




There are about 4400 registered practising chiropractors in Australia,1 making chiropractic the eighth largest registered health profession (out of 10).2 During 2005, 16% of Australians, over 3 million people, consulted a chiropractor at least once3 at an out-of-pocket cost of $905 million.4
Despite the large number of people who receive chiropractic care, very little is known about why people seek this care and what care chiropractors provide. With the increased attention, and criticism, directed at the chiropractic profession, it is important to have reliable up-to-date information about what is actually happening in chiropractic clinical practice.5
Previous attempts to document this practice in Australia are now outdated.6-13 Worldwide, systematic approaches to gathering information about chiropractic practice have been limited by study design, including chart abstraction, patient recall surveys, practitioner recall surveys and reviews of administrative databases.14-22
The Chiropractic Observation and Analysis Study (COAST) aimed to describe the clinical practices of chiropractors in Victoria, Australia. COAST used methods developed by the Bettering the Evaluation and Care of Health (BEACH) program. BEACH is a continuous, rigorous, national study of Australian general medical practice clinical activity and has been running since 1998.23,24 COAST documented the following:
COAST was a cross-sectional observational study of chiropractic practice in Victoria, Australia.
A random sample of 180 chiropractors from the list of 1298 chiropractors registered on the Chiropractors Registration Board of Victoria were invited to participate, using a modified tailored design method.25 BEACH investigators have determined that a minimum sample of 40 health care practitioners is required to ensure reasonable precision for more frequent events; on this basis, and given the resources available to complete this study, we approached 180 chiropractors, anticipating a 30% response rate.
Chiropractors recorded anonymous patient encounter data by hand on paper encounter recording forms, with items in free text or check box format (Appendix 1). A pad of 106 forms was supplied to each chiropractor, with extra forms provided in case of mistakes. The encounter recording form was based on the BEACH study encounter form and was modified to reflect chiropractic practice. The forms were first piloted with five chiropractors with varying practice styles who each collected data on 10 consecutive patients. The data collection form is available on request.
Chiropractors recorded terms on the encounter form that they believed most accurately described the encounter. These terms were then entered and classified by a coder according to the International classification of primary care, 2nd edition (ICPC-2) using the Australian ICPC-2 PLUS general practice terminology.26,27 For example, for the patient reason for encounter (RFE) or the problem and diagnosis, the research team anticipated that terms would be recorded by the chiropractors to describe patients who presented with little or no symptoms at the time of the encounter. Terms used to describe such visits would be related to wellbeing, wellness, health maintenance and check-up.28,29 Such wellness-related terms were coded to the ICPC chapter “general and unspecified”.
Where an RFE, a problem and diagnosis, or process of care was documented that had no corresponding ICPC-2 PLUS term, a new term (and code) was created. A detailed explanation of the coding, process for generating new terms relevant to the chiropractic profession, and subsequent coding and grouping system has been previously published.30
Descriptive statistics were used to summarise chiropractor, patient and encounter characteristics. RFEs were reported by ICPC chapter, and chiropractor-identified problems and diagnoses were reported by groups of related ICPC-2 PLUS terms. For each chiropractor, patients attending more than once during the 100 encounters recorded were identified by date of birth, sex and postcode. Analyses were undertaken using Stata version 12 (StataCorp) and 95% CIs were calculated for all relevant estimates. The survey estimator procedures in Stata were used to adjust for the clustering effect and to calculate the design effect (Deff). The intracluster correlation coefficient (ICC) was then calculated from the Deff using the formula ICC = (Deff − 1)/(k − 1), where k is the average number of consultations across all chiropractors.31
We compared participating chiropractors’ sex and years in practice, and the proportion practising in a rural setting, with data on all practising Victorian chiropractors provided by the Chiropractors Registration Board of Victoria. We also compared chiropractor characteristics with available data (age and sex only) from the Australian Health Practitioner Regulation Agency.1 We used one-sample t tests using population mean (years in practice) and population proportion (sex, rural practice setting), along with the χ2 goodness-of-fit test for age ranges (with recoding of COAST data to ensure ranges were uniform across the two datasets).
Of the original 180 chiropractors approached, 24 were ineligible. Of those who were eligible, 72 agreed to participate (46% response rate); 20 of these withdrew and did not provide any data, and 52 (33%) completed the study. Participating chiropractors provided information on 4464 chiropractor–patient encounters between 11 December 2010 and 28 September 2012. Appendix 2 shows the flow of chiropractor participants through the study. Not all chiropractors provided information on 100 encounters: 33 out of 52 provided information on at least 100, 13 provided information on 50–100, and six provided information on less than 50 encounters.
