-cigarettes to help them cut down (P = 0.002). Older users were more likely than younger users to report that they were using e-cigarettes to quit or cut down (each, P < 0.001). Smokers were significantly more likely than quitters to be using e-cigarettes to cut down (P = 0.002). The most common “other” reason for using e-cigarettes was curiosity or novelty (eg, “just to try it”), offered by 18 respondents.
Box 5 summarises responses regarding places of purchase for e-cigarette users’ most recent cartridge or vial. The most common sources were over the internet (29%) and tobacconists (27%), with a small proportion purchasing from convenience stores or petrol stations (8%). A large proportion of respondents did not know from where their last vial came (13%) or named a type of outlet specifically mentioned by less than 2% of respondents (23%). Frequent e-cigarette users were significantly more likely to have purchased over the internet than infrequent users (P < 0.001). There were no significant differences in places of purchase according to age or smoking status.
Discussion
This study is one of the first to explore patterns of e-cigarette use among tobacco smokers and recent quitters in Australia. Current use of e-cigarettes was reported by 9% of the sample, comparable with the 7% reported by the 2013 Australian ITC.12 Despite the fact that e-cigarette companies are currently prohibited from marketing their products as cessation aids (as none are approved by the TGA), the results of this study suggest that tobacco smokers are principally using e-cigarettes to help them quit. Clinicians and cessation services should be aware of smokers’ interest in e-cigarettes as cessation aids; the most recent guidance from the NHMRC encourages consumers to seek further information about e-cigarettes from reliable sources, including their general practitioner.8
Despite the fact that many e-cigarette users reported using them to assist quitting, most users in this sample were dual users, continuing to use conventional cigarettes as well as e-cigarettes. Many reported that they used e-cigarettes to cut down on the number of cigarettes they smoked. For avoiding the risks of smoking-related premature death, however, reducing cigarette numbers is much less effective than quitting,22 and future research should investigate whether tobacco smokers using e-cigarettes to cut down are doing so as part of a cessation strategy or in the hope of reducing smoking-related harm.
In this study, the rate of current e-cigarette use was highest (16%) among people aged 18–29 years. Younger users were more likely than older users to use e-cigarettes infrequently, and they were less likely than older users to use them to help quit or cut down on cigarettes. Future research should monitor patterns of use in this group to determine whether patterns of dual use persist, or if e-cigarettes have a role to play in cessation by young tobacco smokers.
In NSW, e-cigarettes are not currently covered by the Smoke-free Environment Act 2000.23 Concern has been expressed by some commentators that using e-cigarettes in smoke-free public places might diminish the impact of smoke-free policies on smoking rates by reducing the incentive for smokers to quit and by re-normalising smoking.7 In our study, about 10% of e-cigarette users reported that they used them to circumvent smoking restrictions in public places. Future research should monitor e-cigarette use in smoke-free environments, as well any impact this has on smokers’ quitting motivations.
The current study provides the first evidence about places where Australian tobacco smokers purchase their e-cigarettes. Infrequent users were more likely than frequent users to have obtained e-cigarettes in commonly visited retail environments, such as tobacconists or small retailers. There were no restrictions on the display and promotion of e-cigarettes in those retail environments at the time of this study, but recently passed amendments to the NSW Public Health (Tobacco) Act17 include such a ban. Investigating changes in how smokers purchase and use e-cigarettes following the implementation of this policy will be important. Frequent users were more likely than infrequent users to purchase e-cigarettes over the internet. An increase in internet advertising for e-cigarettes has been noted,24 but the extent to which Australian smokers are exposed to these advertisements — and their impact on beliefs about and the use of e-cigarettes — is still unknown. The large proportion of users purchasing their e-cigarettes online means that they have access to an almost unrestricted market. Although e-cigarettes sold in Australia cannot legally contain nicotine, the availability of nicotine-containing e-cigarettes online poses a complex challenge for enforcing supply regulations, making initiatives focused on educating consumers particularly important.
This study did not assess whether individuals were using nicotine-containing e-cigarettes; ITC data show that 21% of Australian e-cigarette users did not know whether their brand contained nicotine or not.12 Future research on e-cigarette use in Australia should explore whether patterns of use and reasons for using nicotine- and non-nicotine-containing e-cigarettes differ. It should be noted that no data were collected on whether some smokers transitioned from using e-cigarettes to smoking tobacco, another pattern that should be monitored in an Australian sample. The e-cigarette users in this study were likely to reflect the prevalence of e-cigarette use in this community, but the low overall prevalence limited our ability to undertake some subgroup analyses.
