





Volume 214 - Issue 2
Rethinking pharmacological venous thromboembolism prophylaxis in minimally invasive gynaecological procedures
Authors: Esther MC Johns, Alex Ades and Pavitra Nanayakkara
Med J Aust 2021; 214 (2): 60-62.e1. || doi: 10.5694/mja2.50897
Published online: 1 February 2021
Published online: 1 February 2021
Although VTE risk in minor gynaecological procedures is low, a systematic approach to
prophylaxis is necessary
Although VTE risk in minor gynaecological procedures is low, a systematic approach to prophylaxis is necessary
Venous thromboembolism (VTE) is a rare but highly morbid risk of surgery that is largely preventable with appropriate prophylaxis.1,2 Methods of VTE prophylaxis range from conservative options with early ambulation, to mechanical compression devices used during and after surgery, to pharmacological prophylaxis with unfractionated or low molecular weight heparin. The current National Health and Medical Research Council guidelines, endorsed by the Royal Australian and New Zealand College of Gynaecologists, recommend the use of pharmacological prophylaxis for all gynaecological operations.1 However, this fails to acknowledge the difference in VTE risk in major versus minimally invasive surgeries. Indeed, the widely recognised international guidelines published by the American College of Obstetricians and Gynecologists and the American College of Chest Physicians incorporate both procedural (eg, mode of incision) and patient factors in the assessment of VTE risk.3,4 These guidelines encourage early ambulation or mechanical prophylaxis alone for very low and low risk patients, respectively, which largely includes those undergoing minimally invasive gynaecological procedures (with no additional risk factors).3,4 Further, a 2018 systematic review highlighted the very low risk of VTE in minimally invasive gynaecological surgeries, including laparoscopic and vaginal procedures, compared with open procedures. The review concluded that there is unlikely to be any additional benefit of pharmacological prophylaxis compared with mechanical prophylaxis alone in low risk patients.5 This is particularly relevant given the increased risk of haemorrhage associated with pharmacological VTE prophylaxis.6 Consequently, a 2020 Australian Commission on Safety and Quality in Health Care report acknowledged that there is no consensus among evidence‐based guidelines regarding the preferred method of VTE assessment, and clinicians and institutions should refer to the evidence‐based VTE risk assessment tool of their choosing.7 We sought to evaluate the risk of VTE in minimally invasive gynaecological procedures and determine the need for pharmacological prophylaxis in addition to mechanical prophylaxis.
Minor gynaecological surgery carries lower VTE risk
