




The known International studies have found that ease of access to tobacco is associated with more smoking behaviour, including initiation by young people and reduced rates of cessation. The distribution of tobacco retail outlets and the relationship between access and smoking in Australia are not well characterised.
The new We identified a disproportionate concentration of tobacco outlets in socio-economically disadvantaged and in outer regional and geographically remote areas of Tasmania.
The implications There is increasing interest in progressive retail restrictions for achieving further gains in tobacco control. Such restrictions could be effective in reducing the disproportionate density of tobacco retail outlets in socio-economically deprived and remote settings.
Australia is known for its progressive tobacco control measures, such as plain packaging.1 Despite reductions in the prevalence of tobacco smoking in Australia in recent decades, it remains a leading modifiable risk factor for morbidity and mortality.2 The burden of tobacco smoking and related harms disproportionately affects the socio-economically disadvantaged and those living in regional or remote Australia.3 With just under one-fifth of its adult population identifying as current smokers, Tasmania has the second highest smoking prevalence in Australia.2,4 The widespread availability of tobacco is at odds with the known harms of tobacco smoking and is an area where further gains in tobacco control could be achieved.
Emerging evidence suggests that greater retail availability of tobacco (ie, the density and proximity of tobacco retail outlets) is associated with higher levels of smoking, particularly with increased experimentation and uptake by young people and reduced numbers of successful cessation attempts by established smokers.5,6 It is hypothesised that restricting the retail availability of tobacco reduces smoking behaviour by decreasing the ease (and increasing the cost) of obtaining tobacco, denormalising smoking, reducing potential cues for smoking, and by supporting public health messages about its harms.7,8
The relationship between tobacco outlet density and smoking behaviour has mainly been described by overseas studies. The retail availability of tobacco has been well defined in the international literature, including the apparent concentration of outlets in areas of socio-economic disadvantage.6,9 In comparison, our understanding of the retail availability of tobacco in Australia is limited. Publications on tobacco retail outlet numbers have been limited to studies in New South Wales, but the once-off registration scheme in this state (tobacco retailers are required to notify the Ministry of Health only once) means that the true availability of tobacco remains unclear.10-12 Two studies, one each in Western Australia and NSW, explored the distribution of tobacco retail outlets by area remoteness and socio-economic status, and identified a significant inverse relationship between tobacco outlet density and socio-economic status.12,13
The effectiveness of population-level interventions that limit the retail availability of alcohol in reducing alcohol-related harm provides an impetus for exploring similar strategies in tobacco control.14 In order to develop evidence-based policies on the retail availability of tobacco, the current retail availability of tobacco in Australia must be known. We therefore aimed to describe the retail availability of tobacco in Tasmania according to area remoteness and socio-economic status.
Methods
We used an ecological cross-sectional research design to examine the relationship between tobacco retail outlet density and area-level socio-economic status and remoteness.
Data sources
Under the Public Health Act (1997), all tobacco retailers in Tasmania are required to hold a licence to sell tobacco, and the licence must be renewed annually. The Tobacco Seller’s Licence database maintained by the Department of Health and Human Services (Tasmania) is a complete record of all issued licences; internal audits have validated the accuracy of the database. Unlicensed tobacco retailers are only rarely identified. A systematic search of the Tobacco Seller’s Licence database identified current licence holders in Tasmania at 31 December 2016. The retail outlets were mapped at the geographical level of Statistical Areas Level 2 (SA2) of the Australian Standard Geographical Classification with geographic information software (ArcGIS 10.5; Environmental Systems Research Institute). SA2s are medium size geographical classifications intended to represent communities that interact socially and economically, typically including a population of 10 000 individuals.15
Population counts for each SA2 were extracted from the 2011 Census of Population and Housing by the Australian Bureau of Statistics (ABS). The entire resident Tasmanian population (all age ranges) was included in the analyses. Population was used as the denominator for calculating tobacco outlet density per 1000 residents.16
Geographical areas were classified as very remote, remote, outer regional, inner regional, or major cities according to the 2011 Remoteness Areas classification for Australia (outlined in the Remoteness Structure of the Australian Statistical Geographical Standard).17
The 2011 ABS Index of Relative Socioeconomic Advantage and Disadvantage (IRSAD) scores assigned to SA2s were used in our analysis. IRSAD is a composite measure of socio-economic conditions, such as employment status, household income, and occupation. The IRSAD is a relative score; lower values indicate greater socio-economic disadvantage.18
Statistical analysis
Tobacco outlet density per 1000 residents was calculated for each geographical region at the SA2 level. Poisson regression was undertaken with post hoc Holm correction to correct for multiple pairwise comparisons; the regression model was assessed for overdispersion. Poisson regression was used to calculate the rate ratios of tobacco outlet density in the comparison groups relative to two reference groups: SA2s classified as inner regional (no SA2s in Tasmania are classified as major city) and SA2s in the highest IRSAD quartile (least socio-economic disadvantage). Results were also geographically aggregated as “Greater Hobart” and “Tasmania, excluding Greater Hobart” as defined by the ABS Greater Capital City Statistical Area classification.15 The rationale for this aggregation was that the retail environment in Hobart might differ from the remainder of the state. Statistical analyses were performed in the statistical package R, version 3.4.0 (R Foundation for Statistical Computing).
