




Lucille is a 2.5-year-old who has had a cold for 3 days. Last night, it became worse — Lucille was restless and had a fever. Her mother was up with her for much of the night, and she settled eventually with paracetamol. The mother and Lucille come to see you today and both look exhausted. The only positive findings on clinical examination are a congested nose and bulging red left ear drum. You diagnose acute otitis media. “OK”, you say, “Lucille has a middle ear infection”. Her mother asks, “What can be done to help her?”
Shared decision making is a consultation process where a clinician and patient jointly participate in making a health decision, having discussed the options and their benefits and harms, and having considered the patient's values, preferences and circumstances. Shared decision making is not a single step to be added into a consultation, but can provide a framework for communicating with patients about health care choices to help improve conversation quality. It is a process that can be used to guide decisions about screening, tests and treatments. It can also be thought of as a mechanism for applying evidence with an individual patient through personalising the clinical decision. Although, to date, most research about shared decision making has focused on medical practitioners, it is relevant to clinicians of all disciplines, including nursing and allied health.1
Shared decision making can be viewed as a continuum,2 along which the extent to which a patient or a clinician takes responsibility for the decision-making processes varies. At the extremes are clinician-led decisions and patient-led decisions, with many other possible approaches in between.2,3 The extent of involvement will vary between individuals and between consultations, and according to the patient's preferences and the context in which the decision is occurring. Regardless of whether the patient or clinician takes the lead in the decision-making process, joint discussion should occur.
How can shared decision making help?
Internationally, shared decision making is seen as a hallmark of good clinical practice, an ethical imperative,4 and as a way of enhancing patient engagement and activation. Increasingly, it is being advocated for in clinical guidelines and health care policies.5-7 While shared decision making is applicable to most situations, it is especially important in certain circumstances; for example, where the evidence does not strongly support a single clearly superior option (most clinical decisions) or where a preference-sensitive decision is involved. That is, when there is uncertainty as to which option is superior, each option has different inherent benefits and harms, or the decision is likely to be strongly influenced by patients' preferences and values.8,9
The relationship between shared decision making and evidence-based practice is becoming increasingly recognised. Shared decision making provides a process for bringing evidence into the consultation and incorporating it into discussions with the patient, along with discussion about the patient's values and preferences. In other words, it is an important, if under-recognised, component to evidence translation, a route by which evidence is incorporated into clinical practice. Shared decision making may also help reduce the unwarranted variation in care10 that may partially arise from clinicians' opinions dominating decision making, with insufficient consideration of both empirical evidence and patients' preferences.11
Patients and clinicians typically overestimate the benefits of interventions and underestimate their harms.12-14 Shared decision making can provide the opportunity for resolving this mismatch between clinician and patient expectations and the demonstrated benefits and harms of screening, tests and interventions. Consequently, shared decision making may reduce the inappropriate use of tests and treatments,15 such as those that are not beneficial for the majority or are associated with substantial risks or harms. As such, it can play a role in reducing the problem of overdiagnosis and overtreatment. Patients tend to choose more conservative options than their clinicians when fully informed about the benefits and harms.15
Most evidence about the effectiveness of shared decision making comes from trials of decision aids, where most research has been conducted to date. Decision aids have demonstrated effectiveness for increasing knowledge and risk-perception accuracy; improving patient–clinician communication; and reducing decisional conflict, feeling uninformed, passivity in decision making, and indecision about the choices made.15
The process of shared decision making
A common misperception is that shared decision making is synonymous with the use of decision aids. However, the core of shared decision making is a process, which might additionally use decision support tools but is not dependent on them. This process varies according to numerous factors related to the patient, clinician and other circumstances. One set of questions that can be used to guide the process is shown in Box 1. Originally phrased for use by patients,16 we have amended the wording to the clinicians' perspective.
