





OECD data indicate that Australia is a comparatively high user of residential aged care
The Royal Commission into Aged Care Quality and Safety interim report highlighted many concerns about aged care in Australia.1 These include that “the system designed to care for older Australians is woefully inadequate”, and that “aged care services … have simply not been seen as a priority by successive Australian Governments”. To inform the Royal Commission, we undertook a review of international approaches to the provision of aged care.2 As a component of our review, we examined data reported to the Organisation for Economic Co‐operation and Development from 13 countries.3 The list of countries included in the review was developed in consultation with experts and with input from representatives from the Royal Commission. Countries were selected based on the availability of information, applicability to the Australian aged care system, and to ensure a diverse range of countries were represented.
Long term care is the provision of services for medical needs, personal care and assistance in living independently for people with long term dependencies due to their health care needs. Long term care can be provided in institutions (eg, nursing homes or residential aged care facilities) or by providing services to assist people to remain living in their own homes, including community services such as respite care. The OECD defines long term care institutions as specifically designed nursing and residential care facilities that provide accommodation and care as a package, with the predominant service being care. Institutional long term care recipients are those receiving formal long term care in institutions other than hospitals. We compared numbers of older long term care recipients in institutional care (12 countries) and estimates of long term care expenditure for older people (12 countries) (Box).
Australia provides institutional long term care for almost 20% of the population aged ≥ 80 years, and 6% of those aged ≥ 65 years. This places Australia as the nation with the highest proportion of older people living in institutional care compared with 11 other nations (Box). The relative use of institutional care, as opposed to home or community care, was also highest for Australia, with 52.5% of long term care recipients aged ≥ 65 years and 58.6% of long term care recipients aged ≥ 80 years in institutional care. This is in comparison to a range of 21.6% in Japan to 34.6% in the Netherlands for recipients aged ≥ 65 years, and 23.1% in Japan to 41.8% in Canada for those aged ≥ 80 years (Poland is an exception, with institutional care provided for 94.1% of long term care recipients aged ≥ 65 years, and 100% aged ≥ 80 years, based on 2006 data; however, long term care is highly limited, with only 1.6% of the population aged ≥ 80 years receiving care).
Our estimates of gross domestic product (GDP) expenditure on long term care for older people comprise the health component of government/compulsory long term care expenditure (not age‐specific) plus social expenditure on old age benefits in kind, as reported to the OECD. This approach best captures Australia's long term care expenditure on older people. Benefits in kind are services such as the home care packages program. However, this estimate does not capture cash benefits such as the carer allowance in Australia or direct cash payments that are a component of aged care benefits in some other nations (eg, Germany, England, Poland). In the OECD database, these payments cannot be separated from non‐care related cash provisions for older people, such as the age pension. The expenditure estimates indicate that many other nations spend a much greater proportion of their GDP on long term care for older people (Box). Different approaches to funding are used in other countries, including the provision of universal social care insurance, some of which includes compulsory contribution schemes such as in Japan and Germany.5
Limitations in these international comparisons include possible differences between nations in reporting or definitions of institutions, lack of data on the dependency levels of care recipients, and comparisons being limited to OECD nations reporting institutional care use. Nevertheless, the data indicate that in Australia a comparatively high proportion of older people live in institutions, with a relatively low financial investment in the whole aged care sector.
While many countries have wait lists for home care services, the wait times of over 12 months for home care packages at the approved level (for level 2 and above; ie, beyond basic care needs, providing low to high level care) may lead to premature admission to institutional care for some people.6,7,8 In November 2019, the Australian government announced funding of an additional 10 000 home care packages at a cost of $496 million.9 However, in September 2019, there were about 63 000 people waiting for an approved home care package, and an additional 49 000 people were offered, while waiting, a package at a level lower than that approved.6 Some countries focus on keeping older people at home, with greater emphasis on preventive and rehabilitation approaches.10,11 In Denmark, for example, legislation obliges local municipalities to assess all older people applying for home care for their suitability for reablement: short term home‐based training programs aiming to increase people's independence.11
To reduce the number and proportion of older Australians living in residential aged care, there needs to be an increase in investment across the sector, particularly in home‐ and community‐based care.
