





Volume 207 - Issue 4
Diagnosis and management of pancreatic exocrine insufficiency
Authors: Mehrdad Nikfarjam, Jeremy S Wilson and Ross C Smith, Australasian Pancreatic Club Pancreatic Enzyme Replacement Therapy Guidelines Working Group
Med J Aust 2017; 207 (4): 161-165. || doi: 10.5694/mja16.00851
Published online: 21 August 2017
Published online: 21 August 2017
New guidelines classify PEI as definite, possible or unlikely, and provide a diagnostic algorithm for early diagnosis and management
Abstract
Introduction: In 2015, the Australasian Pancreatic Club (APC) published the Australasian guidelines for the management of pancreatic exocrine insufficiency (http://pancreas.org.au/2016/01/pancreatic-exocrine-insufficiency-guidelines). Pancreatic exocrine insufficiency (PEI) occurs when normal digestion cannot be sustained due to insufficient pancreatic digestive enzyme activity. This may be related to a breakdown, at any point, in the pancreatic digestive chain: pancreatic stimulation; synthesis, release or transportation of pancreatic enzymes; or synchronisation of secretions to mix with ingested food.
Main recommendations: The guidelines provide advice on diagnosis and management of PEI, noting the following:
- A high prevalence of PEI is seen in certain diseases and conditions, such as cystic fibrosis, acute and chronic pancreatitis, pancreatic cancer and pancreatic surgery.
- The main symptoms of PEI are steatorrhoea or diarrhoea, abdominal pain, bloating and weight loss. These symptoms are non-specific and often go undetected and untreated.
- PEI diagnosis is predominantly based on clinical findings and the presence of underlying disease. The likelihood of PEI in suspected patients has been categorised into three groups: definite, possible and unlikely.
- If left untreated, PEI may lead to complications related to fat malabsorption and malnutrition, and have an impact on quality of life.
- Pancreatic enzyme replacement therapy (PERT) remains the mainstay of PEI treatment with the recommended adult initial enzyme dose being 25 000–40 000 units of lipase per meal, titrating up to a maximum of 75 000–80 000 units of lipase per meal.
- Adjunct acid-suppressing therapy may be useful when patients still experience symptoms of PEI on high dose PERT.
- Nutritional management by an experienced dietitian is essential.
Changes in management as a result of these guidelines: These are the first guidelines to classify PEI as being definite, possible or unlikely, and provide a diagnostic algorithm to facilitate the early diagnosis of PEI and appropriate use of PERT.
Pancreatic exocrine insufficiency (PEI) occurs when normal digestion cannot be maintained due to insufficient pancreatic digestive enzyme activity in the small intestines.1 PEI has non-specific symptoms shared with other pancreatic diseases and gastrointestinal conditions2-4 and can result from damage to the pancreas where gross alteration of structure or functional change occurs.1
The main clinical PEI symptoms are steatorrhoea or diarrhoea, abdominal pain and weight loss.5 If left untreated, PEI can lead to malnutrition and related complications,6 as well as poor quality of life due to persistent gastrointestinal symptoms.7,8 An early and accurate PEI diagnosis and successful treatment are clinically important and of clear benefit to patients.5
Methods
This article summarises the Australasian guidelines for the management of pancreatic exocrine insufficiency, published by the Australasian Pancreatic Club (APC) in 2015.9 The guidelines apply a diagnostic algorithm to categorise patients into three groups based on the likelihood of PEI: definite, possible, and unlikely.9 The recommendations are based on the Oxford Centre for Evidence-based Medicine system for grading the level of evidence (http://www.cebm.net/oxford-centre-evidence-based-medicine-levels-evidence-march-2009), with the addition of level 3c: critical review of literature (Box 1). Strength of agreement for recommendations was gauged through electronic questionnaires distributed to the members of the working group.