As many patients are unfamiliar with being invited to share in decision making, it may help to briefly explain the process. Outlining that they have some choices that you would like to go through with them before deciding together about the next step may reassure patients who might otherwise feel overwhelmed, uncertain or even abandoned. If the problem or diagnosis is clear, and a decision about the next step is necessary, the next step involves describing the nature of the problem or condition (question 1, Box 1). This should usually include providing information about the natural history of the condition — that is, what is likely to happen without any intervention (“watch and wait”). Eliciting the patient's expectations about management of the condition, including previously tried approaches and experiences, along with fears and concerns, is important and allows for discussion and correction of misperceptions where necessary (either at this stage or later in the process). The second question triggers a discussion of the options and identification of those that the patient would like to hear more about (Box 1). The third question enables discussion about the benefits and harms of each option, including their likely probability or size (Box 1 and Box 2). The fourth question provides patients the opportunity to weigh up the benefits and harms of the options, and consider them in the context of their preferences, values and circumstances (Box 1). Finally, the fifth question explores whether the patient is ready to make a decision or whether further information, time or involvement of other people is needed before a choice can be made (Box 1). If a high-quality and appropriate decision support tool is available for the decision under consideration, it can be incorporated before, during or after the consultation.
There are other approaches to shared decision making, in addition to the approach shown in Box 1. One alternative model breaks the decision-making part of the consultation into choice talk (helping patients to know that options exist), option talk (discussing the options and their benefits and harms) and decision talk (helping patients explore options and make decisions).19
The role of decision support tools in shared decision making
Evidence summaries can be useful in supporting decision making, but current formats such as clinical practice guidelines and systematic reviews typically do not map well onto decision points in the consultation, nor do they promote patient interaction and discussion. This is particularly so where the evidence is uncertain or where benefits and harms need to be weighed up with patient preferences and clinical contexts to individualise decisions.
Specifically developed decision support tools can help clinicians and patients to draw on available evidence when making clinical decisions.20 The tools take a number of formats (Box 3). Some are explicitly designed to facilitate shared decision making (eg, decision aids). Others provide some of the information needed for some components of the shared decision-making process (eg, risk calculators, evidence summaries), or provide ways of initiating and structuring conversations about health decisions (eg, communication frameworks, question prompt lists).
When appropriate tools do exist, clinicians can use them in various ways: during the consultation (Box 1); as homework tools (where the patient is invited to use them either in the waiting room or at home, before or after the consultation); and either with or without assistance.
Decision support tool use is not always straightforward. They may not fit the patient's clinical or personal circumstances; clinicians and patients need to be willing to use them; they require clinicians to have some skills in how to use them; and there may need to be support for their use and delivery. Decision support tools alone are not the answer, and providing them does not guarantee that shared decision making will occur. Knowledge exchange alone is not sufficient — shared decision making needs to occur in a context where patients are enabled and supported to have a more active role.21,22
Misconceptions about shared decision making
Shared decision making is making headway in many countries.23 However, a number of misconceptions are hampering its implementation. Box 4 lists the barriers to shared decision making, as perceived by clinicians,24 along with comments and, where possible, research findings about each perceived barrier.
Challenges to shared decision making
There are several key challenges to the widespread use of shared decision making within the Australian health care system. First, training in shared decision-making skills is essential for its uptake, yet unlike various international initiatives,40 limited training options exist in Australia for both student clinicians and practicing clinicians. Second, shared decision making is dependent on clinicians having access to up-to-date high-quality evidence, preferably already synthesised. Decision support tools can assist with this, but they exist for only a minority of health care decisions, are of varying quality, are scattered across multiple sources and are difficult to find, and ones developed internationally may not be readily applicable to the Australian context or vulnerable populations. Third, shared decision making is hampered for clinical questions where quality evidence does not exist or has not yet been synthesised. Finally, shared decision making in the area of Indigenous health and vulnerable populations (such as patients with poor health literacy) is important but presents additional challenges, and there is less research to guide implementation in these areas.36
Australia is drastically lagging behind many other countries in all aspects of shared decision making — policies, lobbying, advocacy, research funding, training, resources and implementation.41,42 In the absence of a coordinated national effort, we encourage individual clinicians to begin incorporating shared decision making into their consultations with patients when a health decision is needed. Australia's health training and delivery organisations need urgently to begin prioritising and planning to make shared decision making a reality in Australia.