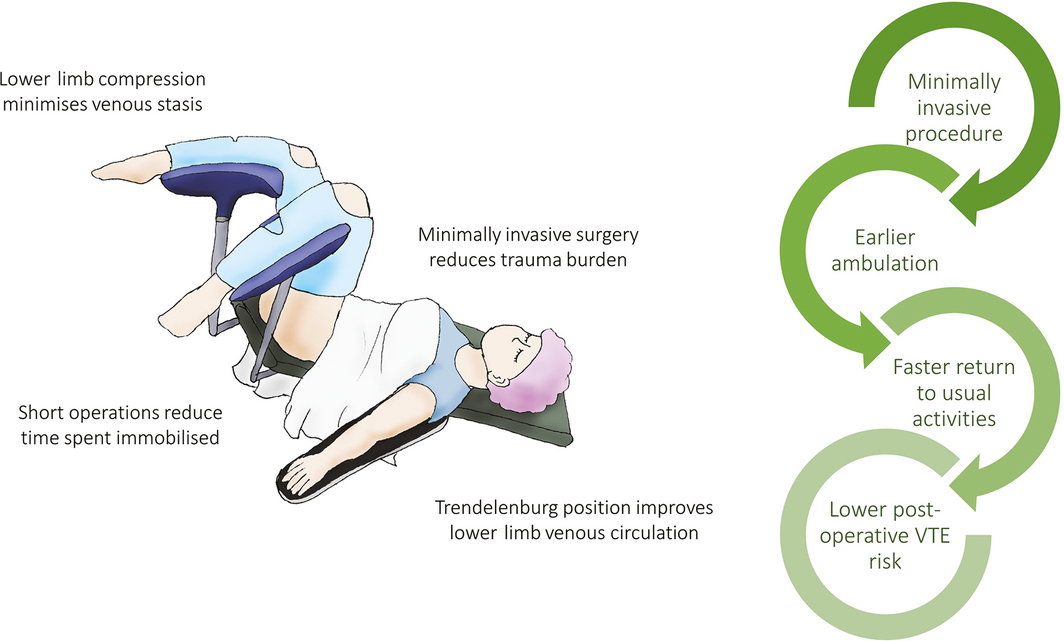
Minor gynaecological surgery conducted via the laparoscopic or vaginal route carries a lower risk of VTE than open surgery.8,9,10,11 Indeed, a large prospective cohort study of 89 931 women undergoing hysterectomy for a benign indication demonstrated a twofold risk of VTE in the group undergoing laparotomy compared with those undergoing laparoscopic or vaginal procedures.11 Moreover, a small, prospective, multicentre cohort study of 266 women undergoing laparoscopies for minor conditions such as endometriosis, ovarian cysts and infertility found no cases of VTE in the 30 days following the procedure in the absence of any VTE prophylaxis.8 Consequently, it is not appropriate to consider all types of gynaecological surgery together when discussing their associated VTE risk. The reasons for this discrepancy are thought to be associated with the characteristics of the patients being generally younger and healthier, in addition to factors such as short procedural duration, limited trauma burden, faster recovery resulting in early ambulation and short hospital stay, as well as positioning of the patient on the operating table in the Trendelenburg or lithotomy position, which limits pooling of blood in the calves.2,5 Given the lower risk of VTE under these minimally invasive conditions, it is important to consider whether there is indeed a need for pharmacological, in addition to mechanical, prophylaxis (Box 1).
Pharmacological VTE prophylaxis offers no additional benefit to mechanical prophylaxis in low risk patients
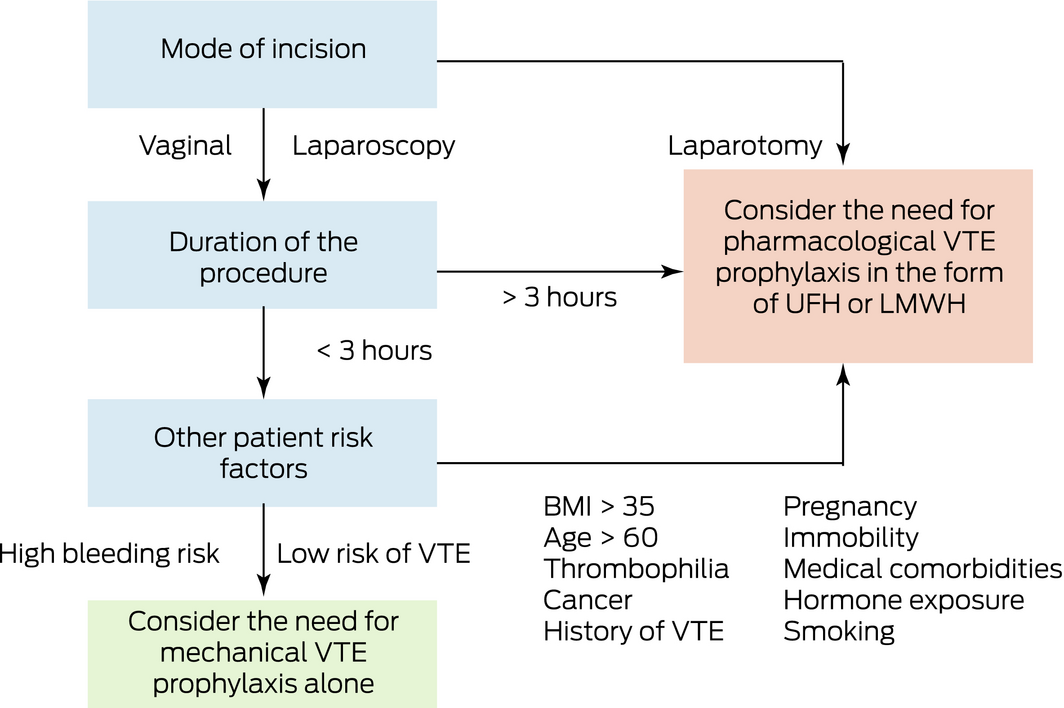
The importance of VTE prophylaxis during and after surgery is well recognised, with most hospitals subscribing to a VTE prophylaxis protocol. The use of mechanical prophylaxis during and after surgery in the form of sequential compression devices and graduated compression stockings has been shown to halve the risk of VTE.2,12 Importantly, there are few risks associated with mechanical compression compared with pharmacological prophylaxis with unfractionated or low molecular weight heparin, which are associated with haemorrhage, greater estimated blood loss and a higher risk of requiring a transfusion.6 The role of pharmacological VTE prophylaxis in major, complex surgeries is well established. However, in minor gynaecological procedures the benefit of pharmacological prophylaxis in comparison to mechanical prophylaxis alone is less clear.2,13,14,15 Indeed, a 2016 study found no additional benefit of pharmacological prophylaxis when added to mechanical prophylaxis in women undergoing minimally invasive surgeries for endometrial cancer.14 This finding was echoed in a large retrospective cohort study of 20 496 women undergoing hysterectomy where the addition of pre‐ or post‐operative