




An emergency imaging pathway based on local and international guidance tailored to the Australian health care setting
Imaging in coronavirus disease 2019 (COVID‐19) is primarily helpful in diagnosing COVID‐19‐related complications and identifying alternative diagnoses that may explain a patient’s presentation.
It can also be useful in the risk stratification of patients by identifying the presence and severity of comorbidities.1,2 Imaging is of limited use in screening for COVID‐19 in asymptomatic individuals, and in many cases where COVID‐19 symptoms are mild.1,3 Indiscriminate use of imaging in patients with confirmed or suspected COVID‐19 not only exposes the patient to unnecessary radiation but also represents an unnecessary infection risk and logistic demand for medical imaging departments.
Existing international COVID‐19 imaging pathways have been derived in clinical environments significantly different from Australia, often where there is high COVID‐19 prevalence and constrained resource availability. Some centres preferentially use chest x‐ray, whereas others perform various types of computed tomography (CT) imaging of the chest. There is also inconsistency in the reporting of imaging studies in suspected or confirmed COVID‐19, with some reports following traditional didactic format, and others using synoptic template reports as recommended by a variety of medical bodies.4,5
Here we describe an imaging pathway developed at the Royal Adelaide Hospital, the designated COVID‐19 hospital in South Australia. This pathway aims to outline the imaging indications, technique and reporting of chest imaging in an emergency setting, at a time of low COVID‐19 prevalence. We incorporate current available international pathways and best practice guidelines for emergency imaging of COVID‐19 patients into a simple pathway relevant to Australian practice.
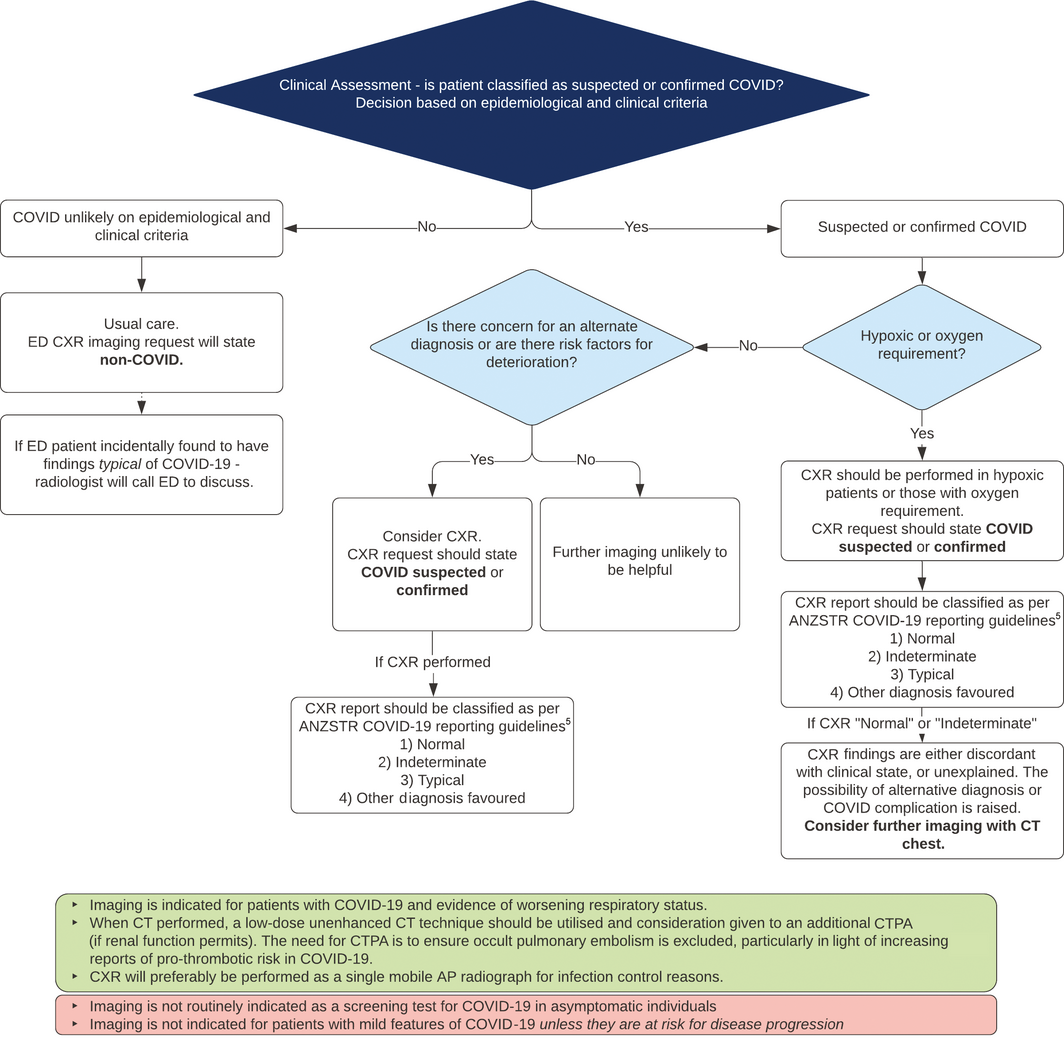
Imaging pathway development
We reviewed consensus and position statements from the Royal Australian and New Zealand College of Radiologists, the Australian and New Zealand Society of Thoracic Radiology, the Fleischner Society and the British Society of Thoracic Imaging. Recommendations pertaining to high COVID‐19 prevalence environments and resource‐constrained environments were modified to suit a scenario of low prevalence. When local guidelines conflicted with international organisations, priority was given to local recommendations on the basis of relevance. Recommendations were subsequently integrated into a clinical imaging pathway in consultation with local specialists in radiology, emergency medicine, general medicine, respiratory medicine and infectious diseases (Box).