1 An example of one approach to shared decision making
Five questions that clinicians can use to guide shared decision making16 | Example phrases (for the opening clinical scenario of a child with acute otitis media) | Comments | |||||||||||||
1. What will happen if we wait and watch? | “In children, most middle ear infections get better by themselves, usually within a week. The best options to control pain and fever are paracetamol or ibuprofen.” | Quantitative information can be provided where possible, either at this step or in step 3 where each option is described. When this is not possible, descriptive information can be provided (eg, “most people find that the symptoms go away by ...”). Eliciting patient's expectations about management of the condition (eg, “what have you heard or do know about …?”), including previously tested approaches and experiences, along with fears and concerns, is important and may occur here or later in the process. | |||||||||||||
2. What are your test or treatment options? | “Waiting for it to get better by itself is one option. Another option is to take antibiotics. Do you want to discuss that option?” | For some decisions (such as in this example), the options may be familiar to patients and need little elaboration at this step. In others, a more detailed explanation of each option and its practicalities, including options which are time-urgent, will be required. | |||||||||||||
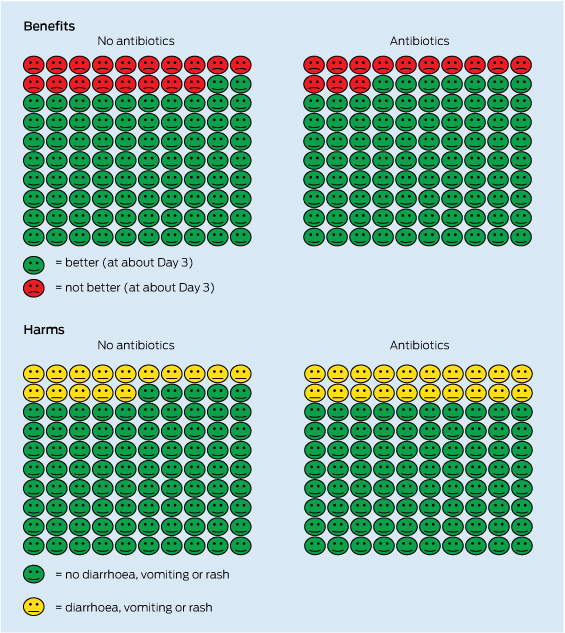
3. What are the benefits and harms of these options? | “We know from good research that of 100 children with middle ear infection who do not take antibiotics, 82 will feel better and have no pain after 2–3 days. Out of 100 children who do take antibiotics, 87 will feel better after about 3 days of taking them. So, about five more will get better a little faster. We can't know whether your child will be one of the five children who benefit or not.” (A graphic representation of these numbers can also be shown at this point, and again after the harms information is discussed [Box 2].) “There are some downsides to antibiotics though. Out of 100 children who do take antibiotics, 20 will experience vomiting, diarrhoea or rash, compared with 15 who do not take them. That means about five children out of 100 will have side effects from antibiotics. But again, we can't know whether your child will have any of these problems. The other possible downside is antibiotic resistance — would you like to hear more about it?” (The option of delayed prescribing could also be discussed here. Numbers used in this scenario are from Venekamp et al.17) | In addition to descriptively discussing the benefits and harms of each option, the probability of each occurring, where this is known, should be provided. For dichotomous outcomes (eg, having a myocardial infarction), this should be in the form of natural frequencies (ie, the number out of 100 or 1000 people who experience the event) rather than relative risk. For continuous outcomes (eg, number of days of pain, and level of anxiety as reported on an anxiety measure), this may be expressed by the estimated size of the effect (eg, the average reduction in 20 points on anxiety on a tool that measured it as a score from 0 to 100). Decision support tools, if available, can be useful at this stage. Simple visual graphics can be particularly useful in helping to communicate the numbers. Principles of effectively communicating statistical information to patients should be followed, such as using natural frequencies (ie, x out of 100), being aware of framing effects, and using multiple formats.18 The discussion of harms should extend beyond the risk of side effects and include other impacts that the option could have on the patient, such as cost, inconvenience and interference with daily roles, and reduced quality of life. | |||||||||||||
4. How do the benefits and harms weigh up for you? | “With all I've said, which option do you feel most comfortable with?” | This step includes eliciting patients' preferences and working with them to clarify how each option may fit with their values, preferences, beliefs and goals. Some decision aids include formal value clarification exercises that may be used to supplement the conversation and/or enable the patient to reflect further following the consultation. Clarifying the patient's understanding of what has been discussed so far, using the teach-back method, can help to identify if any information needs to be repeated or explained in another way. | |||||||||||||
