





Volume 208 - Issue 6
Sports injuries in Victoria, 2012–13 to 2014–15: evidence from emergency department records
Authors: D Tharanga Fernando, Janneke Berecki-Gisolf and Caroline F Finch
Med J Aust 2018; 208 (6): 255-260. || doi: 10.5694/mja17.00872
Published online: 2 April 2018
Published online: 2 April 2018
Evaluating sports injury rates per participant and the relative severity of injuries is important for monitoring safety
Abstract
Objectives: To report the incidence of presentations to emergency departments (EDs) in Victoria for sport- and active recreation-related injuries; to establish which sports have the highest rates of injury per participant; to assess the effects of age and sport type on the rate of serious sport injury (resulting in admission to hospital).
Design, setting and participants: Retrospective analysis of 171 541 ED presentations to 38 Victorian hospitals, 2012–13 to 2014–15. Sports- and active recreation-related injuries in people aged 5 years or more were identified from coded data and by text searches.
Main outcome measures: Population rates of injuries by sport and ranking of sports by per participant injury rates (for people aged 15 years or more); proportions of presenting patients subsequently admitted to hospital (serious sport injuries) (for people aged 5 years or more).
Results: During 2012–13 to 2014–15, there were 171 541 presentations to EDs with sports-related injuries. Sports most commonly associated with presentation by people aged 15 years or more were Australian football, motor sports, and cycling/BMX; the highest per participant injury rates (people aged 15 or more) were for motor sports, rugby, and skateboarding/inline hockey/roller sports. 11% of ED patients aged 5 years or more were subsequently admitted to hospital; the odds of admission were highest for those with injuries from motor sports, horse riding, or cycling/BMX.
Conclusions: Assessing sports injury rates corrected for participation rates and evaluating the relative severity of injuries is important for monitoring safety. Our findings can assist decisions about which sports should be the focus of injury prevention efforts.
The known The number of patients treated in hospital for sport-related injuries has increased in recent years, placing an increasing burden on the health service system.
The new In Victoria, the sports associated with the highest numbers of presentations of people aged 15 years or more to emergency departments are Australian football, motor sports, and cycling/BMX, but participant injury rates are highest for motor sports, rugby, and skateboarding and similar activities, while hospital admission rates are highest for horse riding, motor sports, and cycling/BMX.
The implications Sports injury prevention initiatives should focus on sports associated with high per participant injury rates or with relatively severe injuries.
Health campaigns promote participation in sport or active recreation to enhance physical wellbeing. Participation rates for jogging, running, fitness and gym activities, and cycling and bicycle motocross (BMX) have risen in recent years,1 suggesting that physical activity campaigns have been effective. The frequency of sport-related injury, however, has also risen. Identifying which sports have the highest rates of injury and serious injury, and which population subgroups are at greater risk, is necessary for informing public health campaigns that promote safe physical activity. Injury rates should be expressed not only as population rates, but also as per participant injury rates; the relative safety of a sport can be better assessed by taking the participation rate into account.
Various types of football, motor, and water sports accounted for nearly half the hospitalisations in Australia for sports injuries during 2011–12; participant injury rates were particularly high for motor sports, roller sports, Australian football, and rugby.2 Life-threatening injuries were most frequently associated with cycling, motor sports, and horse riding. In Victoria, the number of hospital-treated (non-fatal) sport injuries in all age groups increased significantly during the 7-year period, 2004–2010.3,4
Systematic population-level monitoring of sports injuries is not currently undertaken in Australia. Australia-wide sports injury hospitalisation data have been reported,2 but fewer than 10% of sports injuries lead to hospital admission,5,6 although many are treated in emergency departments (EDs). A dataset of injury presentations to Victorian EDs provides a unique opportunity for exploring trends in sports injury at the population level.
The aims of our study were to report the incidence of presentations to EDs in Victoria for sport- and active recreation-related injuries, and to establish which sports have the highest rates of injury per participant. We also examined the effects of age and sport type on the rate of serious sport injury, defined by the patient being admitted to hospital after presenting to an ED.
Methods
Data sources
We undertook a retrospective case series analysis based on ED presentations data extracted from the Victorian Emergency Minimum Dataset (VEMD), which records information (including level 1 injury surveillance data) from 38 Victorian public hospitals providing a 24-hour ED service. These hospitals account for about 80% of ED presentations in Victoria.7 Data collection was in accordance with National Minimum Data Standards for injury surveillance.8 Cost data were extracted from the Victorian Cost Data Collection (VCDC), which contains data on the average costs (direct and indirect) of treating patients in EDs according to age group, sex and diagnosis code.9
Two types of denominator data were employed. Residential population data for the age groups ≥ 5 and ≥ 15 years in Victoria for the period 2012–13 to 2014–1510 were available for calculating population injury rates. Participant injury rates during 2013–14 were calculated from sports participation data for the ≥ 15 years age group included in a customised report prepared for this study by the Australian Bureau of Statistics in 2017, based on data collected by the 2013–14 Participation in Sport and Physical Recreation survey11 (online Appendix, box 1). Sports participation data were not available for children under 15 years of age or for other years.