Ethics approval
This study was conducted within the Tobacco Control Unit of Public Health Services at the Department of Health and Human Services. The analysis involved routinely collected administrative data geocoded at a level that precluded identification of individual businesses in the published results. The analysis was conducted with the approval of the data custodian, the Director of Public Health, and further ethics approval for this study was therefore not required.
Results
At 31 December 2016, 769 current tobacco licences had been issued in Tasmania, an average of 1.54 tobacco retailers per 1000 residents, or one outlet per 650 Tasmanians (Box 1). There was notable variation between SA2s in the density of tobacco retail outlets (range, 0–6.44 per 1000 residents).
Tobacco outlet density by remoteness
Suburbs or towns in outer regional, remote, and very remote Tasmania had 79% more tobacco outlets per 1000 persons than inner regional Tasmania (rate ratio [RR], 1.79; 95% confidence interval [CI], 1.29–2.50; P < 0.001). A relationship between tobacco outlet density and increasing remoteness was evident; in outer regional Tasmania the density was 62% greater (RR, 1.62; 95% CI, 1.42–2.29; P = 0.013) and in very remote Tasmania it was more than four times as great (RR, 4.27; 95% CI, 2.03–8.00; P < 0.001) than in inner regional Tasmania (Box 2).
Tobacco outlet density by socio-economic status
Across Tasmania, the density of tobacco outlets in suburbs or towns in the lowest two IRSAD quartiles was twice as great as in areas in the highest IRSAD quartile (very low v very high quartile: RR, 2.30; 95% CI, 1.32–4.21; P = 0.014; low v very high quartile: RR, 2.24; 95% CI, 1.30–4.09; P = 0.011). A relationship between density and socio-economic status was found for the Greater Hobart region, but differences between IRSAD quartiles were not statistically significant. Outside the Greater Hobart region, the density of outlets in towns and suburbs in the two lowest IRSAD quartiles was significantly higher than in those in the highest IRSAD quartile (very low v very high quartile: RR, 2.01; 95% CI, 1.10–3.88; P = 0.029; low v very high quartile: RR, 2.31; 95% CI, 1.29–4.44; P = 0.017) (Box 3). Four SA2s were excluded from the socio-economic analysis (and the remoteness analysis) because they were not representative of residential areas: two wilderness areas, and two shopping precincts comprised predominantly of retail outlets with minimal resident population.
Discussion
The density of tobacco outlets was greater in outer regional, remote and very remote Tasmania than in inner regional areas, and in areas characterised by socio-economic disadvantage. We thus found a social disparity in tobacco outlet density, as previously reported for WA and NSW,12,13 confirming that the social gradient in tobacco retail availability is not restricted to these two states.
The prevalence of smoking and smoking-related diseases is greater in socio-economically deprived population groups and among those living in remote and regional Australia.3 The observed inequality of tobacco outlet distribution may reflect demand, but is also likely to contribute to consumption. The NSW analysis found that the gradient in tobacco outlet density persisted despite controlling for smoking prevalence at the local government area level, suggesting that the disparity in outlet distribution may reflect tobacco industry tactics.12 For example, encouraging tobacco supply in disadvantaged neighbourhoods where smoking rates are higher than in the general population is likely to create a social and commercial environment that further encourages smoking behaviour. Evidence from international cross-sectional studies suggests that tobacco outlet density and proximity are associated with youth experimentation, smoking by young people and adults, and reduced success in cessation attempts by established smokers.5-7 Socio-economic disadvantage is an independent risk factor for poorer health outcomes.19 The concentration of tobacco outlets in socio-economically deprived suburbs and towns may further exacerbate health inequities.