5. Do you have enough information to make a choice? | “Is there any more you want to know? Do you feel you have enough information to make a choice?” | This provides another opportunity to ask if the patient has additional questions. Patients may feel ready to make a decision at this stage or it may be jointly decided to defer the decision and plan when it should be revisited. The patient may wish to seek further information before deciding, discuss with family, or take time to process and reflect on the information received. | |||||||||||||
3 Examples of types of decision support tools to facilitate shared decision making
Type of tool | Brief description | Examples | |||||||||||||
Condition-specific | |||||||||||||||
Decision aids | Describe the options, and the benefits and harms of each option, along with a values clarification exercise and sometimes a guide to decision making. The International Patient Decision Aid Standards Collaboration (http://www.ipdas.ohri.ca) provides information about assessing the quality of decision aids | Ottawa Hospital Research Institute A to Z Inventory of Decision Aids: : http://decisionaid.ohri.ca/AZinvent.php | |||||||||||||
Decision or fact boxes | A short summary of the benefits and harms of an intervention, often presented in two columns | Dartmouth Medicine drug facts box: http://dartmed.dartmouth.edu/spring08/html/disc_drugs_we.php; | |||||||||||||
Option grids | A one-page summary of the evidence for the possible options, addressing patient-centred outcomes, and questions and concerns frequently raised by patients; can be useful within the consultation for a patient to highlight what is important to them | Option Grid Collaborative: | |||||||||||||
Question prompt lists | A predefined list of condition-specific questions for patients to consider using in a consultation | Cancer Institute NSW: | |||||||||||||
Evidence summaries | Clinical practice guidelines and other summaries of the body of evidence | Clinical Evidence: http://www.clinicalevidence.bmj.com; UpToDate: | |||||||||||||
Generic | |||||||||||||||
Communication frameworks | A generic set of questions or scripts and a structure for clinicians and patients to use during decision making | Ask Share Know: http://www.askshareknow.com.au; Ottawa Personal Decision Guide: | |||||||||||||
4 Misconceptions about shared decision making and key research findings that refute them
Misconception | Research findings | ||||||||||||||
The duration of the consultation will be lengthened | |||||||||||||||
This concern is the most frequently reported barrier to shared decision making. Indeed, time constraint is the most frequently reported barrier to any clinical change.25 | Three systematic reviews (on interventions to implement shared decision making, and impact of decision aids on processes of care and patient outcomes) indicate that there is no systematic increase in consultation duration when shared decision making is implemented or decision aids are used.15,26,27 | ||||||||||||||
Patients will be unsupported when making health care decisions | |||||||||||||||
There is a fear that shared decision making will make patients feel abandoned during difficult decisions. | This is a misinterpretation of the intent of shared decision making. The definition of shared decision making explicitly describes patients and their clinicians sharing the decision together.3 Shared decision making is not about insisting that every patient make the decision (not all patients wish to); rather it helps to ensure that patients are informed about their options and are offered the opportunity to participate in the process. | ||||||||||||||
Not every patient wants to share in the decision-making process with their clinician | |||||||||||||||
Critics of shared decision making argue that not every patient wants to be involved in making decisions with their clinician. | An Australian survey reported that > 90% of women preferred a shared role with their doctor in making decisions about screening and diagnostic tests.28 A European survey of > 8000 people reported a high desire for shared health decision making (> 70% of the sample).29 A systematic review of 14 studies that examined the match between patient preferences about information and decision making with clinician–patient communication found that a substantial number of patients (26%–95%; median, 52%) were dissatisfied with the information given and would have preferred a more active role in decisions concerning their health, especially when they understood the expectations attached to this role.30 A time trend in desired involvement in decision making has also been reported. Of the studies conducted in 2000 and later, 71% reported that most respondents preferred a role in sharing decisions, compared to 50% of studies that were conducted before 2000.31 | ||||||||||||||
Most people are not able to participate in shared decision making | |||||||||||||||