Box – Estimates derived from OECD data2 on proportion of older population receiving long term care (LTC) in institutions (A), and LTC estimates for expenditure on older people as a proportion of gross domestic product (GDP) (B)
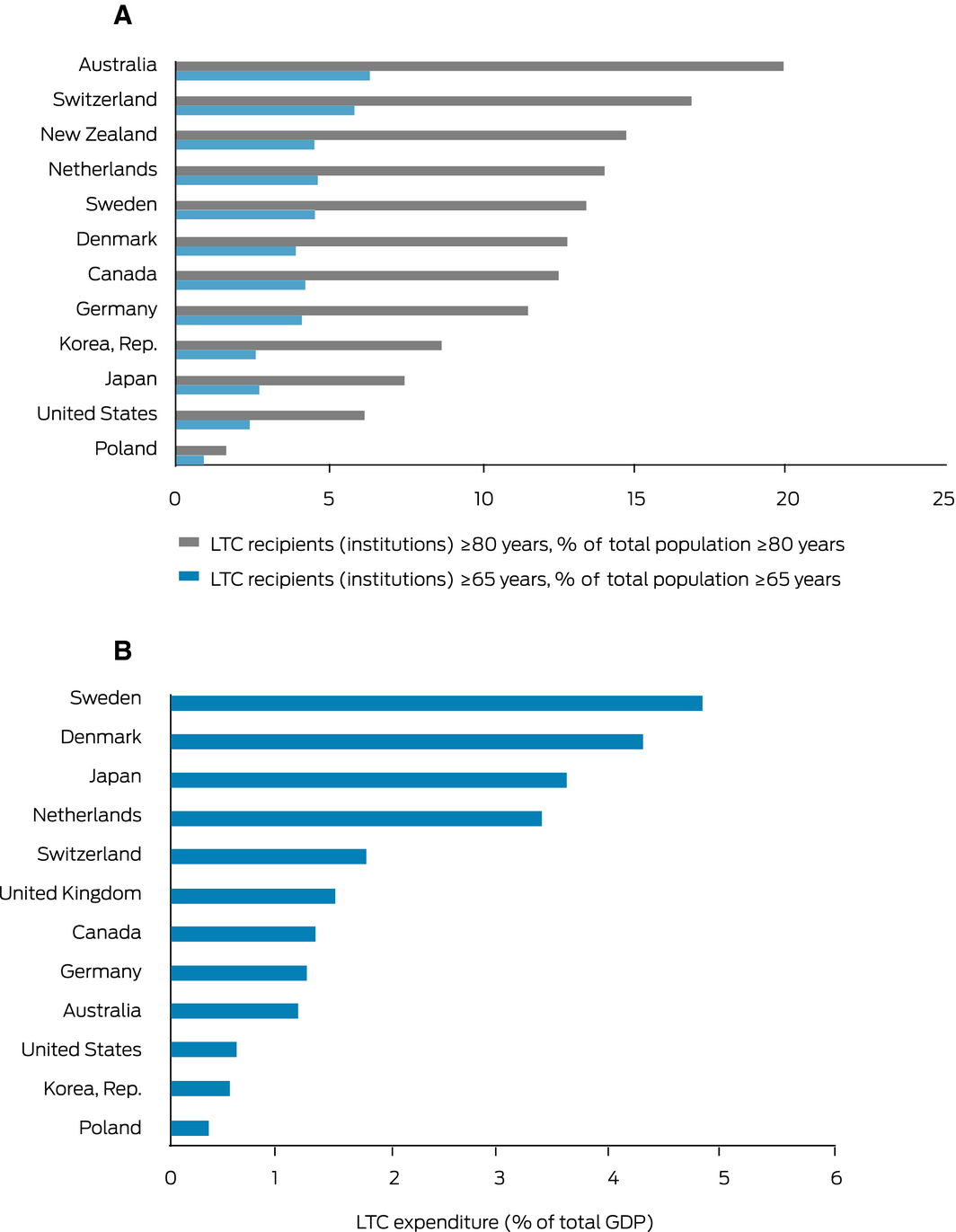
Notes: Data refer to 2015 or nearest year. A: Data not available for UK; it is unclear whether or not older people living in skilled nursing facilities are counted in US data. B: Data not available for New Zealand. Old age benefits in kind were not reported for Canada or Poland; Germany reports zero expenditure as benefits in kind. US expenditure may only include institutional care.4 Data extracted on 6 May 2019 (A) and 15 September 2019 (B) from https://stats.oecd.org/index.aspx?DataSetCode=HEALTH_STAT.3
Provenance: Not commissioned; externally peer reviewed.