A combination of retail restrictions — including licensing, display restrictions at the point of sale, and compliance checks to prevent sales to minors — are important strategies in tobacco retail regulation.20 No jurisdictions in Australia currently restrict the number or locations of tobacco retail outlets, and the international experience is also limited. Land use tools, including zoning ordinances and conditional use permits, have been employed in California to restrict the location of tobacco retailers.21 In 2014, in acknowledgement of the disproportionate clustering of tobacco outlets in poorer neighbourhoods, San Francisco introduced a cap of 45 tobacco retailers per legislative district, and banned outlets within 500 feet of schools.22
Whether this type of progressive retail restriction is effective in reducing individual smoking behaviour or overall smoking prevalence has not been evaluated in formal studies. However, epidemiological modelling has shown that retail outlet interventions, such as reducing outlet numbers or limiting outlets near areas frequented by youths, may achieve modest reductions in population-level smoking prevalence.8 Additionally, a modelling study in the United States found that restricting outlets from operating near schools would be effective in reducing the disparity in tobacco retailer density in socio-economically deprived neighbourhoods.23 Reductions in smoking prevalence are mediated by increases in the time, effort, and incidental costs associated with obtaining tobacco. Individuals of low socio-economic status are most sensitive to changes in tobacco pricing.24 As a result, tobacco retailing restrictions may be particularly effective in reducing smoking prevalence in areas of socio-economic disadvantage, and may therefore have positive equity effects.
While the public appear to support progressive retail measures for reducing the prevalence of smoking, the intended and unintended implications of such a policy require further exploration.25 Further research into the effectiveness and social equity of progressive restrictions that limit the number or location of tobacco retail outlets is needed to inform evidence-based tobacco control policy, particularly for socio-economically deprived and rural areas. The unintended consequences of concentrating tobacco sales in fewer, larger outlets may result in discounted tobacco prices and encourage larger purchases by smokers for stockpiling. Additionally, restricting outlets according to geographic region or socio-economic profile might be perceived as discriminatory.20
The nature of the tobacco licensing system in Tasmania means that our findings offer a complete picture of the retail availability of tobacco in this state. Limitations of our study include the fact that population and socio-economic indices were based on the 2011 ABS Census of Population and Housing, whereas the tobacco outlet data were current for 31 December 2016. Additionally, our analysis did not account for smoking prevalence, which is a potentially important confounding variable. Smoking prevalence data at the SA2 level are not available for Tasmania, and estimates at the level of local government area would be too crude. Interestingly, a similar analysis found that the association between area socio-economic status and tobacco outlet density was independent of smoking prevalence.12 We were not able to adjust our analyses for business type because this characteristic is inconsistently classified in the Tobacco Seller’s Licence database. Adjusting for business type may provide insight into the rise in outlet density with increasing remoteness. Regional and remote towns may have a relatively greater concentration of businesses, such as general stores and mixed businesses, that stock a wide range of common consumer goods, including tobacco. Additional limitations include the assumption that a current tobacco seller’s licence corresponds to an active tobacco retail outlet. The acquisition of tobacco sales data would overcome this limitation, but were not available at the time of our analysis.
It would be interesting to assess tobacco retail density in areas with higher populations of children and young people. However, it is difficult to identify such areas in the datasets we analysed, as the areas in which children live may not correspond to where they attend school or participate in recreational activities.
Conclusion
Tobacco retail outlets are concentrated in areas of socio-economic disadvantage, and their density is higher in outer regional, remote, and very remote Tasmania than in inner regional areas. These social and geographical gradients may exacerbate the health inequities experienced by these populations. A supply-focused tobacco control policy that restricts the retail availability of tobacco is an approach that could further reduce the prevalence of smoking. However, the evidence base for assessing the effectiveness of a policy that restricts the number or placement of tobacco retail outlets is limited. Further investigation of the intended and unintended consequences of such measures is required to inform evidence-based tobacco control policy, particularly for socio-economically deprived and rural areas.