Strengths of this study include our use of recent data, with a large and representative sample of tobacco smokers and recent quitters. The inclusion of mobile phones in the sampling method helped minimise concerns about sampling bias. This study expands the knowledge base provided by a recent report from NSW13 by monitoring changes in e-cigarette use over an 18-month period, including data on e-cigarette use among recent quitters. This delivers detailed data on the frequency of e-cigarette use among users, and we explored reasons for using e-cigarettes as well as places of purchase.
Although overall use of e-cigarettes in NSW remains low, this study highlights problems related to higher rates of use among younger people, dual use of e-cigarettes and tobacco, and the use of e-cigarettes to cut down or quit tobacco cigarettes. The use of e-cigarettes by tobacco smokers attempting to reduce harm means that physicians, cessation services and public health authorities should be aware of tobacco smokers’ interest in e-cigarettes for harm reduction, inform smokers that e-cigarettes are currently unregulated and untested as cessation aids,8 and continue to provide evidence-based recommendations to smokers wanting to quit.
Box 1 – Characteristics of the 2966 participants in the Cancer Institute Tobacco Tracking Survey (CITTS), January 2014 – June 2015
Number (unweighted) |
Percentage (weighted*) |
||||||||||||||
Sex |
|||||||||||||||
Women |
1324 |
51% |
|||||||||||||
Men |
1642 |
49% |
|||||||||||||
Age |
|||||||||||||||
18–29 years |
638 |
22% |
|||||||||||||
30–55 years |
1391 |
44% |
|||||||||||||
≥ 55 years |
937 |
34% |
|||||||||||||
Education |
|||||||||||||||
Low |
743 |
26% |
|||||||||||||
Moderate |
1467 |
50% |
|||||||||||||
High |
726 |
24% |
|||||||||||||
Region |
|||||||||||||||
Non-metropolitan |
1182 |
39% |
|||||||||||||
Metropolitan |
1784 |
61% |
|||||||||||||
Socio-economic status |
|||||||||||||||
Low |
1015 |
35% |
|||||||||||||
Moderate or high |
1951 |
65% |
|||||||||||||
Smoking Status |
|||||||||||||||
Recent quitter |
524 |
18% |
|||||||||||||
Current smoker |
2442 |
82% |
|||||||||||||
Smoking frequency† |
|||||||||||||||
Less than daily |
335 |
13% |
|||||||||||||
Daily |
2107 |
87% |
|||||||||||||
Heaviness of Smoking Index score† |
|||||||||||||||
Low |
791 |
33% |
|||||||||||||
Moderate |
1021 |
44% |
|||||||||||||
High |
561 |
24% |
|||||||||||||
* Percentages are weighted for telephone status, age, sex, and regional residence. † Indicator available only for smokers. | |||||||||||||||
Box 2 – Prevalence of e-cigarette use among 2966 participants in the Cancer Institute Tobacco Tracking Survey (CITTS), in New South Wales, January 2014 – June 2015 (tobacco smokers and quitters)
Box 3 – Patterns of e-cigarette use and results of multivariable logistic regression analyses predicting any use and frequent use
|
Current e-cigarette use (n = 2947) |
Frequency of use (n = 254) |
||||||||||||||
No use |
Any use |
aOR (95% CI) |
P |
Infrequent |
Frequent |
aOR (95% CI) |
P |
||||||||
Total number |
2693 |
254 |
150 |
104 |
|||||||||||
Sex |
|||||||||||||||
Women |
93% |
7% |
1 |
55% |
45% |
1 |
|||||||||
Men |
90% |
10% |
1.22 (0.91–1.64) |
0.185 |
60% |
40% |
0.90 (0.50–1.61) |
0.719 |
|||||||
Age |
|||||||||||||||
18–29 years |
84% |
16% |
1 |
70% |
30% |
1 |
|||||||||
30–55 years |
92% |
8% |
0.48 (0.35–0.66) |
< 0.001 |
54% |
46% |
1.92 (0.99–3.71) |
0.053 |
|||||||
≥ 55 years |
96% |
4% |
0.24 (0.16–0.36) |
< 0.001 |
35% |
