




Abstract
Objective: To describe the frequency, nature and outcomes of reports about health practitioners made by their treating practitioners under Australia’s new mandatory reporting system.
Design and setting: Retrospective case file review and analysis of treating practitioner reports received by the Australian Health Practitioner Regulation Agency between 1 November 2011 and 31 January 2013, and of the outcomes of the completed investigations of these reports to November 2014.
Main outcome measures: Characteristics of treating practitioners and reported practitioners; nature of the care relationship; grounds for report; regulatory action taken in response to report.
Results: Of 846 mandatory reports about medical practitioners, 64 (8%) were by treating practitioners. A minority of reports (14 of 64) were made by a practitioner-patient’s regular care provider; most (50 of 64) arose from an encounter during an acute admission, first assessment or informal corridor consultation. The reported practitioner-patients were typically being treated for mental illness (28 of 64) or substance misuse (25 of 64). In 80% of reports (50 of 64), reporters described practitioner-patients who exhibited diminished insight, dishonesty, disregard for patient safety, or an intention to self-harm.
Conclusions: The nature and circumstances of the typical treating practitioner report challenge assumptions expressed in policy debates about the merits of the new mandatory reporting law. Mandatory reports by treating practitioners are rare. The typical report is about substance misuse or mental illness, is made by a doctor who is not the patient’s regular care provider, and identifies an impediment to safely managing the risk posed by the practitioner-patient within the confines of the treating relationship.
In 2010, the Australian states and territories adopted a national law requiring health practitioners, employers and education providers to report “notifiable conduct” by health practitioners to the appropriate National Health Practitioner Board through the Australian Health Practitioner Regulation Agency (AHPRA). Notifiable conduct encompasses four behaviours: (1) practising while intoxicated by alcohol or drugs; (2) sexual misconduct during the practice of the profession; (3) placing the public “at risk of substantial harm” because of an impairment; or (3) placing the public at risk because of a “significant departure from accepted professional standards”.1 Details of these rules have been published elsewhere.2,3
The mandatory notification law was received with some concern, particularly by doctors and medical professional bodies.2,4 A particularly controversial aspect was its application to practitioners who, in the course of providing care to another practitioner, form a belief that notifiable conduct has occurred. The versions of the law enacted in Western Australia and Queensland allow certain exemptions for practitioners treating other practitioners, but those in force in the other states do not.3
Critics of extending mandatory reporting to care relationships object to the perceived assault on the time-honoured ethics principle of patient confidentiality; they also worry that it will deter impaired practitioners from seeking assistance.5-7 Defenders of the rule argue that treating practitioners have a valuable vantage point from which to identify impaired colleagues, and that requiring them to do so protects the public and enhances trust in the health system.8
Our earlier study of 816 mandatory reports received by AHPRA over a 14-month period2 found that around 8% were made by treating practitioners. In recognition of the importance of these “treating practitioner reports” for policy and practice, we collected and analysed additional data on this subset of reports, and the outcomes of their investigation by AHPRA.
Methods
As part of a larger study of mandatory notification,2 we reviewed all reports received between 1 November 2011 and 31 January 2013. Access to the reports was subject to strict conditions guaranteeing privacy and confidentiality, and study team members signed non-disclosure agreements. The study was approved by the Human Research Ethics Committee at the University of Melbourne (reference, HREC 1239183.2).
The examined reports were from all states and territories except New South Wales, and had been lodged with AHPRA either in a notification form available on the AHPRA website or in letter form. The layout and content of the reports have been previously described.2 Although health practitioners in NSW are subject to the same reporting requirements as those in other states, AHPRA has a more limited role in relation to notifications made in NSW.2
The reports were reviewed between April and June 2013 at the AHPRA head offices in Melbourne. Three trained reviewers extracted de-identified information about the statutory grounds for notification, the type of problem reported, and practitioner characteristics and demographics. This information was supplemented with data from the national register of health practitioners, including information on sex, age, practice location, profession, and the specialties of both the reporter and the subject of the report.
All reports lodged by a treating practitioner about a practitioner-patient were flagged for more detailed review; they formed the focus of our analysis.
