




Newborn infants requiring retrieval for medical care have an increased risk of developing major neonatal complications and possibly long-term neurodevelopmental disabilities compared with those born in a centre that can immediately provide the required level of care.1-6 These increased risks could be ascribed to a difference in access to high-level obstetric care, expert resuscitation and immediate neonatal intensive care. Newborn retrieval separates the mother and infant at birth for a time and creates issues for families that can be difficult to quantify, including the inconvenience secondary to separation and financial pressures. Newborn retrieval is expensive, equivalent to between 1 and 4 days of intensive care, plus ambulance and aircraft costs (Andrew Berry, State Director of the New South Wales Newborn and Paediatric Emergency Transport Service [NETS], personal communication) with additional opportunity costs when teams are not available for other missions.
In Australia, the National Health and Medical Research Council (NHMRC) recommends that births of less than 33 weeks’ completed gestation take place in perinatal centres.7 The NSW Pregnancy and Newborn Services Network (PSN) was established in 1991 to oversee the planning, coordination and regionalisation of perinatal services. The benefits of such strategies have already been shown to reduce births in non-perinatal centres and improve clinical outcomes in extremely premature infants.8 However, whether such a benefit is observed in more mature babies (late preterm and term) is not reported.
In NSW, the roles of public hospitals are delineated according to resources and skills to provide different levels of maternity and newborn services (Appendix).9 There is no such role delineation for private hospitals. If a hospital operates outside its role delineation, it is more likely to need a retrieval service to transfer the newborn to an appropriate facility. Such neonatal retrievals might be avoided if pregnant women are initially transferred to an appropriate facility.
Elective caesarean section before 39 weeks of gestation is associated with increased respiratory morbidity in the newborn.10 In 2007, NSW Health issued a policy directive regarding the gestation at which elective caesarean section becomes safer in terms of reduced neonatal respiratory morbidity.11 Earlier discretionary caesarean has the potential to increase neonatal morbidity and newborn retrieval.
where there was knowledge and sufficient time to arrange safe IUT but this was not arranged;
discretionary caesarean — elective (pre-labour) caesarean section without documented fetal or maternal indications before 39 completed weeks of gestation;
elective induction (pre-labour) without documented fetal or maternal indications before 39 completed weeks of gestation; and
hospitals practising outside their role — hospitals planning births at lower gestational ages than that designated by their role delineation.
Each retrieval was reviewed by a retrieval consultant and neonatologist and assigned to a category based on consensus. The retrieval rates for each category of retrievals (potentially avoidable, unavoidable and unclassified) and for each level of the referring public hospital Appendix) and for private hospitals were calculated over the study period. The rates were adjusted for live births at each of the hospitals during the study period. Although there is no role delineation guide from NSW Health for private hospitals, they were classified based on their available resources and skills using similar classification to that used with public hospitals. Trends in potentially avoidable retrievals from each of the referring hospitals were reported for the study period. The distributions of the causes in potentially avoidable retrievals were described with the aim of identifying areas for improvement.
There were 2494 newborn retrievals over the study period with an annual average of 623 total retrievals and 30 potentially avoidable retrievals. There was an increase in the number of retrievals over the study period from 566 in 2006 to 699 in 2009. Box 1 shows the distribution of the retrievals for each category and the live birth rates over the study period. Total retrievals per 10 000 live births gradually increased over the study period from 62 in 2006 to 73 in 2009. Potentially avoidable retrievals per 10 000 live births reduced by half in the same time. Box 2 shows this information for each public hospital level and for private hospitals. Among public hospitals, use of the retrieval service decreased with increasing level of the hospital. Tertiary perinatal centres (level 5–6) rarely use retrieval services, with level 1–4 centres and private hospitals being the major users of retrieval for newborns. Rates of potentially avoidable retrievals ranged from none to nine per 10 000 live births across the different levels of the public and private hospitals.
Box 3 displays the potentially avoidable retrieval rates per 10 000 live births for each hospital level over the study period. There was a reduction in the potentially avoidable retrieval rates (per 10 000 live births) at all levels of public hospitals over the study period while those at the private hospitals have remained constant over time.