Injury case selection
ED presentations between 1 July 2012 and 30 June 2015 by people aged 5 years or more were included. As data for sports participation were available only for people aged 15 years or more, cases selected for participation-adjusted injury rate calculations were limited to this age group; to allow comparisons, these cases were also selected for calculating matching population injury rates.
An algorithm was developed for selecting cases in which injury resulted from being engaged in sport or active recreation, including “activity when injured” and “place where injury occurred” variables, and the “description of injury event” (patient’s personal account or description of injury event, provided at triage)12 (online Appendix, box 2). No distinction was made between organised and non-organised sport, as this information was not consistently available in the VEMD. Data selection was limited to incident cases (excluding return ED visits and pre-arranged admissions). Those requiring subsequent hospital admission (ie, patients admitted directly from an ED to a hospital ward or unit) were identified. Patients coded as deceased on discharge were excluded from analysis of subsequent hospital admissions.
Statistical analysis
Analyses were conducted in Stata 14.0 (StataCorp). χ2 tests and binary logistic regressions (univariate and multivariate models) were employed; the binary model outcome was subsequent admission v no subsequent admission to hospital. The main explanatory variable of interest was sport type. Because participation and the type of sport played varied considerably by sex, the analyses were stratified by this factor and different sports served as reference groups (Australian football for males, netball for females). All reported results are for the sample aged 5 years or more, except Box 1, which is based on a subsample of those aged 15 years or more.
Ethics approval
Analysis of Victorian Injury Surveillance Unit emergency department data and hospital admissions data was reviewed by the Monash University Human Research Ethics committee and was granted exemption from ethics review; the research satisfies section 5.1.22 of the National Statement on Ethical Conduct in Human Research.13
Results
Emergency department presentations
There were 1 036 978 presentations for injuries by people aged 5 years or more to the VEMD-reporting hospitals in Victoria during 2012–13 to 2014–15, of which 171 541 (17%; 57 180 per year) were related to sport or active recreation. The number of sports injury-related ED presentations increased from 54 789 in 2012–13 to 60 734 in 2014–15 (11% increase), or from 1031 to 1102 per 100 000 population (7% increase). Of these patients, 18 666 (11%) were subsequently admitted to hospital.
The twenty sports associated with the highest numbers of ED presentations by people aged 15 years or more accounted for 85 718 presentations, or almost 74% of all sports injury ED presentations in this age group. The sports associated with the highest numbers of presentations were Australian football, motor sports, and cycling/BMX, but the participant injury rates were highest for motor sports, rugby, and skateboarding and other roller sports (Box 1).
Almost two-thirds of ED presentations with injuries associated with the top twenty causes of sport-related injury were by people aged 5–24 years; 30 819 presentations (24%) were by people aged 25–44 and 9820 (8%) by people aged 45 or more. Males accounted for 91 333 injury presentations (72%) associated with these sports, but the proportion differed by sport (Box 2).
An estimated $17.9 million was spent annually on ED presentations for sports-related injuries incurred in the twenty sports with which the greatest numbers of presentations were associated. The sports associated with the highest total ED costs were Australian football, motor sports, and cycling/BMX; the sports with the highest costs per presentation were motor sports, horse riding, and cycling/BMX (Box 3).
Hospital admissions after presentation to an emergency department
The proportion of patients aged 5 years or more admitted to hospital after presenting to an ED was greatest for injuries incurred during horse riding, motor sports, and cycling/BMX. The highest absolute number of hospital admissions were for motor sports (3239), cycling/BMX (2501) and Australian football (2483) (Box 4).
We restricted further analysis of admission to hospital after an ED presentation to the ten sports that most frequently resulted in injury ED presentations for each sex; these cases accounted for 82 728 presentations by males (68% of all sport-related presentations) and 30 730 by females (62%). The final reduced model included age, region and sport as factors, and an age–sport interaction (Box 5).
After adjusting for age and region, the odds of males presenting to an ED being admitted to hospital were greatest for injuries related to motor sports (v Australian football: adjusted odds ratio [aOR], 3.99; 95% CI, 3.63–4.38), horse riding or other equestrian activities (aOR, 3.31; 95% CI, 2.34–4.68), and cycling/BMX (aOR, 2.20; 95% CI, 1.94–2.50; for each, P < 0.001). The odds for basketball, soccer, and cricket were lower than for Australian football (all P < 0.001) (Box 5, online Appendix, figure 1).