heparin did not alter the incidence of VTE.13 Similarly, a systematic review in 2011 concluded that while mechanical prophylaxis reduced the risk of VTE from 2% to < 1% in women undergoing gynaecological surgery, there was no additional benefit of unfractionated or low molecular weight heparin in reducing the risk of VTE.2 This protocol additionally avoids the bleeding risk associated with pharmacological prophylaxis. Thus, the use of mechanical prophylaxis until the patient is ambulant appears to be adequate to manage the risk of VTE in minimally invasive gynaecological procedures. Box 2 illustrates our suggested decision tree for determining which type of prophylaxis may be appropriate.
Patient factors must be considered when determining VTE risk
It is important to note that these recommendations apply only to individuals undergoing minimally invasive surgeries that are inherently low risk themselves. Patient characteristics play an important role in VTE risk and should be considered in every surgical procedure, regardless of its complexity.1,5 In particular, the prothrombotic risk associated with cancer markedly increases the VTE risk in such patients and should be evaluated with care.5 Other important risk factors to consider are body mass index (especially > 35), age (> 60 years), inherited thrombophilia, history of prior VTE, immobility, pregnancy, hormone exposure and other medical comorbidities.5,9,13 Indeed, many of the studies investigating the importance of the mode of surgery on VTE prophylaxis found stronger covariates with VTE from these factors than in the variable of interest, suggesting that we should not forget to consider individual patient factors when deciding on appropriate VTE prophylaxis. It is vital that clinicians consider the mode of surgery as part of the broader VTE risk in the individual, and not as the sole risk‐determining factor.16
Conclusions
The risk of VTE in individuals undergoing minimally invasive, minor gynaecological procedures is very low. However, the consequences of a thromboembolic event can be catastrophic. A thorough and systematic approach to VTE prophylaxis is therefore necessary. Australian and international guidelines in this area are yet to reach consensus on an approach to minimally invasive gynaecological procedures, requiring clinicians to regularly exercise their judgement. The current literature supports the use of mechanical prophylaxis during and after surgery until the patient is ambulant, but does not find support for the addition of pharmacological prophylaxis, especially given the increased risk of bleeding. However, individual risk factors for VTE should always be considered first, with the mode of incision forming a part of that calculation, and high risk patients should be managed accordingly.