Recommendations
Prevalence
A number of diseases and conditions are known to be associated with PEI. For example, PEI is estimated to occur in 94% of patients with chronic pancreatitis (10–15 years after clinical onset);10,11 > 85% of patients with cystic fibrosis;12-14 74% of patients after pancreatic resection surgery;15 and 92% of patients with unresectable pancreatic cancer.16 The general level of PEI prevalence (high to low probability) can be assigned to different patient populations (Box 2).9
There are limited reliable data on the prevalence of PEI in the general population.5 PEI often goes undetected and patients referred from primary care may not represent the majority of PEI sufferers within the community.3,4,17,18
Pathophysiology
Various factors, including extrapancreatic conditions, may reduce pancreatic enzyme activity within the intestinal lumen if they interrupt the chain of events required for normal meal digestion. Failure at any stage in the process — which includes pancreatic stimulation, synthesis and release of digestive enzymes by pancreatic acinar cells, enzyme transportation through the duct system, and synchronised mixing of the pancreatic secretions with ingested food — may lead to PEI.5
The pathophysiology of PEI has four possible aetiologies:1
-
Damage: the pancreatic parenchyma is no longer able to synthesise the required amounts of digestive enzymes.
-
Asynchrony: dissociation of normal postprandial digestive enzyme secretions and intestinal meal delivery. This can occur in conditions such as short bowel syndrome, Crohn’s disease or after gastric, biliary or pancreatic resections or bypass procedures.
-
Obstruction: pancreatic duct blockage affects the transport of digestive enzymes and other secretions into the duodenum.
-
Decreased endogenous stimulation: decreased stimulation of enzyme production is particularly noted with coeliac disease.
Pancreatic exocrine secretions may be substantially reduced without producing clinical manifestations of PEI.5 Pancreatic lipases, for example, need to be reduced to 5–10% of normal postprandial levels before steatorrhoea, the main PEI clinical symptom, is evident.19 This is linked to compensatory enzyme mechanisms and the high reserve capacity of the pancreas.19 The mechanisms for development of PEI and its clinical consequences are summarised in Box 3.
Diagnosis
The symptoms of PEI are gastrointestinal-related and non-specific. If undiagnosed, patients may have ongoing symptoms such as diarrhoea and abdominal pain that can sometimes be mistaken as a functional bowel disorder.3,18 PEI symptoms can vary from patient to patient, and are dependent on the degree of PEI experienced and its aetiology.5
In practice, an initial suspicion of PEI is based on the clinical assessment of the patient, self-reported bowel movements, and weight loss (or failure to thrive in children). However, an important factor to remember is that the reliance on patient symptoms alone may lead to under- or overdiagnosis.5
Morphological and functional assessments can be made to confirm diagnosis (Box 4). Initially, computed tomography can identify gross pancreatic structural changes and is readily available. However, these changes are not always specific and may require further investigation with magnetic resonance imaging, endoscopic ultrasound and, rarely, secretin-enhanced magnetic resonance cholangiopancreatography or endoscopic retrograde cholangiopancreatography.9,20,21 Additionally, PEI may still occur in patients with a morphologically normal pancreas.22 Direct functional tests, such as the secretin–cholecystokinin stimulation test and endoscopic pancreatic function test, involve the collection of pancreatic secretions while the pancreas is stimulated.5 Direct tests are sensitive and specific, but are also invasive, costly and therefore have limited routine clinical use.23 Indirect functional tests (eg, faecal, breath and blood tests) are cheaper and easier to use, but are generally less sensitive and less specific.23 Screening for nutritional markers in the blood, including magnesium, fat-soluble vitamins and lipoproteins, can help assess nutritional deficiencies and may be used to support a PEI diagnoses as well as to monitor treatment effectiveness.5,24,25
The 2015 PEI management guidelines9 graded patients with clinically suspected PEI into three subgroups with corresponding recommended investigations and treatment options (Box 4):
-
PEI definite: if the presentation falls within this group, a diagnosis of PEI can be made solely on clinical grounds. In this situation, gross changes to the pancreas are present (eg, total pancreatectomy or radiologic investigations show severe calcific pancreatitis or neoplasms in the head of the pancreas) along with symptoms suggestive of severe steatorrhoea, weight loss and fat-soluble vitamin deficiency.