After adjusting for age and region, the odds of females presenting to an ED being admitted to hospital were greatest for injuries related to horse riding (v netball: aOR, 18.3; 95% CI, 13.5–24.8), motor sports (aOR, 12.5; 95% CI, 8.74–18.0), and cycling/BMX (aOR, 8.65; 95% CI, 5.71–13.1; for each, P < 0.001) (Box 5, online Appendix, figure 2).
Higher age was associated with a significantly increased likelihood of hospital admission for both sexes (Box 5).
Discussion
The sports associated with the highest numbers of injury-related presentations to EDs by people aged 5 years or more were Australian football, motor sports, cycling/BMX, basketball, soccer, and netball. An earlier study14 found that football, basketball, netball, hockey, and cricket were associated with the highest numbers of presentations to EDs; we found that injuries from motor sports and horse riding were more frequent than for cricket or hockey.
The highest injury rates per participant among those aged 15 years or more were for motor sports, rugby, skateboarding, weightlifting, Australian football, and horse riding. Swimming, cycling, and cricket had high participation rates, but injury rates were relatively low. A 2003 study of sports participation and injuries in the Latrobe Valley, Victoria, found that Australian football, cycling, and basketball were associated with the highest per participant injury rates in people aged 5 years or more.6 The difference between these findings and ours result from the large standard errors for participation estimates for motor sports, rugby, and weightlifting in our study, and the inclusion of children under 15 in the Latrobe study. Motor sports have been reported to have the highest per participant injury rates in Australia,2 consistent with our findings.
The sports and recreation activities with the highest odds of hospital admission following presentation to an ED were horse riding, motor sports, and cycling/BMX. Few sports injuries studies have focused on the activities most frequently associated with severe injury; an American study found that all-terrain vehicle riding, motocross, and horse riding had high relative risks of hospital admission, while the relative risks for basketball and soccer were low,15 consistent with our findings.
Higher age was significantly associated with subsequent hospital admission; only 8% of ED presentations in our study were by people aged 45 or more, but they were significantly more likely than younger patients to be admitted to hospital. This is consistent with earlier research which found that the odds of hospital admission increased with age.15
Total ED treatment costs were highest for Australian football-related injuries, but the cost per incident was relatively moderate; both total costs and cost per incident were high for motor sport-related injuries, while total costs for horse riding injuries were lower, but the cost per incident was high.
Strengths and limitations
One strength of our study was that coverage of sport injury-related presentations to EDs was near complete, although the VEMD does not include cases treated at EDs in private hospitals. Our study is one of few to analyse sports injuries in Victoria stratified by sex, adding another layer of information to previous work.6,16 Other strengths include our methods for identifying cases, and our inclusion of exposure data.
The quality of case selection relied on accurate coding and good narrative recording by ED staff. The quality of VEMD data varies between hospitals; some do not provide accurate coding and informative text narratives, or text narratives that match coded fields. Coded fields (eg, “activity when injured”) were used for identifying cases, but in the VEMD not all sports injury cases are coded as sport-related. We diminished this problem by screening text narrative to identify sports injury cases not coded as such. The narratives also have quality problems, relying on the accuracy and completeness of reporting, but this is likely to be consistent across all sports injury presentations and unlikely to affect relative injury rates.
Injury rates based on sports participation rates rather than on general population numbers is preferable, but participation data for children aged 5–15 years was not available in the survey data supplied. The reliability of participation data was also limited by survey constraints, with relative standard errors exceeding 25% for some sports; the estimates for motor sports and rugby are considered unreliable. Further, the survey participation estimates were sometimes lower than cited by other sources. For example, participation in Australian football in 2013–14 was estimated to be 121 000, but the most recent Australian Football League survey (2017) reported 462 000 participants;17 the 2015–16 cricket census reported 328 000 Victorians playing cricket,18 compared with 92 000 in the sports participation survey. These differences can largely be attributed to differing data collection methods, and verifying per participant injury rates will require further research.
It was not always possible to distinguish between sport and similar non-leisure activities (eg, cycling as a mode of transport). The incidence of Australian football-related injuries may have been overestimated, as all unspecified football injuries were coded to Australian football because of its popularity in Victoria. Finally, a large proportion of people with sports injuries present to physiotherapists and general practitioners rather than EDs,16 and injuries not requiring professional medical attention receive on site treatment only. Our study consequently did not reflect the overall incidence of sports injuries in Victoria.
Conclusions
Taking participation into account gives valuable insights into the relative safety of different sports. For example, many injuries are incurred during Australian football, but the injury rate is lower than for motor sports when adjusted for participation. Participation-adjusted sports injury rates and evaluating the risk of subsequent hospital admission, corrected for demographic factors, is useful for sports officials and organisations, health promotion agencies, and others actively monitoring safety in sport. Our findings can help set targets for reducing injury rates and deciding which sports should be the focus of injury prevention efforts.