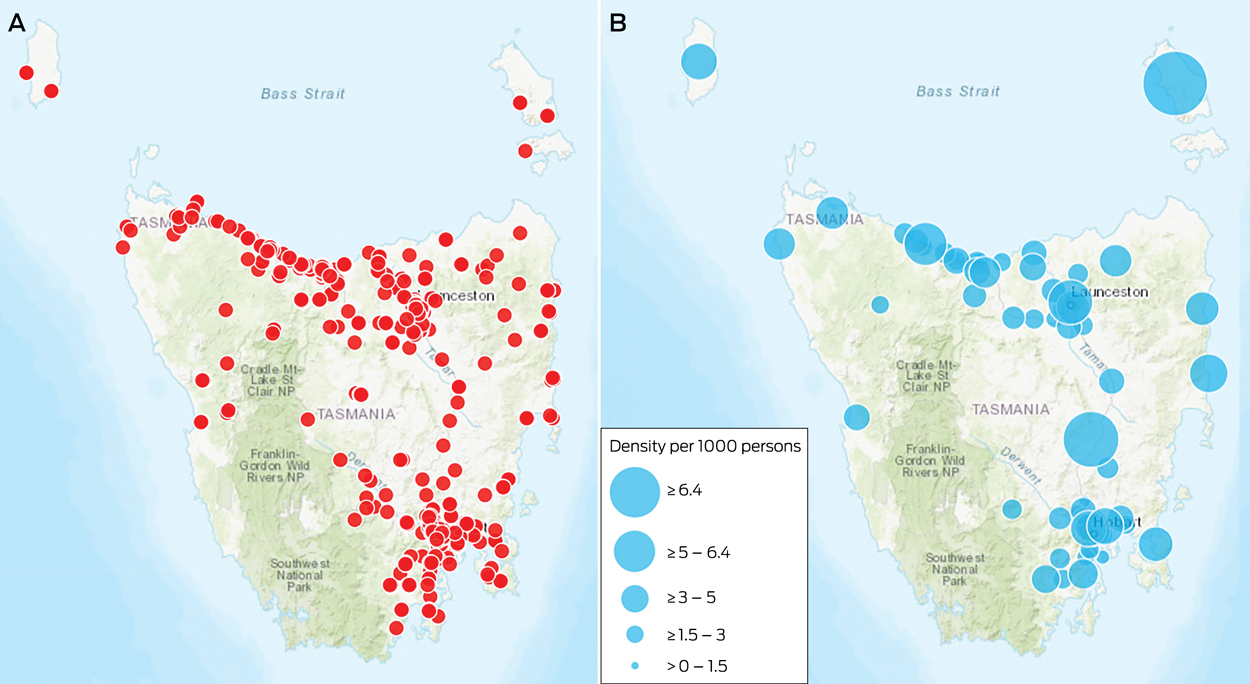
Box 1 – Geographic distribution of tobacco retail outlets in Tasmania, 2016. A, Location of retail outlets; B, outlet density per 1000 residents, by geographic area (at level of Statistical Areas 2)
Box 2 – Tobacco outlet density in Tasmania, 2016, by remoteness classification
|
Remoteness classification |
Tobacco outlet density |
Rate ratio |
P |
||||||||||||
|
|
|||||||||||||||
|
Inner regional |
1.13 |
1 |
|
||||||||||||
|
Outer regional |
1.82 |
1.62 (1.42–2.29) |
0.013 |
||||||||||||
|
Remote |
2.68 |
2.38 (0.87–5.24) |
0.054 |
||||||||||||
|
Very remote |
4.81 |
4.27 (2.03–8.00) |
< 0.001 |
||||||||||||
|
Outer regional, remote, very remote combined |
2.02 |
1.79 (1.29–2.50) |
< 0.001 |
||||||||||||
|
|
|||||||||||||||
|
|
|||||||||||||||
Box 3 – Tobacco outlet density of towns and suburbs in Tasmania, 2016, by area-level (Statistical Areas 2 [SA2]) Index of Relative Socioeconomic Advantage and Disadvantage (IRSAD) quartile*
|
IRSAD quartile |
Tasmania |
Greater Hobart region |
Rest of Tasmania |
||||||||||||
|
Density |
Rate ratio |
P |
Density |
Rate ratio |
P |
Density |
Rate ratio |
P |
|||||||
|
|
|||||||||||||||
|
Very high |
0.82 |
1 |
|
0.93 |
1 |
|
1.04 |
1 |
|
||||||
|
High |
1.32 |
1.60 |
0.13 |
0.83 |
0.89 |
1.0 |
1.35 |
1.29 |
0.46 |
||||||
|
Low |
1.84 |
2.24 |
0.011 |
1.11 |
1.19 |
1.0 |
2.41 |
2.31 |
0.017 |
||||||
|
Very low |
1.89 |
2.30 |
0.014 |
1.46 |
1.57 |
0.88 |
2.09 |
2.01 |
0.029 |
||||||
|
|
|||||||||||||||
|
* Analysis excluded four areas not representative of residential suburbs (wilderness areas, such as kunanyi/Mount Wellington, and geographic areas consisting entirely of shopping precincts). |
|||||||||||||||
Received 6 August 2017, accepted 19 December 2017
- Shannon M Melody1,2
- Veronica Martin-Gall2
- Ben Harding3
- Mark GK Veitch2
- 1 Menzies Institute for Medical Research, University of Tasmania, Hobart, TAS
- 2 Department of Health and Human Services, Hobart, TAS
- 3 Department of Health and Human Services, Launceston, TAS
Shannon Melody is funded by the Australian Department of Health Specialist Training Program. The authors acknowledge Scott McKeown for his feedback on the manuscript.