65% |
4.43 (1.69–11.62) |
0.002 |
|||||||
Education |
|||||||||||||||
Low |
93% |
7% |
1 |
56% |
44% |
1 |
|||||||||
Moderate |
91% |
9% |
1.02 (0.70–1.50) |
0.903 |
59% |
41% |
1.13 (0.43–2.98) |
0.809 |
|||||||
High |
90% |
10% |
1.21 (0.78–1.87) |
0.399 |
56% |
44% |
1.16 (0.40–3.35) |
0.784 |
|||||||
Region |
|||||||||||||||
Non-metropolitan |
93% |
7% |
1 |
57% |
43% |
1 |
|||||||||
Metropolitan |
91% |
9% |
1.32 (0.97–1.81) |
0.078 |
58% |
42% |
0.81 (0.41–1.60) |
0.546 |
|||||||
Socio-economic status |
|||||||||||||||
Low |
91% |
9% |
1 |
59% |
41% |
1 |
|||||||||
Moderate or high |
92% |
8% |
0.78 (0.57–1.06) |
0.109 |
56% |
44% |
1.25 (0.67–2.33) |
0.484 |
|||||||
Smoking status |
|||||||||||||||
Recent quitter |
93% |
7% |
1 |
35% |
65% |
1 |
|||||||||
Current smoker |
91% |
9% |
1.55 (1.02–2.36) |
0.039 |
61% |
39% |
0.38 (0.16–0.86) |
0.020 |
|||||||
Smoking frequency* |
|||||||||||||||
Less than daily |
89% |
11% |
1 |
81% |
19% |
1 |
|||||||||
Daily |
91% |
9% |
1.14 (0.71–1.83) |
0.586 |
57% |
43% |
2.31 (0.79–6.75) |
0.125 |
|||||||
Heaviness of Smoking Index score* |
|||||||||||||||
Low |
90% |
10% |
1 |
63% |
37% |
1 |
|||||||||
Moderate |
91% |
9% |
1.19 (0.79–1.77) |
0.404 |
60% |
40% |
0.79 (0.35–1.76) |
0.561 |
|||||||
High |
94% |
6% |
0.83 (0.51–1.34) |
0.442 |
54% |
46% |
1.02 (0.40–2.59) |
0.970 |
|||||||
aOR = adjusted odds ratio. Multivariable logistic regression Model 1 included demographic factors (sex, age, education, socio-economic status) and smoking status; Model 2 also included smoking frequency and Heaviness of Smoking Index score. * Results from Model 2 for the smoker sample only; all other results are for Model 1. | |||||||||||||||
Box 4 – Reasons for using e-cigarettes given by 218 tobacco smokers and 36 recent quitters in New South Wales
To help me quit smoking |
To cut down on the number of cigarettes I smoke |
Not as bad for your health as cigarettes |
So I can smoke where smoking cigarettes is not allowed |
Taste better than cigarettes |
Cheaper than cigarettes |
||||||||||
Total (n = 254) |
32% (26–39%) |
26% (21–33%) |
20% (15–26%) |
11% (8–16%) |
7% (4–12%) |
8% (5–13%) |
|||||||||
Frequency of use |
|||||||||||||||
Infrequent (n = 150) |
28% (21– 37%) |
19% (13–27%) |
20% (14–28%) |
15% (10–21%) |
9% (5–15%) |
10% (6–17%) |
|||||||||
Frequent (n = 104) |
37% (28–48%) |
36% (27–47%) |
20% (13–30%) |
7% (3–15%) |
5% (2–12%) |
6% (3–12%) |
|||||||||
P (χ2 test) |
0.088 |
0.002 |
0.525 |
0.060 |
0.141 |
0.170 |
|||||||||
Age |
|||||||||||||||
18–29 years (n = 99) |
18% (11–28%) |
14% (9–23%) |
25% (17–36%) |
14% (8–23%) |
13% (7–22%) |
9% (4–16%) |
|||||||||
30–54 years (n = 155) |
42% (34–50%) |
35% (27–43%) |
16% (11–23%) |
10% (6–16%) |
3% (1–9%) |
8% (4–14%) |
|||||||||
P (χ2 test) |
< 0.001 |
< 0.001 |
3.49 (0.045) |
0.229 |
0.005 |
0.486 |
|||||||||
Smoking status |
|||||||||||||||
Recent quitter (n = 36) |
36% (21–54%) |
6% (2–18%) |
36% (20–56%) |
7% (1–27%) |
12% (4–33%) |
15% (6–32%) |
|||||||||
Smoker (n = 218) |
32% (25–39%) |
30% (23–37%) |
17% (13–23%) |
12% (8–17%) |
6% (4–11%) |
7% (4–12%) |
|||||||||
P (χ2 test) |
0.397 |
0.002 |
0.018 |
0.233 |
0.214 |
0.116 |
|||||||||
Percentages are weighted for telephony status, age, sex, and regional residence; 95% CIs are given in parentheses. Bonferroni-adjusted P < 0.003 defined as statistically significant. | |||||||||||||||
Box 5 – Places of purchase for e-cigarette liquids and vials for e-cigarette users in New South Wales
Tobacconist |