-
PEI possible: if only moderate pancreatic structural changes are seen, then a PEI diagnosis is suggested if the patient also presents with nutritional impairment and diarrhoea, although there could be other reasons for these symptoms. The probability of a positive objective test, and therefore response to pancreatic enzyme replacement therapy (PERT), is 30–70%.
-
PEI unlikely: conditions seen within this group may only occasionally be associated with or caused by PEI. PEI symptoms are likely to be seen in < 10% of cases and the probability of a positive objective test and response to PERT is estimated to be < 10%.
Although these guideline recommendations were produced through a consensus process in light of the best available evidence, they are not yet validated.
Complications
If left untreated, PEI can lead to serious complications including:
-
Nutritional deficiencies: malabsorption of micronutrients (including zinc, magnesium, calcium, thiamine and folic acid) and lipid-soluble vitamins increases the risk of malnutrition-related complications.6 Almost two-thirds of patients with chronic pancreatitis have either osteoporosis or osteopenia (combined prevalence rate of 65%).27 PEI in these patients is significantly correlated with reduced bone mineral density and decreased levels of the fat-soluble vitamin D required for normal bone metabolism.27,28
-
Reduced quality of life8,29,30 related to persistent gastrointestinal and pain symptoms, as well as other factors such as inability to work and financial strain.8
-
High morbidity and mortality through the increased risk of malnutrition-related complications and cardiovascular events.31-33
Management
The primary treatment goal for PEI is to restore the normal digestion process in order to maintain adequate nutrition. PEI-related symptoms also need to be alleviated and disease progression prevented.5 The fundamental elements of current PEI management in adults are outlined in the PEI management algorithm in Box 5:5,9,34
-
PERT (evidence level 1b);
-
lifestyle modifications: primarily alcohol abstinence, cessation of smoking and consumption of a well balanced diet (level 5);
-
trial of acid-suppressing agents in patients who continue to experience symptoms of PEI despite high doses of PERT (level 1b);
-
diet adjustments: small frequent meals, normal fat intake and vitamin supplementation (lipid-soluble vitamins A, D, E and K) (level 5); and
-
follow-up of patients: focusing on nutritional deficiencies, symptoms of maldigestion, treatment of any causative diseases and ensuring treatment compliance (level 5).
Pancreatic enzyme replacement therapy
PERT is the mainstay of PEI treatment. Encapsulated microgranules deliver pancreatic extracts (a combination of lipase, amylase and protease) into the duodenal lumen, providing sufficient enzymatic activity so that nutrient digestion is restored and malabsorption is prevented.23
The microgranules are taken with a meal and mix intragastrically with the chyme, but are protected from acid degradation by an enteric coating. They are then released from the stomach along with the chyme into the duodenum. The pH-sensitive coating dissolves in the duodenum’s alkaline environment, releasing the enzymes at the optimum point for digestion and absorption. Variation in enzyme content, the size of the enzyme particles and the dissolution properties of the enteric coating can influence the effectiveness of PERT and the bioequivalence of different formulations.1
Some patients may require adjuvant treatment with acid suppressors (eg, proton pump inhibitors) if the pH of their duodenum is lower than normal (eg, in patients with bicarbonate deficiency; level 1b). A lower pH may affect the dissolution of the enteric coating and reduce the effectiveness of enzymes.1
PEI severity varies from patient to patient, and the relationship between the dose of pancreatic enzymes and response to therapy is not linear. PERT dosage therefore needs to be individually titrated to the lowest effective dose to avoid gastrointestinal complications associated with higher enzyme doses and to prevent treatment burden.5,35-37 Very high doses of PERT have been associated with fibrosing colonopathy, and the maximum dose recommendation is 10 000 units of lipase/kg/day.36
The APC-recommended PERT starting dose for adults is 25 000–40 000 units of lipase (Box 5) (level 3c) taken with each meal (level 2b).9 If there is insufficient response to the initial dose, it should be titrated up to a maximum of 75 000–80 000 units of lipase per meal (level 3c). The guidelines also outline recommended PERT doses for children and infants (including breastfed infants), which may be per gram of dietary fat, per feed or calculated by bodyweight.9
Long term, it is important to monitor and follow up patients with PEI to ensure sufficient PERT response, treat any causative diseases, prevent complications and confirm treatment compliance. If PERT is ineffective even with correct administration, dosage optimisation and adjuvant treatment with acid suppressors (level 1b), other reasons for a poor response should be considered (such as bacterial overgrowth) or the PEI diagnosis may need to be reconsidered.1,31
Nutritional management
Dietary management is an important issue with PEI, and it is essential that patients be referred to a dietitian to oversee the process. Dietary advice should be tailored specifically to the individual patient’s requirements in terms of their nutritional and weight status, macronutrient intake and micronutrient deficiencies. Recommended nutritional assessments carried out by dietitians include:9
-
Aetiology of PEI: recommendations of meal size and frequency, and nutritional supplementation can vary with different diagnoses.