No relevant disclosures.
- 1. Daube M, Eastwood P, Mishima M, Peters M. Tobacco plain packaging: the Australian experience. Respirology 2015; 20: 1001-1003.
- 2. Australian Bureau of Statistics. 4364.0.55.001. Australian Health Survey: first results, 2014–15. Dec 2015. http://www.abs.gov.au/ausstats/abs@.nsf/mf/4364.0.55.001 (viewed Feb 2017).
- 3. Greenhalgh E, Bayly M, Winstanley M. Trends in the prevalence of smoking by socio-economic status. In: Scollo M, Winstanley M, editors. Tobacco in Australia: facts and issues. Melbourne: Cancer Council Victoria, 2015. http://www.tobaccoinaustralia.org.au/chapter-1-prevalence/1-7-trends-in-the-prevalence-of-smoking-by-socioec (viewed Feb 2017).
- 4. Australian Institute of Health and Welfare. National Drug Strategy Household Survey: detailed report 2013 (AIHW Cat. No. PHE 183). Canberra: AIHW, 2014.
- 5. Halonen JI, Kivimäki M, Kouvonen A, et al. Proximity to a tobacco store and smoking cessation: a cohort study. Tob Control 2013; 23: 146-151.
- 6. Novak SP, Reardon SF, Raudenbush SW, Buka SL. Retail tobacco outlet density and youth cigarette smoking: a propensity-modeling approach. Am J Public Health 2006; 96: 670-676.
- 7. Chuang Y-C, Cubbin C, Ahn D, Winkleby MA. Effects of neighbourhood socioeconomic status and convenience store concentration on individual level smoking. J Epidemiol Community Health 2005; 59: 568-573.
- 8. Pearson AL, van der Deen FS, Wilson N, et al. Theoretical impacts of a range of major tobacco retail outlet reduction interventions: modelling results in a country with a smoke-free nation goal. Tob Control 2015; 24: e32-e38.
- 9. Yu D, Peterson N, Sheffer M, et al. Tobacco outlet density and demographics: analysing the relationships with a spatial regression approach. Public Health 2010; 124: 412-416.
- 10. Feletto E, Burton S, Williams K, et al. Who stops selling? A systematic analysis of ex-tobacco retailers. Tob Control 2017; 26: 164-168.
- 11. Paul CL, Mee KJ, Judd TM, et al. Anywhere, anytime: retail access to tobacco in New South Wales and its potential impact on consumption and quitting. Soc Sci Med 2010; 71: 799-806.
- 12. Kite J, Rissel C, Greenaway M, Williams K. Tobacco outlet density and social disadvantage in New South Wales, Australia. Tob Control 2014; 23: 181-182.
- 13. Wood LJ, Pereira G, Middleton N, Foster S. Socioeconomic area disparities in tobacco retail outlet density: a Western Australian analysis. Med J Aust 2013; 198: 489-491. <MJA full text>
- 14. Martineau F, Tyner E, Lorenc T, et al. Population-level interventions to reduce alcohol-related harm: an overview of systematic reviews. Prev Med 2013; 57: 278-296.
- 15. Australian Bureau of Statistics. 1270.0.55.001. Australian Statistical Geography Standard (ASGS). Volume 1: main structure and greater capital city statistical areas, July 2011. Dec 2010. http://www.abs.gov.au/AUSSTATS/abs@.nsf/allprimarymainfeatures/9593E06A9325683BCA257FED001561EA?opendocument (viewed Mar 2017).