A senior investigator (MB) examined each flagged report to verify that it had been submitted by a treating practitioner. She also extracted any free text that discussed the health condition treated, the nature of the treatment relationship, the perceived risk, and steps the reporter took before lodging their report.
Using a grounded theory approach,9 two investigators (MB, DS) reviewed a subsample of the extracts and developed a coding scheme for deriving information on six variables from the free text: primary health condition for which the patient was being treated; the reporter–patient relationship; the timing of the risk; impediments to risk reduction; advice sought on reporting obligations; and disclosure to the patient of the intent to report. Using the finalised coding scheme, one investigator and a second, legally trained reviewer independently coded the textual extracts for all reports.
Comparison of the data coding by the two coders found inter-rater reliability that ranged from good to very good, depending on the variable. For example, the kappa (κ) score for the variable “impediments to risk reduction”, which probably involved more implicit judgment than the other variables, was 0.77.
In November 2014, the outcomes of the response by AHPRA to each case were obtained and added to the analytic dataset. This allowed 18 to 36 months to elapse after the report lodgement dates.
Statistical analyses were conducted with Stata 13.1 (StataCorp).
Results
Of 846 mandatory reports made to National Boards through AHPRA during the study period, 64 (8%) were lodged by health practitioners who had a treating relationship with the subject of the report. The others were lodged by non-treating practitioners, managers, employers or educators. All results reported here relate to the treating practitioner reports.
Sample characteristics
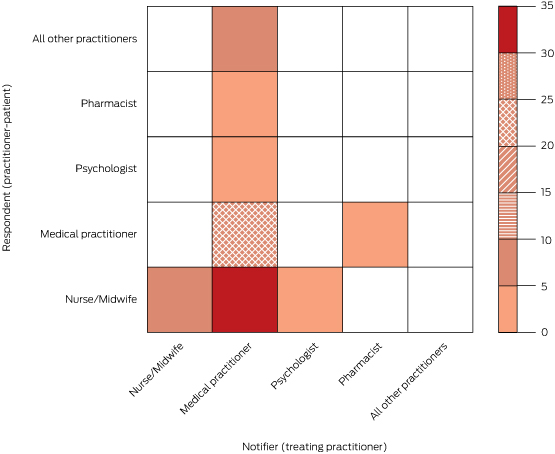
A large majority of the reporters (57 of 64) were doctors, and most of the practitioner-patients were nurses (41 of 64) (Box 1). Two-thirds of the reports by doctors were made by psychiatrists (26 of 57) or general practitioners (16 of 57).
The most common dyads were doctors reporting nurse-patients (35 of 64 cases) and doctors reporting doctor-patients (15 of 64 cases) (Box 2). Nurse reports about nurse-patients were relatively uncommon (5 of 64 cases), although every nurse report involved a nurse-patient.
Grounds for report
Three-quarters of the reports (47 of 64) indicated that the practitioner-patient had placed the public at risk of substantial harm because of an impairment (Box 3). One-fifth of the reports (14 of 64) indicated that the practitioner had practised while intoxicated. Only three reports were triggered by departures from professional standards or sexual misconduct.
Health condition being treated
Practitioner-patients were primarily being treated for mental illnesses (28 of 64), substance misuse disorders (25 of 64) or neurological conditions (9 of 64) (Box 3). The most common forms of mental illness were psychosis, mania and depression. The most commonly misused substances were opiates, benzodiazepines, alcohol and amphetamines.
Nature of treatment relationship
The reporter for one in five reports (14 of 64) was the patient’s regular care provider (Box 4); the others involved treatment encounters with a non-regular care provider. The most common scenario was that the reporter had assumed the role of treating practitioner in the context of an acute presentation to hospital (38 of 64 cases), usually a psychiatric admission (27 of 38 cases). The other scenarios were that the reporter was seeing the patient for the first time (9 of 64 cases) or that the treatment relationship had been established indirectly through an informal corridor consultation (3 of 64 cases).