-
Diet history: to establish baseline diet, understand how the patient eats and define alcohol habits (level 5).
-
Malnutrition assessment: additional anthropometric measures (such as mid-arm circumference, mid-arm muscle circumference, triceps skinfold or subjective global assessment) should be used in conjunction with body mass index. Weight and body mass index assessments alone may be misinterpreted, for example, as a result of fluid changes due to ascites or oedema.7
-
Nutritional deficiencies: these are not always clinically apparent, and screening for nutritional markers (including magnesium, fat-soluble vitamins, vitamin B12, iron and lipoproteins) is needed at the time of diagnosis so that appropriate supplements can be given and their status monitored (level 5).
-
Bone health: osteoporosis or osteopenia may be a long term complication of PEI, and early assessment and appropriate treatment is essential (level 2a).
-
Fat requirement: low fat or reduced fat diets are not recommended with optimised PERT. A target of 30% total energy from dietary fat is now considered appropriate, but adverse symptoms such as steatorrhoea need to be monitored (level 5).
Changes in management
PEI is an underdiagnosed and often undertreated condition.3,5,18,38-41 The dilemma for the clinician, therefore, is to be able to determine which patients will benefit from further investigations and PEI treatment. The latest guidelines for the management of PEI, developed by the APC, grade presentation types based on the likelihood of PEI being present (ie, definitely, possibly and unlikely PEI). In this way, the difficulties of diagnosing PEI can be taken into account, while relating the value of investigation and treatment to each diagnostic category.9 The guidelines also provide consensus recommendations on the use of PERT for each category.
Box 1 – Levels of evidence*
|
|
|||||||||||||||
|
1a |
Systematic reviews (with homogeneity) of RCTs |
||||||||||||||
|
1b |
Individual RCTs (with narrow confidence interval) |
||||||||||||||
|
1c |
All or none RCTs |
||||||||||||||
|
2a |
Systematic reviews (with homogeneity) of cohort studies |
||||||||||||||
|
2b |
Individual cohort study or low quality RCTs (eg, < 80% follow-up) |
||||||||||||||