Age, sex, and type of activity influence the incidence and severity of sports-related injuries treated at EDs and the proportion of patients subsequently admitted to hospital. Efforts to reduce the likelihood of serious injury should concentrate on lower participation sports with higher rates of hospitalisation, such as motor sports and horse riding, and on sports with high per participant injury rates, such as motor sports, rugby, and skateboarding. We recommend further investigation of the settings in which motor sports, horse riding, and other activities are undertaken for reliably evaluating current safety measures.
Box 1 – The twenty sport and recreational activity types associated with the highest numbers of injury-related presentations to emergency departments (EDs) by people aged 15 years or more (initial presentations only), Victoria, 2012–13 to 2014–15*
|
Sports activity |
2012–13 to 2014–15 |
2013–14 |
|||||||||||||
|
ED presentations (proportion of overall total) |
Annual injury rate, per 100 000 population |
ED presentations (proportion of overall total) |
Participants† |
Injury rate, per 100 000 participants |
Injury rate, rank |
||||||||||
|
|
|||||||||||||||
|
Australian football |
20 784 (17.9%) |
146.6 |
6747 (17.8%) |
121 000 |
5576 |
5 |
|||||||||
|
Motor sports |
9655 (8.3%) |
68.1 |
3168 (8.4%) |
10 200¶ |
31 059 |
1 |
|||||||||
|
Cycling/BMX |
8432 (7.3%) |
59.5 |
2752 (7.3%) |
300 500 |
916 |
18 |
|||||||||
|
Basketball (indoor/outdoor) |
7991 (6.9%) |
56.4 |
2767 (7.3%) |
176 900 |
1564 |
9 |
|||||||||
|
Soccer (indoor/outdoor) |
7227 (6.2%) |
51.0 |
2317 (6.1%) |
123 100 |
1882 |
8 |
|||||||||
|
Netball (indoor/outdoor) |
5483 (4.7%) |
38.7 |
1777 (4.7%) |
142 300 |
1249 |
13 |
|||||||||
|
Horse riding/equestrian activities/polo |
4825 (4.2%) |
34.0 |
1520 (4.0%) |
29 000§ |
5241 |
6 |
|||||||||
|
Skateboarding/inline hockey (indoor/outdoor)‡/roller sports |
4593 (4.0%) |
32.4 |
1450 (3.8%) |
19 000§ |
7633 |
3 |
|||||||||
|
Cricket (indoor/outdoor) |
3527 (3.0%) |
24.9 |
1145 (3.0%) |
92 600§ |
1237 |
14 |
|||||||||
|
Ice/snow sports |
1888 (1.6%) |
13.3 |
526 (1.4%) |
35 300§ |
1490 |
10 |
|||||||||
|
Dancing/ballet |
1665 (1.4%) |
11.7 |
545 (1.4%) |
49 800 |
1094 |
15 |
|||||||||
|
Hockey (indoor/outdoor) |
1476 (1.3%) |
10.4 |
472 (1.2%) |
11 700¶ |
4034 |
7 |
|||||||||
|
Rugby |
1405 (1.2%) |
9.9 |
456 (1.2%) |
4100¶ |
11 122 |
2 |
|||||||||
|
Weightlifting/powerlifting/body building |
1074 (0.9%) |
7.6 |
362 (1.0%) |
5100¶ |
7098 |
4 |
|||||||||
|
Martial arts |
1057 (0.9%) |
7.5 |
339 (0.9%) |
46 400§ |
731 |
19 |
|||||||||
|
Athletics (track and field) |
984 (0.8%) |
6.9 |
334 (0.9%) |
35 100§ |
952 |
17 |
|||||||||
|
Fishing |
967 (0.8%) |
6.8 |
337 (0.9%) |
31 300§ |
1077 |
16 |
|||||||||
|
Surf sports |
925 (0.8%) |
6.5 |
316 (0.8%) |
25 200§ |
1254 |
12 |
|||||||||
|
Water skiing/powerboating |
891 (0.8%) |
6.3 |
300 (0.8%) |
21 900§ |
1370 |
11 |
|||||||||
|
Swimming/diving |
869 (0.8%) |
6.1 |
313 (0.8%) |
281 300 |
111 |
20 |
|||||||||
|
Total for top 20 sport/recreation types |
85 718 (74.0%) |
604.8 |
27 943 (73.7%) |
— |
— |
— |
|||||||||
|
Other sport/recreation types |
30 109 (26.0%) |
212.4 |
9976 (26.3%) |
— |
— |
— |
|||||||||
|
Total |