Box 1 shows the characteristics of participating chiropractors. Compared with all registered chiropractors in Victoria, those who participated in COAST had similar mean time since graduation (16 years), and a similar proportion worked in an urban location (35/52 [67%] compared with 626/894 [70%]). However, a smaller proportion of COAST participants were women (14/52 [27%] compared with 399/1050 [38%]), but this difference was not statistically significant. Similarly, compared with all Australian chiropractors, participating chiropractors were of similar age, but there was a non-statistically significant under-representation of women in this study (14/52 [27%]) compared with national data (1679/4664 [36%]).
Box 2 shows the demographic details of patients who sought chiropractic care and the source of payment for encounters. In most chiropractor–patient encounters (71%), patients were aged 25–64 years. In 9% of encounters, patients were younger than 15 years old, and in 13%, patients were aged 65 years and older. In 81% (95% CI, 76%–86%) of encounters, patients paid for some or all of the consultation fee. For 13% of encounters, it was a repeat visit where a patient presented at least twice during the 100 recorded encounters.
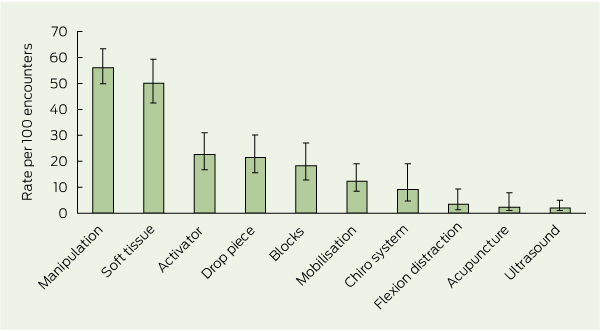
The distribution of problems and diagnoses managed in the encounters, as identified by the chiropractors, is shown in Box 3. Spinal problems, including chiropractor-recorded terms such as “chiropractic subluxation” (a term used by some chiropractors to describe a perceived dysfunction detected in a joint segment32), and joint dysfunction were the most commonly identified problems and diagnoses. Box 4 shows the techniques and care provided by the chiropractors. The most frequent were manual adjustments (manipulation) and soft tissue therapy. Other care provided by chiropractors during the encounters included (reported as rates per 100 encounters): therapeutic exercise prescription (52; 95% CI, 44–61), advice about exercises in general (21; 95% CI, 15–29), advice about posture (21; 95% CI, 10–18), and recommendations to use ice packs (11; 95% CI, 7–18), heat therapy (8; 95% CI, 4–18) and supplements (5; 95% CI, 3–8). Other recommendations were coded at a rate of less than four per 100 encounters (full results available on request).
There is evidence of patient referral between GPs and chiropractors, albeit in only a small proportion of encounters. In the general population, most people who see a chiropractor, and other complementary and alternative practitioners, also consult a medical practitioner.3 Further research is required to maximise the patient benefit that can be gained through a team approach to primary care.
The common use of maintenance and wellness-related terms reflects current debate in the chiropractic profession. “Chiropractic wellness care” is considered by an indeterminate proportion of the profession as an integral part of chiropractic practice,28 with the belief that regular chiropractic care may have value in maintaining and promoting health, as well as preventing disease.29 The definition of wellness chiropractic care is controversial, with some chiropractors promoting only spine care as a form of wellness, and others promoting evidence-based health promotion, eg, smoking cessation and weight reduction, alongside spine care.28 A 2011 consensus process in the chiropractic profession in the United States emphasised that wellness practice must include health promotion and education, and active strategies to foster positive changes in health behaviours.28
The response rate for this study, 33% of the eligible chiropractors approached, is higher than that achieved in the BEACH study in 2011 (27%).23 The response rates for two recent Australian national surveys of the chiropractic profession, one about workforce and one about low back pain, were 23%33 and 37%,34 respectively. The response rate for this study was similar to that obtained in the first general practice morbidity and prescribing survey conducted from 1969 to 1974 (29%).35,36 For simple postal surveys of health professionals, response rates have been declining over the past 10 years.37 The burden on practitioners to participate in this study may have affected response rates, further compounded by 28% of chiropractors withdrawing after initially agreeing to participate, some of whom withdrew when they realised the amount of work involved. However, of those who did complete the study, 78% indicated they would recommend participating in COAST to other chiropractors. Ideally, data obtained in this study would be routinely collected in chiropractic practice, but infrastructure is not in place to facilitate this, with two-thirds of chiropractors who participated using paper-only clinical records; hence clinical data cannot be easily captured.