Critics of shared decision making question its complexity, believing most people will not be able to manage it. | Shared decision making is comprised of a set of behaviours on the part of the clinician and the patient that can be learnt.32,33 An increasing number of studies have demonstrated that shared decision making can be implemented successfully in clinical practice.27,34 | ||||||||||||||
Shared decision making cannot be used with vulnerable people | |||||||||||||||
Shared decision making requires a special set of skills that may be too complex for all patients to acquire, and vulnerable people may not ever be able to share decisions with their clinicians. | Most surveys of patients' willingness to engage in shared decision making show that the most vulnerable people are less willing to participate.30 Therefore, we need to be careful not to increase health inequities by offering shared decision making solely to the most privileged patients. Individuals with low health literacy want to be involved in health decisions but often lack the knowledge, skills and confidence to communicate with clinicians, navigate the health system and engage in shared decision making.35 They receive less information, ask fewer questions and are less satisfied with health care provider communication.36 More vulnerable patients may be less likely to engage in shared decision making because of lower self-efficacy — a modifiable factor to increase their willingness to do so.34 Indeed, in order to decrease health inequities, more needs to be done to engage the most vulnerable patients to make informed decisions.36,37 | ||||||||||||||
“I already do this” | |||||||||||||||
Most clinicians feel that they already successfully engage their patients in shared decision making — a belief that may arise from not really understanding what it is and how to do it. | A systematic review of 33 studies that assessed shared decision making using the OPTION (Observing Patient Involvement in Decision Making) scale found low levels of patient-involving behaviours. In studies where no intervention was used to facilitate shared decision making, the mean OPTION score was 23 14 (0–100 scale, where higher scores indicate higher levels of patient involvement in decision making).21 Lack of familiarity with shared decision making by clinicians has been found to be a barrier to shared decision making in a number of studies.38 | ||||||||||||||
Engaging patients in shared decision making will raise their anxiety level | |||||||||||||||
Some clinicians are afraid that shared decision making will raise patients' anxiety levels as they become aware of the inherent uncertainty of evidence. | A Cochrane review of decision aids refutes this misconception, finding no effect on anxiety.15 Anxiety should not be confused with decisional conflict, an intrapsychological construct that reflects the difficulty that individuals can experience when comparing the pros and cons of different options.39 | ||||||||||||||
Provenance: Not commissioned; externally peer reviewed.
- Tammy C Hoffmann1,2
- France Légaré3
- Magenta B Simmons4
- Kevin McNamara5,6
- Kirsten McCaffery7
- Lyndal J Trevena7
- Ben Hudson8
- Paul P Glasziou1
- Christopher B Del Mar1
- 1 Centre for Research in Evidence-Based Practice, Bond University, Gold Coast, QLD.
- 2 School of Health and Rehabilitation Sciences, University of Queensland, Brisbane, QLD.
- 3 Centre Hospitalier Universitaire de Québec, Quebec, Canada.
- 4 Orygen Youth Health Research Centre, Melbourne, VIC.
- 5 Greater Green Triangle University Department of Rural Health, Flinders University and Deakin University, Warrnambool, VIC.
- 6 Centre for Medicine Use and Safety, Monash University, Melbourne, VIC.
- 7 School of Public Health, University of Sydney, Sydney, NSW.
- 8 Department of Public Health and General Practice, University of Otago, Christchurch, New Zealand.
This article arose from discussions held at an inaugural national shared decision-making symposium in October 2013 on the Gold Coast, Australia. The symposium was sponsored by the Centre for Research in Evidence-Based Practice, the Australian Commission on Safety and Quality in Health Care (with particular thanks to Heather Buchan) and the National Health and Medical Research Council (NHMRC). Tammy Hoffmann is supported by NHMRC/Primary Health Care Research, Evaluation and Development Career Development Fellowship 1033038, with funding provided by the Australian Government Department of Health. Kirsten McCaffery is supported by NHMRC Career Development Fellowship 1029241. Paul Glasziou is supported by NHMRC Australia Fellowship 527500. Tammy Hoffmann, Paul Glasziou and Christopher Del Mar are chief investigators at the Centre for Research Excellence in Minimising Antibiotic Resistance from Acute Respiratory Infections, which is undertaking research in shared decision making (NHMRC grant 1044904).
