





Volume 217 - Issue 1
Tattoo sarcoidosis presenting as abdominal allodynia
Authors: Annabelle Faint and A James M Daveson
Med J Aust 2022; 217 (1): 23-23. || doi: 10.5694/mja2.51603
Published online: 4 July 2022
Published online: 4 July 2022
A 40-year-old man was referred with left- sided abdominal pain radiating across his abdomen, arthralgias and a mild ileitis endoscopically
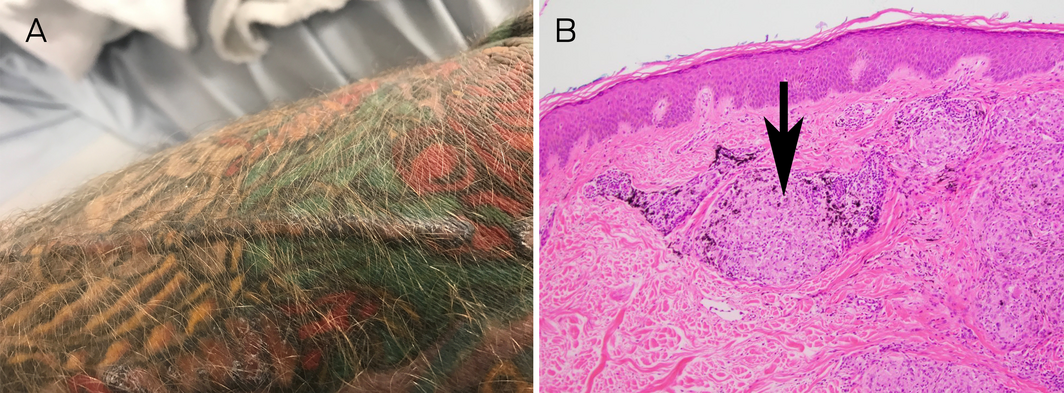
A 40‐year‐old man was referred with left‐sided abdominal pain (described as “like broken‐glass”) radiating across his abdomen, arthralgias and a mild ileitis endoscopically (not histologically). Clinical examination revealed abdominal allodynia and a focally raised, firm and oedematous tattoo (Figure, A). Serum angiotensin converting enzyme (ACE) was 71IU/L (reference interval [RI], 20–70IU/L) and ACE mass was 248μg/L (RI, 37–211μg/L). A biopsy of the affected tattoo revealed extensive granulomatous dermal inflammation with well defined “naked” tubercles. Polarisation showed a minute amount of exogenous material superficially, although most of the granulomata did not show refractile foreign material, consistent with cutaneous sarcoidosis (Figure, B). Subsequent investigations excluded inflammatory bowel disease. The pain and elevated tattoo resolved with oral corticosteroids (although it initially relapsed when withdrawn) and subsequently methotrexate 20mg weekly. Sarcoidal reactions to tattoos have been reported1 with abdominal pain related to small fibre neuropathies manifest by allodynia and hyperaesthesia.2 In one study of patients with cutaneous sarcoidosis treated with methotrexate, lesions completely resolved in 75% of patients.3 The prevailing hypothesis is that tattoo pigments provide chronic antigenic stimulation in genetically susceptible patients, leading to systematised granulomatous hypersensitivity.4,5
Competing interests
No relevant disclosures.
Acknowledgements
We acknowledge Dr Jill Magee from Sullivan Nicolaides Pathology, who assisted in the preparation and review of the histology.
References
- Antonovich DD, Callen JP. Development of sarcoidosis in cosmetic tattoos. Arch Dermatol 2005; 141: 869–872.
- Heij L, Dahan A, Hoitsma E. Sarcoidosis and pain caused by small‐fiber neuropathy. Pain Res Treat 2012; 2012: 256024.
- Veien NK, Brodthagen H. Cutaneous sarcoidosis treated with methotrexate. Br J Dermatol 1977; 97: 213–216.
- Post J, Hull P. Tattoo reactions as a sign of sarcoidosis. CMAJ 2012; 184: 432.
- Flynn J, Mithcell S, Wynne J. Tattoo‐induced sarcoidosis: a late rare tattoo parlour complication. Crit Care Med 2022; 50: 542.