|
2c |
Outcomes research; ecological studies |
||||||||||||||
|
3a |
Systematic review (with homogeneity) of case–control studies |
||||||||||||||
|
3b |
Individual case–control study |
||||||||||||||
|
3c |
Critical review of the literature, including multiple experimental and observational studies |
||||||||||||||
|
4 |
Case series (and poor quality cohort and case–control studies) |
||||||||||||||
|
5 |
Expert opinion without explicit critical appraisal, or based on physiology, bench research or first principles |
||||||||||||||
|
|
|||||||||||||||
|
RCT = randomised controlled trial. * Adapted from the Australasian Pancreatic Club guidelines,9 based on the Oxford Centre for Evidence-based Medicine system for grading the level of evidence (http://www.cebm.net/oxford-centre-evidence-based-medicine-levels-evidence-march-2009). |
|||||||||||||||
Box 2 – Likelihood of pancreatic exocrine insufficiency (PEI) in various patient populations*
|
Patient group† |
Likelihood of PEI |
||||||||||||||
|
|
|||||||||||||||
|
Cystic fibrosis (pancreatic insufficiency) |
100% (definite) |
||||||||||||||
|
Total pancreatectomy |
|||||||||||||||
|
Severe chronic pancreatitis (with calcific changes, steatorrhoea, weight loss) |
|||||||||||||||
|
Tumour destroying head of pancreas |
|||||||||||||||
|
Acute pancreatitis destroying head of pancreas |
|||||||||||||||
|
Mild and moderate chronic pancreatitis |
30–70% (possible) |
||||||||||||||
|
After severe acute pancreatitis |
|||||||||||||||
|
After severe pancreatitis |
|||||||||||||||
|
After pancreatic surgery (Whipple procedure)‡ |
|||||||||||||||
|
Type 2 diabetes |
< 10% (unlikely) |
||||||||||||||
|
Irritable bowel syndrome |
|||||||||||||||
|
Coeliac disease |
|||||||||||||||
|
Inflammatory bowel disease |
|||||||||||||||
|
Older people (with weight loss) |
|||||||||||||||
|
Bowel resection |
|||||||||||||||
|
|
|||||||||||||||
|
* Adapted from the Australasian Pancreatic Club guidelines.9 † Diseases and conditions either associated with or known to cause PEI. ‡ After pancreatic surgery in the setting of pancreatic cancer (which is often associated with chronic pancreatitis) and in the setting of chronic pancreatitis alone may be more definite indications for PEI. |