- 1. Tracey R, Briggs L. Royal Commission into Aged Care Quality and Safety. Interim report: neglect. Vol. 1. Canberra: Commonwealth of Australia, 2019. https://agedcare.royalcommission.gov.au/publications/Documents/interim-report/interim-report-volume-1.pdf (viewed June 2020).
- 2. Dyer SM, Valeri M, Arora N, et al. Review of international systems for long‐term care of older people. (Research Paper 2, January 2020). Adelaide: Flinders University, 2020. https://agedcare.royalcommission.gov.au/publications/Documents/research-paper-2-review-international-systems-long-term-care.pdf (viewed June 2020)
- 3. Organisation for Economic Co‐operation and Development. OECD.Stat. https://stats.oecd.org/ (viewed Sept 2019).
- 4. Organisation for Economic Co‐operation and Development. Health at a Glance 2017: OECD Indicators. Paris: OECD Publishing, 2017. https://www.oecd.org/social/health-at-a-glance-19991312.htm (viewed Feb 2020).
- 5. Joshua LC. Aging and long term care systems: a review of finance and governance arrangements in Europe, North America and Asia‐Pacific. Washington: World Bank Group, 2017. http://documents.worldbank.org/curated/en/761221511952743424/Aging-and-long-term-care-systems-a-review-of-finance-and-governance-arrangements-in-Europe-North-America-and-Asia-Pacific (viewed Dec 2019).
- 6. Australian Government Department of Health. Home care packages program: data report 1st quarter 2019‐20. Canberra: Australian Government, 2019. https://gen-agedcaredata.gov.au/www_aihwgen/media/Home_care_report/Home-Care-Data-Report-1st-qtr-2019-20.PDF (viewed Feb 2020).
- 7. Yates I, Kaplan M, Irlam C, et al. Position paper: Keep fixing Australia's aged care system … taking the next steps in tandem with the Royal Commission. Canberra: COTA, 2018. https://www.cota.org.au/publication/keep-fixing-australias-aged-care-system/ (viewed Feb 2020).
- 8. Daly M. Rethinking the approach to long‐term care. Wirtschaftspolitische Blatter 2018; 65: 77–83.
- 9. Australian Journal of Dementia Care. Govt's $537m response to Royal Commission interim report. 9 Dec 2019. https://journalofdementiacare.com/royal-commission-interim-report/ (viewed Feb 2020).
- 10. Kelders Y, de Vaan K. ESPN thematic report on challenges in long‐term care: Netherlands. Brussels: European Commission, 2018. https://ec.europa.eu/social/BlobServlet?docId=19861&langId=en (viewed Feb 2020).
- 11. Bodker MN, Langstrup H, Christensen U. What constitutes ‘good care’ and ‘good carers’? The normative implications of introducing reablement in Danish home care. Health Soc Care Community 2019; 27: e871–e878.
This work was funded by the Royal Commission into Aged Care Quality and Safety and the National Health and Medical Research Council (NHMRC) Cognitive Decline Partnership Centre. Staff and an advisor of the Royal Commission into Aged Care Quality and Safety contributed to the selection of countries to be reviewed, and collection and interpretation of data on international GDP expenditure on long term care. The Aged Care Royal Commission did not contribute to the drafting of, or interpretation of the data in, this article. The contents of the published materials are solely the responsibility of the administering institution, Flinders University, and the individual authors identified, and do not reflect the views of the NHMRC or the funders.
Maria Crotty was part of the NHMRC Cognitive Decline Partnership Centre and received funds. This partnership centre included three Australian not‐for‐profit aged care providers. Suzanne Dyer received salary from these grants. Dominic Tilden is owner and director of, and Madeline Valeri and Nimita Arora are employees of, a private health economics consultancy that provides services to multiple pharmaceutical and devices companies, but no aged care providers.