Internet |
Convenience store or petrol station |
Other or “don’t know” |
||||||||||||
Total (n = 254) |
27% (22–33%) |
29% (23–35%) |
8% (5–12%) |
23% (18–29%) |
|||||||||||
Frequency of use |
|||||||||||||||
Infrequent (n = 150) |
27% (20–35%) |
17% (12–25%) |
12% (7–19%) |
24% (18–32%) |
|||||||||||
Frequent (n = 104) |
28% (19–38%) |
44% (33–54%) |
3% (1–7%) |
21% (14–31%) |
|||||||||||
P (χ2 test) |
0.480 |
< 0.001 |
0.006 |
0.356 |
|||||||||||
Age |
|||||||||||||||
18–29 years (n = 99) |
28% (19–38%) |
23% (14–34%) |
11% (6–19%) |
24% (16–34%) |
|||||||||||
30–54 years (n = 155) |
27% (20–35%) |
33% (25–41%) |
6% (3–11%) |
22% (16–30%) |
|||||||||||
P (χ2 test) |
0.508 |
0.070 |
0.124 |
0.435 |
|||||||||||
Smoking status |
|||||||||||||||
Recent quitter (n = 36) |
27% (14–45%) |
29% (5–47%) |
8% (2–27%) |
19% (9–36%) |
|||||||||||
Smoker (n = 218) |
27% (21–34%) |
29% (22–36%) |
8% (5–12%) |
23% (18–30%) |
|||||||||||
P (χ2 test) |
0.584 |
0.517 |
0.514 |
0.345 |
|||||||||||
Percentages are weighted for telephony status, age, sex, and regional residence; 95% CIs are given in parentheses. Bonferroni-adjusted P < 0.004 defined as statistically significant. | |||||||||||||||
Received 16 October 2015, accepted 17 February 2016
- Sally Dunlop1
- Claudine Lyons2
- Anita Dessaix1
- David Currow1
- 1 Cancer Institute NSW, Sydney, NSW
- 2 Department of Premier and Cabinet, NSW Government, Sydney, NSW
No relevant disclosures.
- 1. Denmick B. A high-tech approach to getting a nicotine fix. Los Angeles Times 2009; 25 Apr. http://articles.latimes.com/2009/apr/25/world/fg-china-cigarettes25 (accessed July 2015).
- 2. McMillen RC, Gottlieb MA, Shaefer RM, et al. Trends in electronic cigarette use among US adults: use is increasing in both smokers and nonsmokers. Nicotine Tob Res 2014; 17: 1195-1202.
- 3. Vardavas CI, Filippidis FT, Agaku IT. Determinants and prevalence of e-cigarette use throughout the European Union: a secondary analysis of 26 566 youth and adults from 27 countries. Tob Control 2014; 24: 442-448.
- 4. Etter JF. Should electronic cigarettes be as freely available as tobacco? Yes. BMJ 2013; 346: f3845.
- 5. Gartner CE, Hall WD, Borland R. How should we regulate smokeless tobacco products and e-cigarettes? Med J Aust 2012; 197: 611-612. <MJA full text>
- 6. Grana R, Benowitz N, Glantz SA. E-cigarettes: a scientific review. Circulation 2014; 129: 1972-1986.
- 7. Chapman S. Should electronic cigarettes be as freely available as tobacco cigarettes? No. BMJ 2013; 346: f3840.
- 8. Australian National Health and Medical Research Council. NHMRC CEO statement: Electronic cigarettes (e-cigarettes). Mar 2015. http://www.nhmrc.gov.au/_files_nhmrc/publications/attachments/ds13_nhmrc_ceo_statement_ecigarettes.pdf (accessed July 2015).
- 9. Biener L, Hargraves JL. A longitudinal study of electronic cigarette use among a population-based sample of adult smokers: association with smoking cessation and motivation to quit. Nicotine Tob Res 2015; 17: 127-133.
- 10. Brown J, West R, Beard E, et al. Prevalence and characteristics of e-cigarette users in Great Britain: findings from a general population survey of smokers. Addict Behav 2014; 39: 1120-1125.
- 11. Glantz SA. Meta-analysis of all available population studies continues to show smokers who use e-cigs less likely to quit smoking [website]. 15 Mar 2015. http://tobacco.ucsf.edu/meta-analysis-all-available-population-studies-continues-show-smokers-who-use-e-cigs-less-likely-quit-smoking (accessed July 2015).