115 827 |
817.2 |
37 919 |
— |
— |
— |
|||||||||
|
|
|||||||||||||||
|
* Sources: Victorian Emergency Minimum Dataset (injuries), Australian Bureau of Statistics (population data),10 customised extraction from catalogue data for Victoria by the Bureau (sports participation data [2013–14]). † Players, competitors, or persons aged 15 years or more who participated in a physically active role during the 12 months prior to survey (excluded those who participated solely as coaches, umpires or club officials). ‡ Hockey played on roller skates. § Standard error for estimate of participation, 25–50%; to be used with caution. ¶ Standard error for estimate of participation, > 50%; estimate classed as unreliable. |
|||||||||||||||
Box 2 – The twenty sport and recreational activity types associated with the highest numbers of injury-related presentations to emergency departments by people aged 5 years or more (initial visits only), Victoria, 2012–13 to 2014–15, by age and sex*
|
Sports activity |
Sex |
Age group |
Total |
||||||||||||
|
Male |
Female |
5–14 years |
15–24 years |
25–44 years |
≥ 45 years |
||||||||||
|
|
|||||||||||||||
|
Australian football |
27 679 (94%) |
1861 (6%) |
8756 (30%) |
14 407 (49%) |
5888 (20%) |
489 (2%) |
29 540 |
||||||||
|
Basketball (indoor/outdoor) |
9086 (66%) |
4591 (34%) |
5686 (42%) |
5161 (38%) |
2538 (19%) |
292 (2%) |
13 677 |
||||||||
|
Cycling/BMX |
9942 (77%) |
2978 (23%) |
4488 (35%) |
2516 (19%) |
3541 (27%) |
2375 (18%) |
12 920 |
||||||||
|
Motor sports |
10 503 (88%) |
1465 (12%) |
2313 (19%) |
4231 (35%) |
3796 (32%) |
1628 (14%) |
11 968 |
||||||||
|
Soccer (indoor/outdoor) |
9316 (83%) |
1865 (17%) |
3954 (35%) |
4267 (38%) |
2620 (23%) |
340 (3%) |
11 181 |
||||||||
|
Skateboarding/inline hockey (indoor/outdoor)/roller sports |
7558 (69%) |
3324 (31%) |
6289 (58%) |
2788 (26%) |
1500 (14%) |
305 (3%) |
10 882 |
||||||||
|
Netball (indoor/outdoor) |
600 (8%) |
7133 (92%) |
2250 (29%) |
3151 (41%) |
2139 (28%) |
193 (2%) |
7733 |
||||||||
|
Horse riding/equestrian activities/polo |
1221 (20%) |
4826 (80%) |
1222 (20%) |
1511 (25%) |
1776 (29%) |
1538 (25%) |
6047 |
||||||||
|
Cricket (indoor/outdoor) |
4245 (94%) |
290 (6%) |
1008 (22%) |
1247 (27%) |
1802 (40%) |
478 (11%) |
4535 |
||||||||
|
Ice/snow sports |
1415 (59%) |
976 (41%) |
503 (21%) |
809 (34%) |
817 (34%) |
262 (11%) |
2391 |
||||||||
|
Dancing/ballet |
505 (23%) |
1711 (77%) |
551 (25%) |
811 (37%) |
514 (23%) |
340 (15%) |
2216 |
||||||||
|
Rugby |
1765 (91%) |
173 (9%) |
533 (28%) |
887 (46%) |
478 (25%) |
40 (2%) |
1938 |
||||||||
|
Hockey (indoor/outdoor) |
1138 (59%) |
786 (41%) |
448 (23%) |
743 (39%) |
601 (31%) |
132 (7%) |
1924 |
||||||||
|
Swimming/diving |
1030 (61%) |
645 (39%) |
806 (48%) |
355 (21%) |
321 (19%) |
193 (12%) |
1675 |
||||||||
|
Athletics (track and field) |
718 (47%) |
813 (53%) |
547 (36%) |
337 (22%) |
440 (29%) |
207 (14%) |
1531 |
||||||||
|
Water volleyball/rafting/other water sports |
884 (61%) |
577 (39%) |
641 (44%) |
308 (21%) |
310 (21%) |
202 (14%) |
1461 |
||||||||
|
Martial arts |
1079 (76%) |
350 (24%) |
372 (26%) |
399 (28%) |
555 (39%) |
103 (7%) |
1429 |
||||||||
|
Jogging/running |
827 (59%) |
575 (41%) |
681 (49%) |
277 (20%) |
321 (23%) |