Other aspects of reports
In most reports (46 of 64 cases), the reporter mentioned discussing the mandatory notification requirement with the patient before the report was lodged. Most reporters (56 of 64) also mentioned that they had sought advice from an indemnity insurer, lawyer, manager or professional peer before making the report.
Twenty-six of the 47 reports of impairment described a risk of harm to the public; 12 of these reports discussed only future risks, six discussed only past risks, and eight discussed both.
Nearly four in five reports (50 of 64) described an impediment to risk reduction. There were four main types of impediment. The most commonly described was that the practitioner-patient lacked insight into the risks posed to patients by conditions such as mania, psychosis, or dementia (29 of 50 cases). A second impediment was deliberate dishonesty with the treating practitioner; this most commonly arose in cases where a practitioner-patient had an addiction and intentionally provided false information to the treating practitioner in an attempt to obtain drugs of misuse (12 of 50 cases). A third impediment was deliberate disregard for treatment advice or patient safety (5 of 50 cases); for example, when a practitioner would not adhere to prescribed medicines or comply with a plan intended to protect patients during the recovery of the treated practitioner. The final impediment to safe management was an ongoing intention to self-harm with medicines that could be obtained in clinical practice (4 of 50 cases).
The 14 reports that did not describe impediments to risk reduction either contained statements indicating that the practitioner-patient had insight into their health condition and was cooperating with treatment (two of these patients had already notified themselves to AHPRA), or there was no relevant information that enabled coding of this variable.
Reponses of reports
By November 2014, National Boards had made a final decision on 86% of the treating practitioner reports (55 of 64). Boards took immediate action in 19 cases. Immediate action is a formal measure that involves placing interim restrictions on practice; it is imposed when this is considered necessary to protect the public pending further investigation.
The final outcomes were: no further regulatory action by a Board (24 of 55 cases); voluntary agreements with the Board and AHPRA regarding appropriate monitoring, treatment or practice restrictions (16 of 54); imposition of formal conditions on the practitioner’s licence (12 of 55); a fine or formal reprimand (2 of 55); and referral to another body for resolution (1 of 55). Although the most common adjudication was to take no further action, it would be erroneous to infer that reports with this outcome were inappropriate or unfounded; steps may have been taken to redress a legitimate concern after the report had been lodged and before the Board’s final decision.
Discussion
Our study of mandatory reports of notifiable conduct by treating practitioners found that 90% were made by doctors, usually psychiatrists or general practitioners, and were typically related to a practitioner-patient who was experiencing mental illness, substance misuse problems or a neurological condition. Relatively few reports were made by regular care providers. Most reports were linked with situations in which the treating practitioner was struggling to safely manage the risk that the practitioner-patient posed, and reporters usually discussed the report with the patient before submitting it.
Australia’s requirement that treating practitioners notify regulators of practitioner-patients with impairments is not unprecedented. New Zealand has required health practitioners to report impaired peers since 2003,10 and several American states have mandatory reporting obligations that extend to treating practitioners.11 However, the Australian legislation is unusually far-reaching in two respects. First, it imposes a duty to report not only health impairments, but also certain concerns about performance. Second, it does not explicitly shield treating practitioners from the obligation to report if the practitioner-patient is participating in an approved program of treatment.
Opponents of mandatory reporting argued that the new requirements would open the floodgates to over-reporting.2 This has not occurred. Mandatory reports are rare events,2 and mandatory reports by treating practitioners are especially infrequent — so infrequent, in fact, that under-reporting is probably a more justifiable concern.