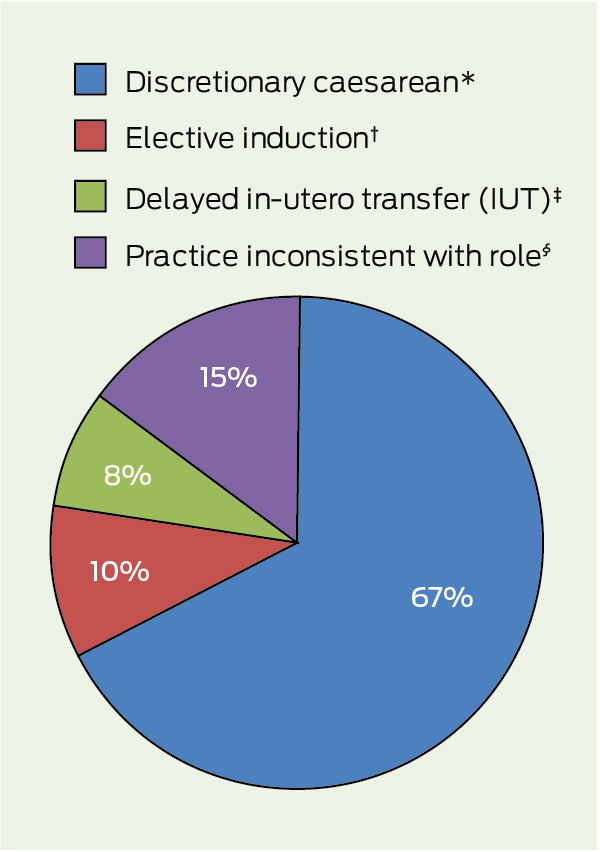
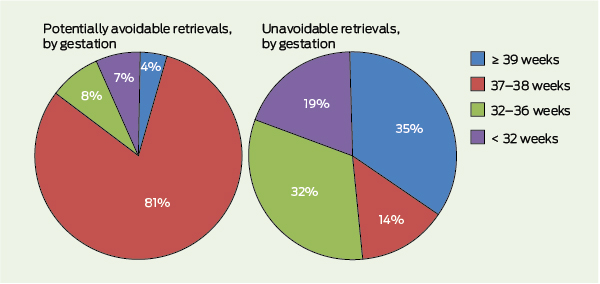
Discretionary caesarean accounts for two-thirds of the potentially avoidable retrievals (Box 4). The other factors leading to potentially avoidable retrievals were hospitals practising outside their role delineation (15%), elective induction (10%), and missed opportunity for IUT (8%). Near-term babies (37–38 weeks’ gestation) constitute most (81%) of the potentially avoidable retrievals, while preterm babies (less than 32 weeks’ gestation) contribute only 7% of the potentially avoidable retrievals (Box 5). In comparison, the distribution of gestation among the unavoidable retrievals was more even.
NSW NETS provides a statewide advisory and intensive care retrieval service for NSW Health. Some 245 hospitals in NSW and the Australian Capital Territory call on NETS for newborns, infants and children up to the age of 16 years. With decreasing numbers of non-tertiary live births of extremely preterm infants, it is vital to ensure the benefits of not requiring a retrieval are extended to the high-risk late-preterm and term population.8 The most difficult task was to define a priori a potentially avoidable retrieval. This was achieved by consensus and using NSW Health policies around role delineation of health services and timing of caesarean section.9,11
Discretionary caesarean accounted for two-thirds of the avoidable retrievals. Most of these babies required retrieval for need of respiratory support. The increased risk of respiratory morbidity in newborns born by elective caesarean section before 39 weeks of gestation has been repeatedly demonstrated.10,12,13 Our results are consistent with these studies and demonstrate the utility of retrieval services in managing those newborns. The United Kingdom National Institute for Health and Care Excellence guidelines and a NSW Health policy directive in 2007 state that elective or pre-labour caesarean section should not occur before 39 completed weeks of gestation in the absence of compelling medical indications.11,14 The reduction in the avoidable retrievals in the years 2008 and 2009 appears to result from implementation of the policy. This was confirmed by a progressive reduction in newborn retrievals secondary to elective caesarean during the study period (28 in 2006, 20 in 2007, 18 in 2008 and 13 in 2009).
There is increasing concern about the neurodevelopmental outcomes for late preterm babies.15 It is important to optimise their outcomes through planned births in facilities that are able to provide an appropriate level of care to the baby at birth, and that adhere strictly to elective caesarean section guidelines. The cost of a potentially avoidable retrieval is difficult to quantify. It not only includes the cost of the retrieval process but also includes the cost of continued stay in the referral centre, back transfer to the referring hospital and financial cost to the family. The inconvenience, lactation and bonding difficulties, and anxiety and uncertainty due to separation of the mother and baby are immeasurable.
1 Retrievals, live births and retrieval rates over the study period
Retrievals per 10 000 live births |
|||||||||||||||
2 Retrievals, live births and retrieval rates at each level* of referring public hospital and at private hospitals over the study period
* Hospital levels are based on resources and skill availability (Appendix). |
|||||||||||||||
3 Potentially avoidable retrieval rates per 10 000 live births at each level* of referring public hospital and at private hospitals
* Hospital levels are based on resources and skill availability (Appendix). |
|||||||||||||||
Received 3 January 2013, accepted 20 August 2013
- Himanshu P Popat1
- Margaret Wall2
- Kathryn A Browning Carmo2
- Andrew Berry2
- 1 Royal Prince Alfred Hospital Newborn Care, Sydney, NSW.
- 2 Newborn and Paediatric Emergency Transport Service, Sydney Children’s Hospital Network, Sydney, NSW.
No relevant disclosures.
