





Medical education
Lessons from practice
Volume 218 - Issue 6
Abdominal pain secondary to bilateral adrenal haemorrhage as the first presentation of antiphospholipid syndrome
Authors: Eugene Wang, Rithin Nedumannil and Max Wolf
Med J Aust 2023; 218 (6): 250-251. || doi: 10.5694/mja2.51874
Published online: 3 April 2023
Published online: 3 April 2023
Clinical record
A 39‐year‐old man presented to the emergency department with a three‐day history of anorexia and severe abdominal pain, which was worse in the right lower quadrant. He had an upper respiratory tract viral infection two weeks before this presentation. Past medical history was significant for mixed connective tissue disease, which was diagnosed 27 years ago and was being monitored. On examination, he was afebrile and normotensive, and demonstrated generalised abdominal distension, guarding and tenderness on palpation. Investigations showed normocytic anaemia with haemoglobin 103g/L (reference interval [RI], 130–180g/L) and marked neutropenia 0.5×109/L (RI, 2.0–7.5×109/L). He had an elevated C‐reactive protein at 391mg/L (RI, <5mg/L) and a prolonged activated partial thromboplastin time (APTT) of 44 seconds (RI, 23–33 seconds) that did not correct on mixing studies.
Computed tomography (CT) scan of the abdomen revealed a thickened appendix and enlarged adrenal glands bilaterally with prominent peri‐adrenal retroperitoneal fat stranding, suggestive of bilateral adrenal haemorrhage (Box) and probable appendicitis. On the basis of worsening right lower quadrant pain, elevated inflammatory markers, and CT findings, a laparoscopic appendicectomy was performed. Intra‐operatively, a thickened appendix was visualised with no macroscopic features of appendicitis. Histopathology of the appendix confirmed inflammation of the appendiceal serosa without mucosal involvement, reflective of extra‐appendiceal inflammation due to separate intra‐abdominal pathology rather than appendicitis.
Following exclusion of acute appendicitis as the cause of abdominal pain, further tests were ordered given the associated neutropenia, prolonged APTT, and history of autoimmune disease. These tests confirmed the presence of lupus anticoagulant, as well as anticardiolipin IgG antibodies 111GPL‐U/mL (RI, <10GPL‐U/mL) and anti‐β‐2‐glycoprotein IgG antibodies 89U/mL (RI, <7U/mL). Antinuclear antibody was detected in a homogeneous pattern with a titre of 1:320, and anti‐double stranded DNA antibodies were negative. Despite the absence of previous thrombosis, these clinicopathological features were consistent with triple‐positive antiphospholipid syndrome (APS) and bilateral adrenal haemorrhage. Although he was normotensive and had normal sodium levels, the patient had reduced morning cortisol, elevated adrenocorticotropic hormone, and lack of cortisol response to a short synacthen test, thus confirming primary adrenal insufficiency. The patient was started on hydrocortisone 20mg thrice daily and long term warfarin with bridging enoxaparin, following which his abdominal pain resolved and he was subsequently discharged without experiencing complications of anticoagulation.
Discussion
APS is an autoimmune disease characterised by the presence of antiphospholipid antibodies, which can bind to β‐2‐glycoprotein I, resulting in the upregulation of prothrombotic molecules and activation of complement and neutrophils.1,2 These all contribute to an increased risk of arterial and venous thrombosis. APS can occur as a primary disease or secondary to autoimmune conditions such as systemic lupus erythematosus. The most common clinical presentations of APS are deep venous thrombosis, ischaemic stroke, and obstetric complications such as recurrent miscarriages.2 Lifelong warfarin is recommended for thrombosis prevention in patients with APS with previous thrombotic events.1,3
A rare complication of APS is adrenal vein thrombosis and subsequent bilateral adrenal haemorrhage. Due to each adrenal gland having a triplex arterial supply but only one draining vein, the hypercoagulable state of APS predisposes the adrenal glands to developing venous thrombosis and secondary haemorrhagic infarction.4 This will usually present as abdominal pain with signs of primary adrenal insufficiency, which can be life‐threatening. Bilateral adrenal haemorrhage resulting in primary adrenal insufficiency is the most common endocrine manifestation of APS, despite occurring in only 0.4% of APS cases.4
This patient presented with abdominal pain mimicking acute appendicitis and no symptoms of primary adrenal insufficiency, which initially masked the bilateral adrenal haemorrhage. No previous history of thrombosis also made the diagnosis of APS challenging. Although uncommon, there have been reports of bilateral adrenal haemorrhage as the first presentation of APS.4,5 It is possible that the patient's recent antecedent viral illness triggered his initial thrombotic manifestation of APS. Prolonged APTT without correction upon mixing and unexplained neutropenia are important clues for APS, which should prompt further diagnostic APS investigations and a CT scan in the setting of abdominal pain to examine the adrenal glands for abnormality. This case highlights the significance of suspecting visceral thrombosis secondary to APS in those with otherwise unexplained abdominal pain and a history of autoimmune disease, even in the absence of previous thrombotic events. In patients with adrenal haemorrhage secondary to APS, close monitoring for development of primary adrenal insufficiency is essential, even in the absence of typical symptoms or signs. Likewise, bilateral adrenal haemorrhage secondary to APS should be considered in patients with signs of adrenal insufficiency, after excluding common causes such as autoimmune adrenalitis.4
Lessons from practice
- Arterial or venous thrombosis and pregnancy complications such as recurrent miscarriages and pre‐eclampsia are classic manifestations of antiphospholipid syndrome (APS).