|||||||||||||||
Box 3 – Mechanisms for the development of pancreatic exocrine insufficiency and its clinical consequences*
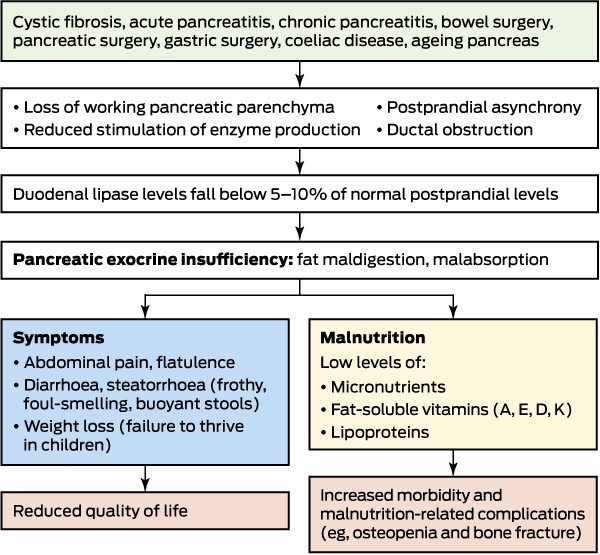
* Adapted from the Australasian Pancreatic Club guidelines.9
Box 4 – Pancreatic exocrine insufficiency (PEI): diagnostic pathway*
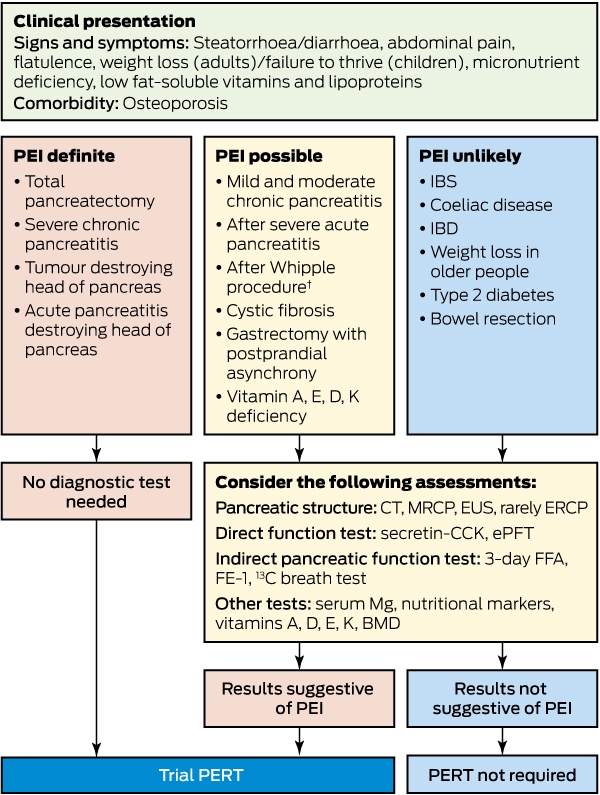
BMD = bone mineral density. CCK = cholecystokinin. CT = computed tomography. ePFT = endoscopic pancreatic function test. ERCP = endoscopic retrograde cholangiopancreatography. EUS = endoscopic ultrasound. FE-1 = faecal elastase-1. FFA = faecal fat analysis. IBD = inflammatory bowel disease. IBS = irritable bowel syndrome. Mg = magnesium. MRCP = magnetic resonance cholangiopancreatography. PERT = pancreatic enzyme replacement therapy. * Adapted from the Australasian Pancreatic Club guidelines.9 † After pancreatic surgery in the setting of pancreatic cancer (which is often associated with chronic pancreatitis) may be a more definite indication for PEI.
Box 5 – Pancreatic exocrine insufficiency (PEI) management (adults)
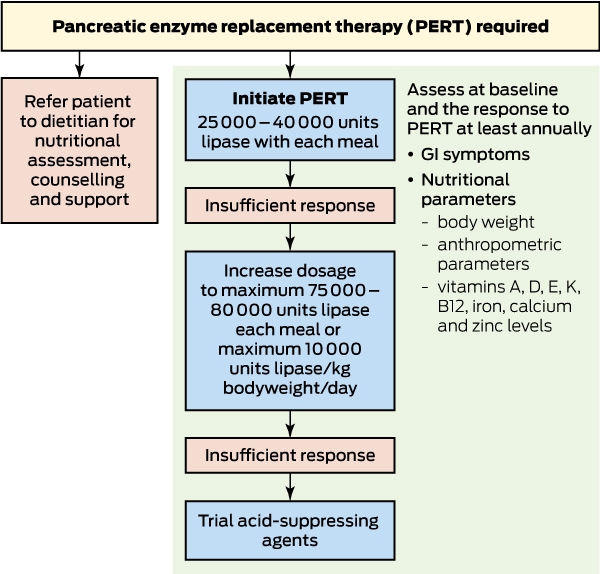
* Adapted from the Australasian Pancreatic Club guidelines.9
Competing interests
The APC has received unrestricted educational funding from Mylan Pharmaceuticals. There has been no funding directed to any of the authors in relation to this article or the production of the APC guidelines for the management of PEI.
Acknowledgements
Members of the APC PERT Guidelines Working Group are listed in the full guidelines available at http://pancreas.org.au/2016/01/pancreatic-exocrine-insufficiency-guidelines. We thank Ergo Advertising for their assistance in creating the flowcharts in this article and editing earlier versions of the manuscript.
References
- Keller J, Layer P. Human pancreatic exocrine response to nutrients in health and disease. Gut 2005; 54 Suppl 6: vi1-28.
- Keane MG, Horsfall L, Rait G, Pereira SP. A case-control study comparing the incidence of early symptoms in pancreatic and biliary tract cancer. BMJ Open 2014; 4: e005720.
- Campbell J, Sanders D, Francis K, et al. Should we investigate gastroenterology patients for pancreatic exocrine insufficiency? A dual centre UK study. J Gastrointestin Liver Dis 2016; 25: 303-309.