123 (9%) |
1402 |
||||||||
|
Weightlifting/powerlifting/body building |
832 (70%) |
352 (30%) |
110 (9%) |
403 (34%) |
503 (42%) |
168 (14%) |
1184 |
||||||||
|
Fishing |
990 (86%) |
162 (14%) |
185 (16%) |
196 (17%) |
359 (31%) |
412 (36%) |
1152 |
||||||||
|
Total for top 20 sport/recreation types |
91 333 (72%) |
35 453 (28%) |
41 343 (33%) |
44 804 (35%) |
30 819 (24%) |
9820 (8%) |
126 786 |
||||||||
|
Other sport/recreation types |
30 249 (68%) |
14 506 (32%) |
14 371 (32%) |
14 941 (33%) |
11 338 (25%) |
4105 (9%) |
44 755 |
||||||||
|
Total |
121 582 (71%) |
49 959 (29%) |
55 714 (32%) |
59 745 (35%) |
42 157 (25%) |
11 338 (7%) |
171 541 |
||||||||
|
|
|||||||||||||||
|
* Source: Victorian Emergency Minimum Dataset. |
|||||||||||||||
Box 3 – Emergency department treatment costs for injury-related presentations to emergency departments by people aged 5 years or more for the twenty sport and recreational activity types associated with the highest numbers of presentations (initial and subsequent visits), Victoria, 2012–13 to 2014–15*
|
Sports activity |
Emergency department presentations |
Estimated emergency department costs per year |
Emergency department costs per presentation |
||||||||||||
|
Mean annual expenditure ($) |
Ranking |
Mean cost per incident ($) |
Ranking |
||||||||||||
|
|
|||||||||||||||
|
Australian football |
29 624 |
3 869 746 |
1 |
391.9 |
9 |
||||||||||
|
Motor sports |
12 013 |
2 487 993 |
2 |
621.3 |
1 |
||||||||||
|
Cycling/BMX |
12 947 |
2 190 833 |
3 |
507.6 |
3 |
||||||||||
|
Basketball (indoor/outdoor) |
13 726 |
1 541 064 |
4 |
336.8 |
18 |
||||||||||
|
Skateboarding/inline hockey/roller sports |
10 934 |
1 383 583 |
5 |
379.6 |
12 |
||||||||||
|
Soccer (indoor/outdoor) |
11 215 |
1 356 029 |
6 |
362.7 |
15 |
||||||||||
|
Horse riding/equestrian activities/polo |
6072 |
1 243 861 |
7 |
614.6 |
2 |
||||||||||
|
Netball (indoor/outdoor) |
7777 |
839 829 |
8 |
324.0 |
19 |
||||||||||
|
Cricket (indoor/outdoor) |
4554 |
552 597 |
9 |
364.0 |
14 |
||||||||||
|
Ice/snow sports |
2400 |
360 426 |
10 |
450.5 |
4 |
||||||||||
|
Dancing/ballet |
2221 |
283 019 |
11 |
382.3 |
11 |
||||||||||
|
Rugby |
1939 |
274 755 |
12 |
425.1 |
5 |
||||||||||
|
Hockey (indoor/outdoor) |
1927 |
229 971 |
13 |
358.0 |
16 |
||||||||||
|
Swimming/diving |
1676 |
228 580 |
14 |
409.2 |
7 |
||||||||||
|
Water volleyball/rafting/other water sports |
1465 |
203 126 |
15 |
416.0 |
6 |
||||||||||
|
Athletics (track and field) |
1533 |
199 570 |
16 |
390.5 |
10 |
||||||||||
|
Martial arts |
1432 |
179 917 |
17 |
376.9 |
13 |
||||||||||
|
Jogging/running |
1407 |
160 682 |
18 |
342.6 |
17 |
||||||||||
|
Weightlifting/powerlifting/body building |
1154 |
157 224 |
19 |
408.7 |
8 |
||||||||||
|
Fishing |
1185 |
126 546 |
20 |
320.4 |
20 |
||||||||||
|
Total |
127 539 |
17 869 354 |
|
420.3 |
|
||||||||||
|
|
|||||||||||||||
|
* Source: Victorian Emergency Minimum Dataset. |
|||||||||||||||
Box 4 – Number of sports injury-related presentations to emergency departments (EDs) by people aged 5 years or more, and the proportion subsequently admitted to hospital, Victoria, 2012–13 to 2014–15, by sport*
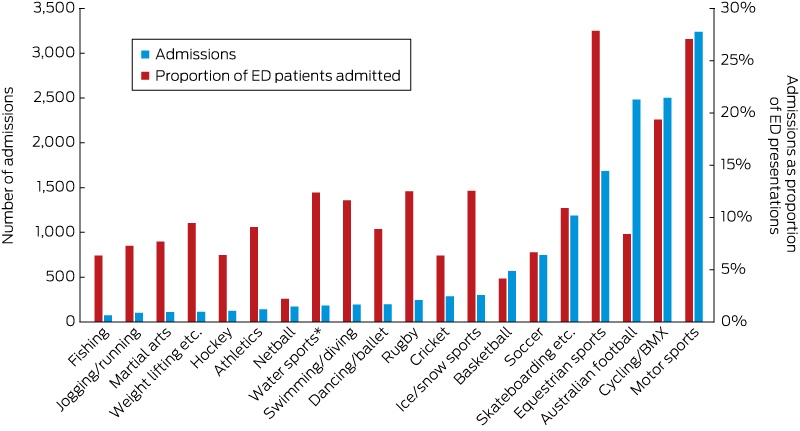
* Source: Victorian Emergency Minimum Dataset.