No relevant disclosures.
- 1. Légaré F, Stacey D, Brière N, et al. Healthcare providers' intentions to engage in an interprofessional approach to shared decision-making in home care programs: a mixed methods study. J Interprof Care 2013; 27: 214-222.
- 2. Kon A. The shared decision-making continuum. JAMA 2010; 304: 903-904.
- 3. Charles C, Gafni A, Whelan T. Shared decision-making in the medical encounter: what does it mean? (or it takes at least two to tango). Soc Sci Med 1997; 44: 681-692.
- 4. Elwyn G, Tilburt J, Montori VM. The ethical imperative for shared decision-making. Eur J Pers Centered Healthc 2013; 1: 129-131. http://www.bjll.org/index.php/ejpch/article/download/645/686 (accessed Apr 2014).
- 5. 111th United States Congress. Patient Protection and Affordable Care Act. Public Law 111-148; 2010.
- 6. Australian Commission on Safety and Quality in Health Care. Australian Safety and Quality Framework for Health Care. Sydney: ACSQHC, 2010. http://www.safetyandquality.gov.au/national-priorities/australian-safety-and-quality-framework-for-health-care (accessed Jan 2014).
- 7. NHS England. Shared decision making. http://www.england.nhs.uk/ourwork/pe/sdm (accessed Dec 2013).
- 8. Elwyn G, Edwards A, Kinnersley P, Grol R. Shared decision making and the concept of equipoise: the competences of involving patients in healthcare choices. Br J Gen Pract 2000; 50: 892-899.
- 9. Müller-Engelmann M, Donner-Banzhoff N, Keller H, et al. When decisions should be shared: a study of social norms in medical decision making using a factorial survey approach. Med Decis Making 2013; 33: 37-47.
- 10. Mulley AG, Trimble C, Elwyn G. Stop the silent misdiagnosis : patients' preferences matter. BMJ 2012; 345: e6572.
- 11. Wennberg JE. Unwarranted variations in healthcare delivery: implications for academic medical centres. BMJ 2002; 325: 961-964.
- 12. Hoffmann TC, Del Mar CB. Naively optimistic? A systematic review of patients' expectation of benefits and harms of treatments, screening, and tests. Poster presented at: Society for Medical Decision Making Asia-Pacific Conference; 2014 Jan 6-8; Singapore. https://smdm.confex.com/smdm/apm2014/webprogram/Paper8033.html (accessed April 2014).
- 13. Hudson B, Zarifeh A, Young L, Wells JE. Patients' expectations of screening and preventive treatments. Ann Fam Med 2012; 10: 495-502.
- 14. Sapre N, Mann S, Elley CR. Doctors' perceptions of the prognostic benefit of statins in patients who have had myocardial infarction. Intern Med J 2009; 39: 277-282.
- 15. Stacey D, Légaré F, Col NF, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev 2014; (1): CD001431. doi: 10.1002/14651858.CD001431.pub4.
- 16. Irwig L, Irwig J, Trevana L, Sweet M. Smart health choices: making sense of health advice. London: Hammersmith Press, 2008.
- 17. Venekamp RP, Sanders S, Glasziou PP, et al. Antibiotics for acute otitis media in children. Cochrane Database Syst Rev 2013; (1): CD000219.
- 18. Hoffmann T, Tooth L. Talking with patients about evidence. In: Hoffmann T, Bennett S, Del Mar C, editors. Evidence-based practice across the health professions. 2nd ed. Sydney: Elsevier, 2013: 328-352.
- 19. Elwyn G, Frosch D, Thomson R, et al. Shared decision making: a model for clinical practice. J Gen Intern Med 2012; 27: 1361-1367.
- 20. Kastner M, Straus SE. Application of the Knowledge-to-Action and Medical Research Council frameworks in the development of an osteoporosis clinical decision support tool. J Clin Epidemiol 2012; 65: 1163-1170.
- 21. Couët N, Desroches S, Robitaille H, et al. Assessments of the extent to which health-care providers involve patients in decision making: a systematic review of studies using the OPTION instrument. Health Expect 2013; Mar 4 [Epub ahead of print]. doi: 10.1111/hex.12054.