- 16. Australian Bureau of Statistics. 2033.0.55.001. Census of population and housing: Socio-Economic Indexes for Areas (SEIFA), Australia, 2011. Mar 2013. http://www.abs.gov.au/AUSSTATS/abs@.nsf/DetailsPage/2033.0.55.0012011?OpenDocument (viewed Mar 2017).
- 17. Australian Bureau of Statistics. Australian Statistical Geography Standard (ASGS). Volume 5: remoteness structure, July 2011. Jan 2013. http://www.abs.gov.au/ausstats/abs@.nsf/mf/1270.0.55.005 (viewed Mar 2017).
- 18. Australian Bureau of Statistics. 2033.0.55.001. Socio-economic Indexes for Areas (SEIFA), Australia, 2011. Mar 2013. http://www.abs.gov.au/ausstats/abs@.nsf/mf/2033.0.55.001 (viewed Mar 2017).
- 19. Marmot M. Social determinants of health inequalities. Lancet 2005; 365: 1099-1104.
- 20. Smyth C, Freeman B, Maag A. Tobacco retail regulation: the next frontier in tobacco control? Public Health Res Pract 2015; 25: e253152.
- 21. McLaughlin I. License to kill? Tobacco retailer licensing as an effective enforcement tool. Saint Paul (MN): Tobacco Control Legal Consortium, 2010. http://www.publichealthlawcenter.org/sites/default/files/resources/tclc-syn-retailer-2010.pdf (viewed Nov 2017).
- 22. Bright Research Group; for the San Francisco Tobacco-Free Project. Reducing tobacco retail density in San Francisco: a case study. San Francisco (CA): San Francisco Department of Public Health, 2016. http://2gahjr48mok145j3z438sknv.wpengine.netdna-cdn.com/wp-content/uploads/Retail-Density-Case-Study-1.27.16-FINAL-to-TFP.pdf (viewed Nov 2017).
- 23. Ribisl KM, Luke DA, Bohannon DL, et al. Reducing disparities in tobacco retailer density by banning tobacco product sales near schools. Nicotine Tob Res 2016; 19: 239-244.
- 24. Scollo M, Bayly M. Impact of price increases on tobacco consumption in Australia. In: Scollo M, Greenhalgh E, editors. Tobacco in Australia: facts and issues. Melbourne: Cancer Council Victoria, 2015. http://www.tobaccoinaustralia.org.au/13-5-impact-of-price-increases-on-tobacco-consumpt (viewed Feb 2015).
- 25. Whyte G, Gendall P, Hoek J. Advancing the retail endgame: public perceptions of retail policy interventions. Tob Control 2014; 23: 160-166.
Abstract
Objectives: To describe the retail availability of tobacco and to examine the association between tobacco outlet density and area-level remoteness and socio-economic status classification in Tasmania.
Design: Ecological cross-sectional study; analysis of tobacco retail outlet data collected by the Department of Health and Human Services (Tasmania) according to area-level (Statistical Areas Level 2) remoteness (defined by the Remoteness Structure of the Australian Statistical Geographical Standard) and socio-economic status (defined by the 2011 Australian Bureau of Statistics Index of Relative Socioeconomic Advantage and Disadvantage).
Main outcome measure: Tobacco retail outlet density per 1000 residents.
Results: On 31 December 2016, there were 1.54 tobacco retail outlets per 1000 persons. The density of outlets was 79% greater in suburbs or towns in outer regional, remote and very remote Tasmania than in inner regional Tasmania (rate ratio [RR], 1.79; 95% confidence Interval [CI], 1.29–2.50; P < 0.001). Suburbs or towns in Tasmania with the greatest socio-economic disadvantage had more than twice the number of tobacco outlets per 1000 people as areas of least disadvantage (RR, 2.30; 95% CI, 1.32–4.21; P = 0.014).
Conclusions: A disproportionate concentration of tobacco retail outlets in regional and remote Tasmania and in areas of lowest socio-economic status is evident. Our findings are consistent with those of analyses in New South Wales and Western Australia. Progressive tobacco retail restrictions have been proposed as the next frontier in tobacco control. However, the intended and unintended consequences of such policies need to be investigated, particularly for socio-economically deprived and rural areas.