- Leeds JS, Hopper AD, Sidhu R. et al. Some patients with irritable bowel syndrome may have exocrine pancreatic insufficiency. Clin Gastroenterol Hepatol 2010; 8: 433-438.
- Lindkvist B. Diagnosis and treatment of pancreatic exocrine insufficiency. World J Gastroenterol 2013; 19: 7258-7266.
- Lindkvist B, Domínguez-Muñoz JE, Luaces-Regueira M, et al. Serum nutritional markers for prediction of pancreatic exocrine insufficiency in chronic pancreatitis. Pancreatology 2012; 12: 305-310.
- Rasmussen HH, Irtun O, Olesen SS, et al. Nutrition in chronic pancreatitis. World J Gastroenterol 2013; 19: 7267-7275.
- Czako L, Takács T, Hegyi P, et al. Quality of life assessment after pancreatic enzyme replacement therapy in chronic pancreatitis. Can J Gastroenterol 2003; 17: 597-603.
- Australasian Pancreatic Club. Australasian guidelines for the management of pancreatic exocrine insufficiency. October 2015. http://pancreas.org.au/2016/01/pancreatic-exocrine-insufficiency-guidelines (accessed Sept 2016).
- Levy P, Domínguez-Muñoz E, Imrie C, et al. Epidemiology of chronic pancreatitis: burden of the disease and consequences. United European Gastroenterol J 2014; 2: 345-354.
- Dumasy V, Delhaye M, Cotton F, Deviere J. Fat malabsorption screening in chronic pancreatitis. Am J Gastroenterol 2004; 99: 1350-1354.
- Kalivianakis M, Verkade HJ. The mechanisms of fat malabsorption in cystic fibrosis patients. Nutrition 1999; 15: 167-169.
- Littlewood JM. Cystic fibrosis: gastrointestinal complications. Br Med Bull 1992; 48: 847-859.
- Pencharz PB, Durie PR. Pathogenesis of malnutrition in cystic fibrosis, and its treatment. Clin Nutr 2000; 19: 387-394.
- Tseng DS, Molenaar IQ, Besselink MG, et al. Pancreatic exocrine insufficiency in patients with pancreatic or periampullary cancer: A systematic review. Pancreas 2016; 45: 325-330.
- Sikkens EC, Cahen DL, de Wit J, et al. A prospective assessment of the natural course of the exocrine pancreatic function in patients with a pancreatic head tumor. J Clin Gastroenterol 2014; 48: e43-e46.
- Herzig K, Purhonen AK, Räsänen KM, et al. Fecal pancreatic elastase-1 levels in older individuals without known gastrointestinal disease or diabetes mellitus. BMC Geriatr 2011; 11: 4.
- Goepp J, Fowler E, McBride T, Landis D. Frequency of abnormal fecal biomarkers in irritable bowel syndrome. Glob Adv Health Med 2014; 3: 9-15.
- DiMagno EP, Go VL, Summerskill WH. Relations between pancreatic enzyme outputs and malabsorption in severe pancreatic insufficiency. N Engl J Med 1973; 288: 813-815.
- Sai JK, Suyama M, Kubokawa Y, Watanabe S. Diagnosis of mild chronic pancreatitis (Cambridge classification): comparative study using secretin injection-magnetic resonance cholangiopancreatography and endoscopic retrograde pancreatography. World J Gastroenterol 2008; 14: 1218-1221.
- Schneider AR, Hammerstingl R, Heller M, et al. Does secretin-stimulated MRCP predict exocrine pancreatic insufficiency? A comparison with noninvasive exocrine pancreatic function tests. J Clin Gastroenterol 2006; 40: 851-855.
- Terzin V, Varkonyi T, Szabolcs A, et al. Prevalence of exocrine pancreatic insufficiency in type 2 diabetes mellitus with poor glycemic control. Pancreatology 2014; 14: 356-360.
- Domínguez-Muñoz JE. Diagnosis of chronic pancreatitis: functional testing. Best Pract Res Clin Gastroenterol 2010; 24: 233-241.