- 1. Kollée LA, Verloove-Vanhorick PP, Verwey RA, et al. Maternal and neonatal transport: results of a national collaborative survey of preterm and very low birth weight infants in The Netherlands. Obstet Gynecol 1988; 72: 729-732.
- 2. Towers CV, Bonebrake R, Padilla G, Rumney P. The effect of transport on the rate of severe intraventricular hemorrhage in very low birth weight infants. Obstet Gynecol 2000; 95: 291-295.
- 3. Simpson JM, Evans N, Gibberd RW, et al. Analysing differences in clinical outcomes between hospitals. Qual Saf Health Care 2003; 12: 257-262.
- 4. Kitchen W, Ford G, Orgill A, et al. Outcome of extremely low birth-weight infants in relation to the hospital of birth. Aust N Z J Obstet Gynaecol 1984; 24: 1-5.
- 5. Truffert P, Goujard J, Dehan M, et al. Outborn status with a medical neonatal transport service and survival without disability at two years. A population-based cohort survey of newborns of less than 33 weeks of gestation. Eur J Obstet Gynecol Reprod Biol 1998; 79: 13-18.
- 6. Saigal S, Rosenbaum P, Hattersley B, Milner R. Decreased disability rate among 3-year-old survivors weighing 501 to 1000 grams at birth and born to residents of a geographically defined region from 1981 to 1984 compared with 1977 to 1980. J Pediatr 1989; 114: 839-846.
- 7. National Health and Medical Research Council. Clinical practice guidelines: care around preterm birth. Canberra: Commonwealth of Australia, 2000. http://www.nhmrc.gov.au/_files_nhmrc/publications/attachments/cp51.pdf (accessed Aug 2009).
- 8. Lui K, Abdel-Latif ME, Allgood CL, et al. Improved outcomes of extremely premature outborn infants: effects of strategic changes in perinatal and retrieval services. Pediatrics 2006; 118: 2076-2083.
- 9. NSW Health. Extract from NSW Health Statewide Services Development Branch. Guide to role delineation of health services. Core services — maternity and child health services. Sydney: NSW Health, 2002.
- 10. Hansen AK, Wisborg K, Uldbjerg N, Henriksen TB. Elective caesarean section and respiratory morbidity in the term and near-term neonate. Acta Obstet Gynecol Scand 2007; 86: 389-394.
- 11. NSW Health. Maternity - timing of elective or pre-labour caesarean section. Policy directive. 3 April 2007. http://www0.health.nsw.gov.au/policies/pd/2007/pdf/PD2007_024.pdf (accessed Jan 2013).
- 12. Tita AT, Landon MB, Spong CY, et al. Timing of elective repeat cesarean delivery at term and neonatal outcomes. N Engl J Med 2009; 360: 111-120.
- 13. Morrison JJ, Rennie JM, Milton PJ. Neonatal respiratory morbidity and mode of delivery at term: influence of timing of elective caesarean section. Br J Obstet Gynaecol 1995; 102: 101-106.
- 14. National Institute for Health and Clinical Excellence. Caesarean section. NICE clinical guideline 132. August 2012. http://www.nice.org. uk/nicemedia/live/13620/57163/57163.pdf (accessed Jan 2013).
- 15. de Jong M, Verhoeven M, van Baar AL. School outcome, cognitive functioning, and behaviour problems in moderate and late preterm children and adults: a review. Semin Fetal Neonatal Med 2012; 17: 163-169.
Abstract
Objective: To identify areas for improvement in outcomes in retrieved newborns by reviewing newborn retrieval activity and evaluating potentially avoidable retrievals from each referring hospital stratified by the level of service delivery over the study period.
Design: A retrospective analysis of newborn retrievals from 1 January 2006 to 31 December 2009.
Setting: Newborn and Paediatric Emergency Transport Service (NETS).
Participants: Newborns less than 72 hours old retrieved by NETS in the study period. Each retrieval was classified as potentially avoidable, unavoidable or unclassified, based on predefined criteria.
Main outcome measures: Newborn retrieval rates (per 10 000 live births) and potentially avoidable retrievals for each referring hospital level and overall.
Results: There were 2494 newborn retrievals over the study period, with an annual mean of 623 total and 30 potentially avoidable retrievals. There was a reduction in the potentially avoidable retrieval rate (per 10 000 live births) over the study period (from 3.9 in 2006 and 4.2 in 2007 to 2.2 in 2008 and 2.3 in 2009) despite an increase in the total retrieval rate over the same time. Discretionary caesarean, defined as elective (pre-labour) caesarean section without documented fetal or maternal indications before 39 completed weeks of gestation, accounted for two-thirds of the potentially avoidable retrievals.
Conclusions: Potentially avoidable retrievals were a small but significant proportion and are becoming less frequent. Discretionary caesarean is the most common cause of potentially avoidable retrieval. Strict implementation of the elective caesarean section policy directive has the potential to reduce morbidity and the costs related to retrieval.