- 22. Joseph-Williams N, Elwyn G, Edwards A. Knowledge is not power for patients: a systematic review and thematic synthesis of patient-reported barriers and facilitators to shared decision making. Patient Educ Couns 2014; 94: 291-309.
- 23. Härter M, van der Weijden T, Elwyn G. Policy and practice developments in the implementation of shared decision making: an international perspective. Z Evid Fortbild Qual Gesundhwes 2011; 105: 229-233.
- 24. Légaré F, Ratté S, Gravel K, Graham ID. Barriers and facilitators to implementing shared decision-making in clinical practice: update of a systematic review of health professionals' perceptions. Patient Educ Couns 2008; 73: 526-535.
- 25. Cabana MD, Rand CS, Powe NR, et al. Why don't physicians follow clinical practice guidelines? A framework for improvement. JAMA 1999; 282: 1458-1465.
- 26. Légaré F, Ratté S, Stacey D, et al. Interventions for improving the adoption of shared decision making by healthcare professionals. Cochrane Database Syst Rev 2010; (5): CD006732.
- 27. Légaré F, Turcotte S, Stacey D, et al. Patients' perceptions of sharing in decisions: a systematic review of interventions to enhance shared decision making in routine clinical practice. Patient 2012; 5: 1-19.
- 28. Davey HM, Barratt AL, Davey E, et al. Medical tests: women's reported and preferred decision-making roles and preferences for information on benefits, side-effects and false results. Health Expect 2002; 5: 330-340.
- 29. Coulter A, Jenkinson C. European patients' views on the responsiveness of health systems and healthcare providers. Eur J Public Health 2005; 15: 355-360.
- 30. Kiesler DJ, Auerbach SM. Optimal matches of patient preferences for information, decision-making and interpersonal behavior: evidence, models and interventions. Patient Educ Couns 2006; 61: 319-341.
- 31. Chewning B, Bylund CL, Shah B, et al. Patient preferences for shared decisions: a systematic review. Patient Educ Couns 2012; 86: 9-18.
- 32. Frosch DL, Légaré F, Fishbein M, Elwyn G. Adjuncts or adversaries to shared decision-making? Applying the Integrative Model of behaviour to the role and design of decision support interventions in healthcare interactions. Implement Sci 2009; 4: 73.
- 33. Hoffmann T, Bennett S, Tomsett C, Del Mar C. Brief training of student clinicians in shared decision making: a single-blind randomised controlled trial. J Gen Int Med 2014; 29: 844-849.
- 34. Légaré F, St-Jacques S, Gagnon S, et al. Prenatal screening for Down syndrome : a survey of willingness in women and family physicians to engage in shared decision-making. Prenat Diagn 2011; 31: 319-326.
- 35. Smith SK, Dixon A, Trevena L, et al. Exploring patient involvement in healthcare decision making across different education and functional health literacy groups. Soc Sci Med 2009; 69: 1805-1812.
- 36. McCaffery KJ, Holmes-Rovner M, Smith SK, et al. Addressing health literacy in patient decision aids. BMC Med Inform Decis Mak 2013; 13 Suppl 2: S10.
- 37. McCaffery KJ, Smith SK, Wolf M. The challenge of shared decision making among patients with lower literacy: a framework for research and development. Med Decis Making 2010; 30: 35-44.
- 38. Gravel K, Légaré F, Graham ID. Barriers and facilitators to implementing shared decision-making in clinical practice: a systematic review of health professionals' perceptions. Implement Sci 2006; 1: 16.
- 39. O'Connor AM. Validation of a decisional conflict scale. Med Decis Making 1995; 15: 25-30.
- 40. Légaré F, Politi MC, Drolet R, et al. Training health professionals in shared decision-making: an international environmental scan. Patient Educ Couns 2012; 88: 159-169.
- 41. McCaffery KJ, Smith S, Shepherd HL, et al. Shared decision making in Australia in 2011. Z Evid Fortbild Qual Gesundhwes 2011; 105: 234-239.
- 42. McCaffery K, Shepherd HL, Trevena L, et al. Shared decision-making in Australia. Z Arztl Fortbild Qualitatssich 2007; 101: 205-211.
Summary