The prevalence of impairment in the health workforce is unknown, but conservative estimates suggest that at least 1000 doctors (about 1% of Australia’s 90 000 registered medical practitioners) are impaired in their ability to practise at some stage in the course of any given year.12-14 Our 15-month sample contained reports on only 16 doctors, and only 20% of the reports were made by the practitioner-patient’s usual care provider. Previous research in the United States and New Zealand suggests that under-reporting of impaired colleagues is widespread,15 even in the context of mandatory reporting laws. Barriers are likely to include loyalty to colleagues, concerns about over-reacting to a situation, and uncertainty about the reporting obligation.16-18
A second objection to the extension of mandatory reporting into the patient–doctor relationship is that it breaches a cornerstone of medical ethics: patient confidentiality. However, the duty to maintain patient confidentiality is not absolute. It is widely accepted that it should yield to obligations to report serious problems or risks that come to light during treatment, including certain infectious diseases, health conditions that imperil driving, and signs of child abuse.19 Whether impairments that pose risks to safe clinical practice are so different from these accepted forms of reporting is debatable. Addressing this issue is beyond the scope of our study, but several aspects of our findings should inform the debate. In particular, the infrequency of treating practitioner reports and the perceived seriousness of the impairments disclosed make it difficult to distinguish the risks associated with practitioner-patient impairment from those of other accepted categories of mandatory reporting by treating practitioners.
Perhaps the most serious charge levelled at the mandatory reporting of practitioner-patients is that it will discourage medical practitioners from seeking assistance.5 This objection involves an empirical question: do the harms that result from treatment foregone because of the law exceed the harms averted by identifying impaired practitioners who would not otherwise have been recognised? Such counterfactuals are difficult to assess. Anecdotal reports suggest that the Doctors' Health Advisory Services in some states experienced a decline in referrals after the law was enacted.6 But it is not clear whether there was a net decrease across all relevant health services; the question of causality is even less certain. Further, the deferred treatment argument presumes that impaired practitioners would still seek care in the absence of the possibility that they might be reported, but the available evidence suggests that health practitioners may have been reluctant to do so even before the introduction of the law.17,20
When discussing concerns about seeking help, it is worth noting how the reporting behaviour by treating practitioners observed in our study deviated from the exact requirements of the law. The statutory duty to report refers to a past risk of harm and, unlike mandatory reporting programs elsewhere, there is no safe harbour for cases where a practitioner-patient subsequently seeks care and takes appropriate steps to protect patient safety. The pattern of reporting we observed did not correspond with these legal requirements. When explaining their decision to report, treating practitioners were more likely to refer to a future risk of harm than to a past risk. Further, treating practitioners frequently emphasised factors that reduced their ability to work with the practitioner-patient to mutually manage the risk to the public (eg, the patient’s lack of insight, dishonesty or recklessness). Caution is required when making inferences about notifiable conduct that was not reported on the basis of what was reported, but these aspects of the reports, coupled with the very low overall rate of reporting, clearly suggest that treating practitioners resisted reporting their practitioner-patients in circumstances where their treatment was on an appropriate and promising path.
Our study has three main limitations. First, we were unable to directly measure over- and under-reporting. Second, Australia’s mandatory reporting law was implemented in concert with a variety of other major changes to health practitioner regulation, so it was not feasible to assess changes in the rate or nature of treating practitioner reports before and after the introduction of the new law. Finally, we relied on information provided in the reports for most of the variables of interest. To save time or protect confidentiality, some treating practitioners may have omitted or altered salient details. Consequently, the counts we report, particularly for variables that relied on being mentioned in the reports, should be interpreted as lower bound estimates.
Much of the policy debate on the merits of mandatory reporting by treating practitioners has been based on certain implicit assumptions. The standard narrative involves an impaired patient who recognises their illness and seeks treatment from their usual care provider, who must then reluctantly take the contentious step of reporting their patient. Our findings suggest a different picture. The debate should acknowledge several realities. In particular: treating practitioner reports are rare, very few are made in the context of an established treatment relationship, and they tend to occur in situations where there is an identified impediment to safely managing a future risk of harm within the confines of the treating relationship.