Box 5 – Univariate and multivariate analyses of hospital admission following sport-related injury presentations to emergency departments by people aged 5 years or more, Victoria, 2012–13 to 2014–15, for ten most common causes of injury, by sex
|
Variable |
Males |
Females |
|||||||||||||
|
Univariate model |
Final reduced multivariate model* |
Univariate model |
Final reduced multivariate model* |
||||||||||||
|
Odds ratio (95% CI) |
P |
Adjusted odds |
P |
Odds ratio (95% CI) |
P |
Adjusted odds |
P |
||||||||
|
|
|||||||||||||||
|
Age group (years) |
|
|
|
|
|
|
|
|
|||||||
|
5–14 |
0.91 (0.86–0.96) |
0.001 |
0.88 (0.79–0.97) |
0.012 |
0.88 (0.79–0.97) |
0.014 |
1.23 (0.82–1.82) |
0.32 |
|||||||
|
15–24 |
Reference |
|
Reference |
|
Reference |
|
Reference |
|
|||||||
|
25–44 |
1.39 (1.32–1.47) |
< 0.001 |
1.11 (0.99–1.24) |
0.06 |
1.78 (1.60–1.97) |
< 0.001 |
1.23 (0.81–1.85) |
0.33 |
|||||||
|
≥ 45 |
3.10 (2.90–3.33) |
< 0.001 |
1.45 (1.08–1.94) |
0.014 |
5.00 (4.47–5.60) |
< 0.001 |
4.10 (2.14–7.85) |
< 0.001 |
|||||||
|
Sport type |
|
|
|
|
|
|
|
|
|||||||
|
Australian football |
Reference |
|
Reference |
|
3.17 (2.49–4.05) |
< 0.001 |
3.50 (2.34–5.23) |
< 0.001 |
|||||||
|
Basketball |
0.53 (0.47–0.59) |
< 0.001 |
0.47 (0.40–0.55) |
< 0.001 |
1.43 (1.14–1.81) |
0.002 |
1.55 (1.02–2.35) |
0.039 |
|||||||
|
Cycling/BMX |
2.65 (2.48–2.83) |
< 0.001 |
2.20 (1.94–2.50) |
< 0.001 |
9.90 (8.22–11.92) |
< 0.001 |
8.65 (5.71–13.1) |
< 0.001 |
|||||||
|
Motor sports |
4.18 (3.94–4.44) |
< 0.001 |
3.99 (3.63–4.38) |
< 0.001 |
11.36 (9.25–13.94) |
< 0.001 |
12.5 (8.74–18.0) |
< 0.001 |
|||||||
|
Soccer (indoor/outdoor) |
0.82 (0.75–0.90) |
< 0.001 |
0.68 (0.58–0.78) |
< 0.001 |
2.07 (1.57–2.73) |
< 0.001 |
2.11 (1.33–3.34) |
0.001 |
|||||||
|
Skateboarding/inline hockey/roller sports |
1.34 (1.24–1.46) |
< 0.001 |
1.17 (1.01–1.36) |
0.034 |
5.27 (4.33–6.40) |
< 0.001 |
5.95 (3.92–9.04) |
< 0.001 |
|||||||
|
Netball (indoor/outdoor) |
NM |
|
NM |
|
Reference |
|
Reference |
|
|||||||
|
Horse riding/equestrian activities/polo |
4.66 (4.10–5.30) |
< 0.001 |
3.31 (2.34–4.68) |
< 0.001 |
17.1 (14.4–20.3) |
< 0.001 |
18.3 (13.5–24.8) |
< 0.001 |
|||||||
|
Cricket (indoor/outdoor) |
0.74 (0.65–0.84) |
< 0.001 |
0.58 (0.44–0.75) |
< 0.001 |
NM |
|
NM |
|
|||||||
|
Ice/snow sports |
1.61 (1.37–1.89) |
< 0.001 |
1.31 (0.99–1.75) |
0.06 |
6.09 (4.74–7.84) |
< 0.001 |
5.13 (3.20–8.23) |
< 0.001 |
|||||||
|
Rugby |
1.55 (1.34–1.79) |
< 0.001 |
1.38 (1.11–1.71) |
0.003 |
NM |
|
NM |
|
|||||||
|
Dancing/ballet |
NM |
|
NM |
|
4.00 (3.16–5.07) |
< 0.001 |
1.70 (0.99–2.89) |
0.05 |
|||||||
|
|
|||||||||||||||
|
NM = not modelled; these sports were not among top ten sports for presentations to emergency departments by members of this sex. * Adjusted for age group and geographic region of residence. |
|||||||||||||||
Competing interests
No relevant disclosures.