Reporting terminology
The pathway incorporates standardised reporting terminology for patients with COVID‐19 as recommended by the Australian and New Zealand Society of Thoracic Radiology.5 Categorisation of study findings as “normal,” “indeterminate,” “typical” or “other diagnosis favoured” improves report clarity and creates actionable imaging outcomes.
Appropriate use of CT
The main role of CT in this pathway is to exclude complications and alternative diagnoses in patients with confirmed or suspected COVID‐19. The pathway prompts clinicians to consider CT for patients who are hypoxic (or have an oxygen requirement) and who have a chest x‐ray that is either “normal” or “indeterminate for COVID‐19”. In this instance there is a clinicoradiological discrepancy, and either a complication (such as a pulmonary embolus) or an alternative diagnosis is suspected.
In keeping with British Society of Thoracic Imaging guidance, a low‐dose unenhanced CT of the chest is the CT scan of choice, with strong consideration given to an additional CT pulmonary angiogram.4 There is accumulating evidence that patients with COVID‐19 are abnormally prothrombotic, and conventional clinical decision rules and blood tests (especially D‐dimer) may not be applicable.3 Clinicians should have a lower threshold than usual for performing a CT pulmonary angiogram. The unenhanced CT functions primarily as a baseline, as the presence of intravenous contrast can artifactually simulate ground glass. Whenever possible, the non‐contrast CT scan and the CT pulmonary angiogram should be performed on the same occasion to minimise infection control risk and operational demands on medical imaging departments.
Baseline imaging for patients at risk of deterioration
Patients with comorbidities are recognised as being at higher risk of deterioration. Defined risk factors vary between institutions but include older patients, requirement for oxygen supplementation, significant comorbidities (especially cardiac or respiratory) and immunosuppression. The consensus statement from the Fleischner Society supports imaging in patients who have a positive test result for COVID‐19 and risk factors for disease progression, regardless of their clinical status. The use of imaging in this situation is to establish a baseline for future comparison and determine the extent of comorbidities. Imaging may also inform the intensity of follow‐up monitoring, either in the community or an inpatient setting.1
Incidental findings suspicious for COVID‐19
Although there are no radiological findings pathognomonic for COVID‐19, there are radiological findings commonly associated with infection.5 When imaging findings typical for COVID‐19 are seen in a patient who is not suspected of having infection, the pathway prompts the radiologist to discuss the findings with the referring emergency physician. Patient isolation and COVID‐19 testing may be required. This is intended as a safety net for patients who may not be identified by current clinical screening processes, acknowledging that patients with COVID‐19 may be asymptomatic, may present with atypical symptoms and do not necessarily have knowledge of close contact with an infected individual.
Ultrasound
There is some evidence that point‐of‐care ultrasound can be used in the imaging of patients with COVID‐19; however, given variability in specialist expertise and availability, this has not been incorporated in this pathway.1
Conclusion
Chest imaging in suspected or confirmed COVID‐19 in a low prevalence environment is best used to detect complications and rule out alternative diagnoses. The pathway described here aims to clarify imaging indications, technique and reporting of studies performed on patients with suspected or confirmed COVID‐19 in an acute care setting.
Provenance: Not commissioned; externally peer reviewed.
- 1. Rubin GD, Ryerson CJ, Haramati LB, et al. The role of chest imaging in patient management during the COVID‐19 pandemic: a multinational consensus statement from the Fleischner Society. Chest 2020; 158: 106–116.
- 2. Royal Australian and New Zealand College of Radiologists. COVID‐19: position statements and guidance. COVID‐19 essential role of clinical radiology services. https://www.ranzcr.com/our-work/coronavirus/position-statements-and-guidance (viewed Apr 2020).
- 3. Royal Australian and New Zealand College of Radiologists. COVID‐19: position statements and guidance. Advice on appropriate use of CT throughout the COVID‐19 pandemic. 9 Apr 2020. https://www.ranzcr.com/our-work/coronavirus/position-statements-and-guidance (viewed Apr 2020).
- 4. Hare SS, Rodrigues JCL, Nair A, et al. The continuing evolution of COVID‐19 imaging pathways in the UK: a British Society of Thoracic Imaging expert reference group update. Clin Radiol 2020; 75: 399–404.
- 5. Royal Australian and New Zealand College of Radiologists. COVID‐19: position statements and guidance. Guidelines for CT chest and chest radiograph reporting in patients with suspected COVID‐19 infection. 24 Apr 2020. https://www.ranzcr.com/our-work/coronavirus/position-statements-and-guidance (viewed Apr 2020).
No relevant disclosures.