- Sikkens EC, Cahen DL, Koch AD, et al. The prevalence of fat-soluble vitamin deficiencies and a decreased bone mass in patients with chronic pancreatitis. Pancreatology 2013; 13: 238-242.
- Duggan SN, Smyth ND, O’Sullivan M, et al. The prevalence of malnutrition and fat-soluble vitamin deficiencies in chronic pancreatitis. Nutr Clin Pract 2014; 29: 348-354.
- Trolli PA, Conwell DL, Zuccaro G Jr. Pancreatic enzyme therapy and nutritional status of outpatients with chronic pancreatitis. Gastroenterol Nurs 2001; 24: 84-87.
- Duggan SN, Smyth ND, Murphy A, et al. High prevalence of osteoporosis in patients with chronic pancreatitis: a systematic review and meta-analysis. Clin Gastroenterol Hepatol 2014; 12: 219-228.
- Haas S, Krins S, Knauerhase A, Löhr M. Altered bone metabolism and bone density in patients with chronic pancreatitis and pancreatic exocrine insufficiency. JOP 2015; 16: 58-62.
- Fitzsimmons D, Kahl S, Butturini G, et al. Symptoms and quality of life in chronic pancreatitis assessed by structured interview and the EORTC QLQ-C30 and QLQ-PAN26. Am J Gastroenterol 2005; 100: 918-926.
- D’Haese J, Ceyhan GO, Demir IE, et al. Pancreatic enzyme replacement therapy in patients with exocrine pancreatic insufficiency due to chronic pancreatitis: a 1-year disease management study on symptom control and quality of life. Pancreas 2014; 43: 834-841.
- Domínguez-Muñoz JE. Pancreatic enzyme therapy for pancreatic exocrine insufficiency. Curr Gastroenterol Rep 2007; 9: 116-122.
- Montalto G, Soresi M, Carroccio A, et al. Lipoproteins and chronic pancreatitis. Pancreas 1994; 9: 137-138.
- Vallejo-Senra N, De La Iglesia-Garcia D, Lopez-Lopez A, et al. Cardiovascular risk (CVR) associated with pancreatic exocrine insufficiency (PEI) in patients with chronic pancreatitis (CP). Pancreatology 2016; 16: S1-S130.
- Toouli J, Biankin AV, Oliver MR, et al. Management of pancreatic exocrine insufficiency: Australasian Pancreatic Club recommendations. Med J Aust 2010; 193: 461-467.
- Anthony H, Collins CE, Davidson G, et al. Pancreatic enzyme replacement therapy in cystic fibrosis: Australian guidelines. Pediatric Gastroenterological Society and the Dietitians Association of Australia. J Paediatr Child Health 1999; 35: 125-129.
- Fieker A, Philpott J, Armand M. Enzyme replacement therapy for pancreatic insufficiency: present and future. Clin Exp Gastroenterol 2011; 4: 55-73.
- Konstan MW, Accurso FJ, Nasr SZ, et al. Efficacy and safety of a unique enteric-coated bicarbonate-buffered pancreatic enzyme replacement therapy in children and adults with cystic fibrosis. Clin Investig (Lond) 2013; 3: 723-729.
- Sikkens EC, Cahen DL, van Eijck C, et al. The daily practice of pancreatic enzyme replacement therapy after pancreatic surgery: a northern European survey: enzyme replacement after surgery. J Gastrointest Surg 2012; 16: 1487-1492.
- Landers A, Muircroft W, Brown H. Pancreatic enzyme replacement therapy (PERT) for malabsorption in patients with metastatic pancreatic cancer. BMJ Support Palliat Care 2016; 6: 75-79.
- Ramos LR, Sachar DB, DiMaio CJ, et al. Inflammatory bowel disease and pancreatitis: a review. J Crohns Colitis 2016; 10: 95-104.
- Phillips ME. Pancreatic exocrine insufficiency following pancreatic resection. Pancreatology 2015; 15: 449-455.
Provenance: Not commissioned; externally peer reviewed.