Box 1 – Characteristics of treating practitioners and practitioner-patients involved in mandatory reports
Practitioner making the notification (treating practitioner) |
Practitioner subject to the notification (practitioner-patient) |
||||||||||||||
Total number |
64 |
64 |
|||||||||||||
Profession |
|||||||||||||||
Medical practitioner |
57 |
16 |
|||||||||||||
Nurse |
5 |
41 |
|||||||||||||
Pharmacist |
1 |
2 |
|||||||||||||
Psychologist |
1 |
1 |
|||||||||||||
Other* |
0 |
4 |
|||||||||||||
Status |
|||||||||||||||
Practitioner |
64 |
59 |
|||||||||||||
Student |
0 |
5 |
|||||||||||||
Sex |
|||||||||||||||
Male |
40 |
20 |
|||||||||||||
Female |
23 |
44 |
|||||||||||||
Data missing |
1 |
0 |
|||||||||||||
Mean age (range), years |
46 (24–62) |
41 (20–81) |
|||||||||||||
* Dentist, physiotherapist, medical radiation practitioner. | |||||||||||||||
Box 2 – Frequency of notifications, by professions of treating practitioner and practitioner-patient
Box 3 – Statutory grounds for reporting, and health conditions mentioned, for 64 mandatory reports by treating practitioners
Statutory grounds for report |
Number of reports |
||||||||||||||
Have an impairment |
47 |
||||||||||||||
Practised while intoxicated |
14 |
||||||||||||||
Departure from professional standards |
2 |
||||||||||||||
Sexual misconduct |
1 |
||||||||||||||
Health condition being treated |
|||||||||||||||
Mental illness |
28 |
||||||||||||||
Psychosis/mania |
16 |
||||||||||||||
Depression/attempted suicide |
10 |
||||||||||||||
Eating disorder |
1 |
||||||||||||||
Obsessive–compulsive disorder |
1 |
||||||||||||||
Substance misuse |
25 |
||||||||||||||
Opiates |
8 |
||||||||||||||
Benzodiazepines |
6 |
||||||||||||||
Alcohol |
5 |
||||||||||||||
Amphetamines |
5 |
||||||||||||||
Other (cannabis, cocaine or LSD) |
3 |
||||||||||||||
Neurological condition |
9 |
||||||||||||||
Dementia/cognitive impairment |
7 |
||||||||||||||
Seizures |
2 |
||||||||||||||
Unclear |
2 |
||||||||||||||
Box 4 – Relationship between treating practitioner and the practitioner-patient for 64 mandatory reports by treating practitioners
Treating relationship of reporting practitioner to practitioner-patient |
Number of reports |
||||||||||||||
Regular care provider |
14 |
||||||||||||||
General practice |
9 |
||||||||||||||
Psychiatry practice |
4 |
||||||||||||||
Infectious disease practice |
1 |
||||||||||||||
Non-regular care provider |
50 |
||||||||||||||
Acute care provider |
38 |
||||||||||||||
Psychiatric admission |
27 |
||||||||||||||
General medical admission |
2 |
||||||||||||||
Emergency department admission |
9 |
||||||||||||||
First assessment |
8 |
||||||||||||||
Psychiatrist |
4 |
||||||||||||||
Physician |
3 |
||||||||||||||
Pharmacist |
1 |
||||||||||||||
Psychologist |
1 |
||||||||||||||
Informal consultation with colleague |
3 |
||||||||||||||
Received 22 June 2015, accepted 7 October 2015
- Marie M Bismark1
- Matthew J Spittal1
- Jennifer M Morris1
- David M Studdert2
- 1 Centre for Health Policy, University of Melbourne, Melbourne, VIC
- 2 Center for Health Policy, Freeman Spogli Institute for International Studies, Stanford Medical School, Stanford, Calif, USA
Marie Bismark was the recipient of a Fellows Career Development Fellowship from the Royal Australian College of Physicians for her study of mandatory reporting.
Marie Bismark and David Studdert are lead investigators on a National Health and Medical Research Council Partnership Grant with AHPRA. Jen Morris is a member of the AHPRA community reference group.
- 1. Health Practitioner Regulation National Law (Victoria) Act 2009. Melbourne: Parliament of Victoria, 2009. http://www.legislation.vic.gov.au/Domino/Web_Notes/LDMS/PubStatbook.nsf/f932b66241ecf1b7ca256e92000e23be/02566FDB9453A0CECA25768600149A94/$FILE/09-079a.pdf (accessed Jun 2015).