Competing interests
No relevant disclosures.
References
- Wickham N, Gallus A, Walters BN, et al. Prevention of venous thromboembolism in patients admitted to Australian hospitals: summary of National Health and Medical Research Council clinical practice guideline. Intern Med J 2012; 42: 698–708.
- Rahn DD, Mamik MM, Sanses TV, et al. Venous thromboembolism prophylaxis in gynecologic surgery: a systematic review. Obstet Gynecol 2011; 118: 1111–1125.
- Gould MK, Garcia DA, Wren SM, et al. Prevention of VTE in nonorthopedic surgical patients: antithrombotic therapy and prevention of thrombosis: American College of Chest Physicians evidence‐based clinical practice guidelines. Chest 2012; 141: e227S–e277S.
- Committee on Practice Bulletins—Gynecology, American College of Obstetricians and Gynecologists. ACOG Practice Bulletin No. 84: Prevention of deep vein thrombosis and pulmonary embolism. Obstet Gynecol 2007; 110 (2 Pt 1): 429–440.
- Jorgensen EM, Li A, Modest AM, et al. Incidence of venous thromboembolism after different modes of gynecologic surgery. Obstet Gynecol 2018; 132: 1275–1284.
- Clarke‐Pearson DL, Synan IS, Dodge R, et al. A randomized trial of low‐dose heparin and intermittent pneumatic calf compression for the prevention of deep venous thrombosis after gynecologic oncology surgery. Am J Obstet Gynecol 1993; 168: 1146–1154.
- Australian Commission on Safety and Quality in Health Care. Venous thromboembolism prevention: clinical care standard. Sydney: ACSQHC, 2020. https://www.safetyandquality.gov.au/publications-and-resources/resource-library/venous-thromboembolism-prevention-clinical-care-standard (viewed Jan 2020).
- Ageno W, Manfredi E, Dentali F, et al. The incidence of venous thromboembolism following gynecologic laparoscopy: a multicenter, prospective cohort study. J Thromb Haemost 2007; 5: 503–506.
- Barber EL, Neubauer NL, Gossett DR. Risk of venous thromboembolism in abdominal versus minimally invasive hysterectomy for benign conditions. Am J Obstet Gynecol 2015; 212(609): e1–7.
- Barber EL, Gehrig PA, Clarke‐Pearson DL. Venous thromboembolism in minimally invasive compared with open hysterectomy for endometrial cancer. Obstet Gynecol 2016; 128: 121–126.
- Kahr HS, Thorlacius‐Ussing O, Christiansen OB, et al. Venous thromboembolic complications to hysterectomy for benign disease: a nationwide cohort study. J Minim Invasive Gynecol 2018; 25(715–723): e2.
- Eppsteiner RW, Shin JJ, Johnson J, van Dam RM. Mechanical compression versus subcutaneous heparin therapy in postoperative and posttrauma patients: a systematic review and meta‐analysis. World J Surg 2010; 34: 10–19.
- Swenson CW, Berger MB, Kamdar NS, et al. Risk factors for venous thromboembolism after hysterectomy. Obstet Gynecol 2015; 125: 1139.
- Freeman AH, Barrie A, Lyon L, et al. Venous thromboembolism following minimally invasive surgery among women with endometrial cancer. Gynecol Oncol 2016; 142: 267–272.
- Sang C‐Q, Zhao N, Zhang J, et al. Different combination strategies for prophylaxis of venous thromboembolism in patients: A prospective multicenter randomized controlled study. Sci Rep 2018; 8: 8277.
- Jorgenson EM, Chur H. Venous thromboembolism in minimally invasive gynecologic surgery: a systematic review. J Minim Invasive Gynecol 2019; 26: 186–196.
Provenance: Not commissioned; externally peer reviewed.