- Bilateral adrenal haemorrhage can be the first thrombotic presentation of APS and is challenging to diagnose in this patient population.
- APS and associated bilateral adrenal haemorrhage should be suspected in patients with a history of autoimmune disease who present with abdominal pain.
- Primary adrenal insufficiency can be asymptomatic and screening for this condition should be considered in all patients with known adrenal gland pathology.
Box – Computed tomography (CT) scan of the abdomen and pelvis with contrast demonstrating bilateral adrenal haemorrhage and thickened appendix
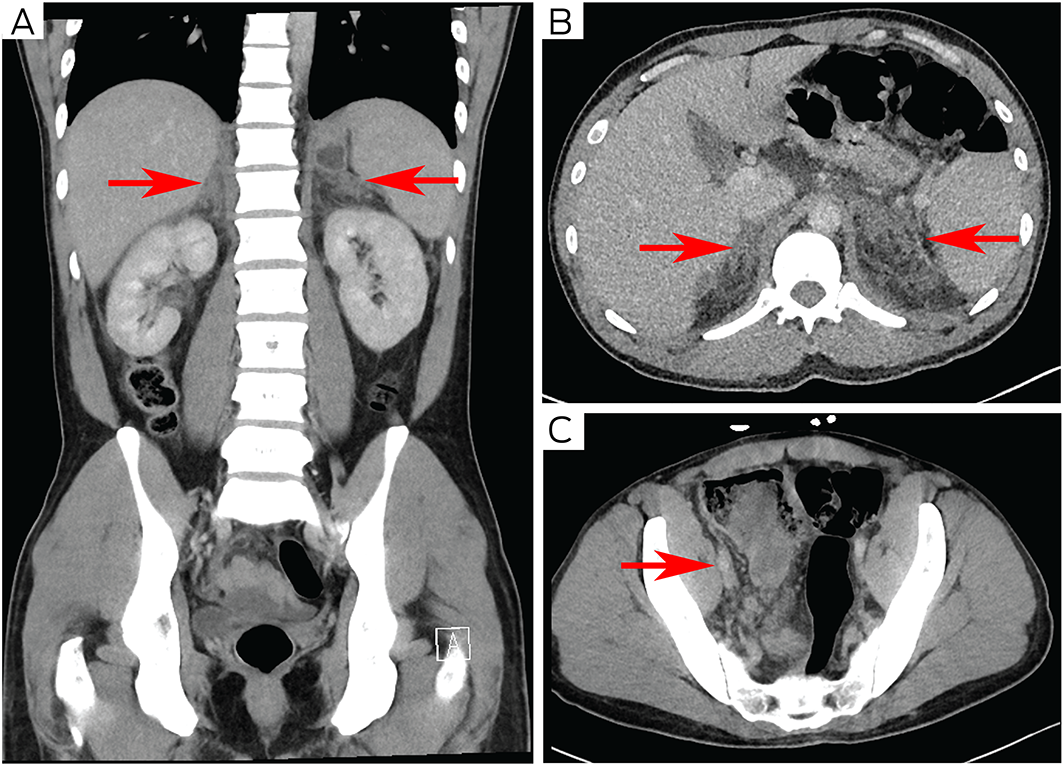
(A and B) Coronal and axial CT showing bulky adrenal glands with prominent retroperitoneal fat stranding (arrows). (C) Axial CT showing thickened appendix (arrow).
Competing interests
No relevant disclosures.
References
- Garcia D, Erkan D. Diagnosis and management of the antiphospholipid syndrome. N Engl J Med 2018; 378: 2010‐2021.
- Schreiber K, Sciascia S, de Groot PG, et al. Antiphospholipid syndrome. Nat Rev Dis Primers 2018; 4: 17103.
- Mezhov V, Segan JD, Tran H, Cicuttini FM. Antiphospholipid syndrome: a clinical review. Med J Aust 2019; 211: 184‐188. https://www.mja.com.au/journal/2019/211/4/antiphospholipid‐syndrome‐clinical‐review
- Presotto F, Fornasini F, Betterle C, et al. Acute adrenal failure as the heralding symptom of primary antiphospholipid syndrome: report of a case and review of the literature. Eur J Endocrinol 2005; 153: 507‐514.
- Khare S, Patel H, Sutaria G, Sharma R. Primary antiphospholipid antibody syndrome presenting as unilateral adrenal hemorrhage. Indian J Endocrinol Metab 2017; 21: 932‐933.
Provenance: Not commissioned; externally peer reviewed.