- 2. Bismark MM, Spittal MJ, Plueckhahn TM, Studdert DM. Mandatory reports of concerns about the health, performance and conduct of health practitioners. Med J Aust 2014; 201: 399-403. <MJA full text>
- 3. Australian Health Practitioner Regulation Agency. National Board guidelines for registered health practitioners: guidelines for mandatory notifications. Melbourne: Australian Health Practitioner Regulation Agency, 2014. http://www.medicalboard.gov.au/documents/default.aspx?record=WD14%2f13326&dbid=AP&chksum=6PgV3lDTI0fwe%2bSb0D342g%3d%3d (accessed Jun 2015).
- 4. Breen KJ. National registration legislative proposals need more work and more time. Med J Aust 2009; 191: 464-465. <MJA full text>
- 5. Goiran N, Kay M, Nash L, Haysom G. Mandatory reporting of health professionals: the case for a Western Australian style exemption for all Australian practitioners. J Law Med 2014; 22: 209-220.
- 6. Australian Medical Association Queensland. A step in the right direction on mandatory reporting [media release]. 12 Nov 2010. http://www.amaq.com.au/gdesign/9351_on/Stepintherightdirection.pdf (accessed Jun 2015).
- 7. Brettingham-Moore C. Mandatory reporting laws to be reviewed. Medical Observer [internet] 2010; 5 Nov. http://www.medicalobserver.com.au/news/mandatory-reporting-laws-to-be-reviewed (accessed Jun 2015).
- 8. Parker M. Embracing the new professionalism: self-regulation, mandatory reporting and their discontents. J Law Med 2011; 18: 456-466.
- 9. Corbin JM, Strauss AL. Basics of qualitative research: techniques and procedures for developing grounded theory. 4th ed. Los Angeles: SAGE, 2013.
- 10. Health Practitioners Competence Assurance Act 2003. Wellington: Government of New Zealand, 2003. http://www.legislation.govt.nz/act/public/2003/0048/latest/DLM203312.html. (accessed Jun 2015).
- 11. Brown RL, Schneidman BS. Physicians’ health programs: what’s happening in the USA? Med J Aust 2004; 181: 390-391. <MJA full text>
- 12. Leape LL, Fromson JA. Problem doctors: is there a system-level solution? Ann Intern Med 2006; 144: 107-115.
- 13. beyondblue. National mental health survey of doctors and medical students. Melbourne: beyondblue, 2013. https://www.beyondblue.org.au/docs/default-source/research-project-files/bl1132-report---nmhdmss-full-report_web.pdf?sfvrsn=4 (accessed Jun 2015).
- 14. McCall SV. Chemically dependent health professionals. West J Med 2001; 174: 50.
- 15. DesRoches CM, Rao SR, Fromson JA, et al. Physicians’ perceptions, preparedness for reporting, and experiences related to impaired and incompetent colleagues. JAMA 2010; 304: 187-193.
- 16. Raniga S, Hider P, Spriggs D, Ardagh M. Attitudes of hospital medical practitioners to the mandatory reporting of professional misconduct. N Z Med J 2005; 118: U1781.
- 17. Baldisseri MR. Impaired healthcare professional. Crit Care Med 2007; 35: S106-S116.
- 18. Council on Ethical and Judicial Affairs. Reporting impaired, incompetent or unethical colleagues. J Miss St Med Assoc 1992; 33: 176-177. https://www.ama-assn.org/ssl3/ecomm/PolicyFinderForm.pl?site=www.ama-assn.org&uri=%2fresources%2fhtml%2fPolicyFinder%2fpolicyfiles%2fHnE%2fE-9.031.HTM (accessed Jun 2015).
- 19. Mathews B, Kenny MC. Mandatory reporting legislation in the United States, Canada, and Australia: a cross-jurisdictional review of key features, differences, and issues. Child Maltreat 2008; 13: 50-63.
- 20. Wallace JE, Lemaire JB, Ghali WA. Physician wellness: a missing quality indicator. Lancet 2009; 374: 1714-1721.
Eleanor Dawson
Competing Interests: No relevant disclosures
Dr Eleanor Dawson
Retired solo private psychaitrist - Independent research re regulation of the profession