- 12. Yong HH, Borland R, Balmford J, et al. Trends in e-cigarette awareness, trial, and use under the different regulatory environments of Australia and the United Kingdom. Nicotine Tob Res 2014; 17: 1203-1211.
- 13. Harrold TC, Maag AK, Thackway S, et al. Prevalence of e-cigarette users in New South Wales. Med J Aust 2015; 203: 326. <MJA full text>
- 14. World Health Organization Framework Convention on Tobacco Control. Electronic nicotine delivery systems. (FCTC/COP/6/10) [report]. 21 July 2014. http://apps.who.int/gb/fctc/PDF/cop6/FCTC_COP6_10-en.pdf?ua=1 (accessed July 2015).
- 15. Australian Government. Department of Health, Therapeutic Goods Administration. Poisons standard July 2015. https://www.comlaw.gov.au/Details/F2015L00844 (accessed July 2015).
- 16. New South Wales Government. Poisons and Therapeutic Goods Regulation 2008. Part 2: Poisons. http://www.legislation.nsw.gov.au/fullhtml/inforce/subordleg+392+2008+FIRST+0+N#pt.2 (accessed July 2015).
- 17. New South Wales Government. Public Health (Tobacco) Act 2008 No 94. http://www.legislation.nsw.gov.au/#/view/act/2008/94/full (accessed July 2015).
- 18. Australian Bureau of Statistics. 2006 census of population and housing: Socio-economic indexes for area’s (SEIFA). http://www.abs.gov.au/websitedbs/censushome.nsf/home/seifa2011?opendocument&navpos=260 (accessed July 2015).
- 19. Heatherton TF, Kozlowski L, Frecker RC, et al. Measuring the heaviness of smoking: using self-reported time to the first cigarette of the day and number of cigarettes smoked per day. Br J Addict 1989; 84: 791-799.
- 20. Li J, Newcombe R, Walton D. The prevalence, correlates and reasons for using electronic cigarettes among New Zealand adults. Addict Behav 2015; 45: 245-251.
- 21. Australian Bureau of Statistics. 3201.0. Population by age and sex, Australian states and territories, June 2010. Dec 2010. http://www.abs.gov.au/ausstats/abs@.nsf/PrimaryMainFeatures/3201.0?OpenDocument (accessed July 2015).
- 22. US Department of Health and Human Services. The health consequences of smoking — 50 years of progress: a report of the Surgeon General. Executive summary. Atlanta: US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, 2014. http://www.surgeongeneral.gov/library/reports/50-years-of-progress/exec-summary.pdf (accessed July 2015).
- 23. New South Wales Government. Smoke-free Environment Act 2000 No 69. http://www.legislation.nsw.gov.au/#/view/act/2000/69/full (accessed July 2015).
- 24. Richardson A, Ganz O, Vallone D. Tobacco on the web: surveillance and characterisation of online tobacco and e-cigarette advertising. Tob Control 2014; 24: 341-347.
Abstract
Objectives: To explore how and why tobacco smokers and recent quitters in NSW use e-cigarettes, as well as common places of purchase.
Design: The Cancer Institute Tobacco Tracking Survey is a serial cross-sectional telephone survey, with 40 interviews in NSW each week.
Participants: 2966 tobacco smokers and recent quitters (in the past 12 months) interviewed January 2014 – June 2015.
Measures: Current e-cigarette use; reasons for using; places of purchase.
Results: 9% of the sample reported currently using e-cigarettes; the rate was highest among 18–29-year-old people (16%). Infrequent use (less than weekly; 57%) was more common than frequent use (at least weekly; 43%). Frequent use was more likely among older adults (55 years and older v 18–29 years: adjusted odds ratio [aOR], 4.43; P = 0.002) and less likely among current tobacco smokers (v recent quitters: aOR, 0.38, P = 0.020). The most common reasons for using e-cigarettes by those over 30 years of age was “to help me quit” (42%) and to “cut down” smoking (35%); for younger adults it was “because they are not as bad for your health as cigarettes” (25%). Common places of purchase were the internet (29%) and tobacconists (27%).
Conclusions: Although use of e-cigarettes by tobacco smokers in NSW remains low, some are using e-cigarettes in attempts to reduce tobacco-related harm. Physicians and public health campaigners should inform smokers about the risks associated with dual e-cigarette and tobacco use, advise interested quitters that e-cigarettes are currently unregulated as cessation aids, and continue to provide evidence-based recommendations and cessation services to smokers wanting to quit.