Acknowledgements
The Victorian Injury Surveillance Unit is supported by the Victorian Government.
References
- Australian Bureau of Statistics. 4177.0. Participation in sport and physical recreation, Australia, 2011–12 — Victoria (table 12). Dec 2012. http://www.abs.gov.au/AUSSTATS/abs@.nsf/DetailsPage/4177.02011-12?OpenDocument (viewed Mar 2017).
- Kreisfeld R, Harrison J, Pointer S. Australian sports injury hospitalisations 2011–12 (AIHW Cat. No. INJCAT 168; Injury Research and Statistics Series No. 92). Canberra: Australian Institute of Health and Welfare, 2014.
- Finch C, Kemp J, Clapperton A. The incidence and burden of hospital-treated sports-related injury in people aged 15+ years in Victoria, Australia, 2004–2010: a future epidemic of osteoarthritis? Osteoarthritis Cartilage 2015; 23: 1138-1143.
- Finch CF, Wong Shee A, Clapperton A. Time to add a new priority target for child injury prevention? The case for an excess burden associated with sport and exercise injury: population-based study. BMJ Open 2014; 4: e005043.
- Sallis R, Jones K, Sunshine S, et al. Comparing sports injuries in men and women. Int J Sports Med 2001; 22: 420-423.
- Cassell EP, Finch CF, Stathakis V. Epidemiology of medically treated sport and active recreation injuries in the Latrobe Valley, Victoria, Australia. Br J Sports Med 2003; 37: 405-409.
- Ashby A, Clapperton A, Ozanne-Smith J, et al. The 50th issue of HAZARD, a celebration of VISAR’s achievements. Hazard [internet] 2002; (50): 1-25. https://www.monash.edu/__data/assets/pdf_file/0009/218439/haz50.pdf (viewed Mar 2017).
- Victorian Government Department of Health and Human Services. Victorian Emergency Minimum Dataset (VEMD) archive. http://www.health.vic.gov.au/archive-hdss/archive/index-vemd.htm (viewed Mar 2017).
- Victorian Government Department of Health and Human Services. Victorian Cost Data Collection (VCDC). https://www2.health.vic.gov.au/hospitals-and-health-services/data-reporting/health-data-standards-systems/data-collections/vcdc (viewed Mar 2017).
- Australian Bureau of Statistics. Quarterly population estimates (ERP) by state/territory, sex and age. ABS.Stat [website]. http://stat.data.abs.gov.au/Index.aspx?DatasetCode=ERP_QUARTERLY (viewed Mar 2017).
- Australian Bureau of Statistics. 4177.0. Participation in sport and physical recreation, Australia, 2013–14. Feb 2015. http://www.abs.gov.au/ausstats/abs@.nsf/mf/4177.0 (viewed Mar 2017).
- Mitchell R, Finch C, Boufous S, Browne G. Examination of triage nurse text narratives to identify sports injury cases in emergency department presentations. Int J Inj Contr Saf Promot 2009; 16: 153-157.
- National Health and Medical Research Council. National statement on ethical conduct in human research (2007). Updated May 2015. https://www.nhmrc.gov.au/guidelines-publications/e72 (viewed Mar 2017).
- Finch C, Valuri G, Ozanne-Smith J. Sport and active recreation injuries in Australia: evidence from emergency department presentations. Br J Sports Med 1998; 32: 220-225.
- Padegimas EM, Stepan JG, Stoker GE, et al. Epidemiology and severity of sports and recreation injuries presenting to a tertiary adult emergency department. Phys Sportsmed 2016; 44: 263-268.
- Mitchell R, Finch C, Boufous S. Counting organised sport injury cases: evidence of incomplete capture from routine hospital collections. J Sci Med Sport 2010; 13: 304-308.
- Navaratnam D. Women's growth helps hit record numbers [media release]. AFL.com [website] 30 Nov 2017. http://www.afl.com.au/news/2017-11-30/football-participation-hits-record-numbers (viewed Jan 2018).
- Victoria home to second highest cricket participation in Australia. Australasian Leisure Management [website] 23 Aug 2016. https://www.ausleisure.com.au/news/victoria-home-to-second-highest-cricket-participation-in-australia/ (viewed Jan 2018).
Linked content
-
MJA Research: Traumatic cricket-related fatalities in Australia: a historical review of media reports
-
MJA Editorial: Preventing recreational sports injuries: practicalities and governance