1 Characteristics of 52 chiropractors participating in COAST
Other non-chiropractic health care practitioner available at same premises |
|||||||||||||||
2 Characteristics of patients in encounters recorded by participating chiropractors
* Missing values not used in calculations. † Multiple payment options allowed, so total not 100%. |
|||||||||||||||
3 Distribution of problems managed (20 most frequent problems), as reported by chiropractors
ICC = intracluster correlation coefficient. * Excludes repeat problem group managed at encounter. |
|||||||||||||||
Received 19 December 2012, accepted 19 September 2013
- Simon D French1,2
- Melanie J Charity1
- Kirsty Forsdike1
- Jane M Gunn1
- Barbara I Polus3
- Bruce F Walker4
- Patty Chondros1
- Helena C Britt5
- 1 General Practice and Primary Health Care Academic Centre, University of Melbourne, Melbourne, VIC.
- 2 School of Rehabilitation Therapy, Queen’s University, Kingston, Ontario, Canada.
- 3 Research and Innovation, RMIT University, Melbourne, VIC.
- 4 Discipline of Chiropractic, School of Health Professions, Murdoch University, Perth, WA.
- 5 Family Medicine Research Centre, Sydney School of Public Health, University of Sydney, Sydney, NSW.
This study was funded by the Chiropractors Registration Board of Victoria and the Chiropractors Association of Australia. The funding bodies provided general advice about the design of the project but had no role in the conduct of the study or in the decisions about publication of the results. We thank the members of the Advisory Committee of chiropractic professional organisations including: Amanda Kimpton (Chiropractic Board of Australia), Simon Floreani (Chiropractors Association of Australia), Navine Haworth (Discipline of Chiropractic, School of Health Sciences, RMIT University), John Reggars (Chiropractic and Osteopathic College of Australasia) and Margaret Nicholls (consumer). We thank Maria Potiriadis for project planning advice during the course of the project. We thank the chiropractor and patient participants for their efforts in participating in this study.
No relevant disclosures.
- 1. Chiropractic Board of Australia, Australian Health Practitioner Regulation Agency. Chiropractic registrant data: March 2013. http://www.chiropracticboard.gov.au/About-the-Board/Statistics.aspx (accessed Oct 2013).
- 2. Australian Health Practitioner Regulation Agency. 2011–12 annual report: AHPRA and national boards. http://www.ahpra.gov.au/Legislation-and-Publications/AHPRA-Publications.aspx#annual (accessed Oct 2013).
- 3. Xue CC, Zhang AL, Lin V, et al. Complementary and alternative medicine use in Australia: a national population-based survey. J Altern Complement Med 2007; 13: 643-650.
- 4. Xue CC, Zhang AL, Lin V, et al. Acupuncture, chiropractic and osteopathy use in Australia: a national population survey. BMC Public Health 2008; 8: 105.
- 5. MacLennan AH, Morrison RG. Tertiary education institutions should not offer pseudoscientific medical courses. Med J Aust 2012; 196: 225-226. <MJA full text>
- 6. Report of the Committee of Inquiry into Chiropractic, Osteopathy, Homoeopathy and Naturopathy. Canberra: Australian Government Publishing Service, 1977.
- 7. Ebrall PS. A descriptive report of the case-mix within Australian chiropractic practice, 1992. Chiropr J Aust 1993; 23: 92-97.
- 8. Ebrall PS. A description of chiropractic and osteopathic practice in the state of Victoria, Australia, for 1989. Chiropr J Aust 1992; 22: 92-97.
- 9. Leboeuf C. A survey of registered chiropractors practising in South Australia in 1986. J Aust Chiropr Assoc 1988; 18: 105-110.
- 10. Leboeuf C, Webb MN. Recently graduated chiropractors in Australia, part 1: personal and professional demographic profile. J Aust Chiropr Assoc 1987; 17: 99-102.
- 11. Leboeuf C, Webb MN. Recently graduated chiropractors in Australia, part 2: certain professional attitudes and practice characteristics. J Aust Chiropr Assoc 1987; 17: 151-154.
- 12. Leboeuf C, Webb MN. Recently graduated chiropractors in Australia, part 4: diagnostic procedures. J Aust Chiropr Assoc 1988; 18: 60-62.
- 13. Leboeuf C, Webb MN. Recently graduated chiropractors in Australia, part 5: therapeutic procedures. J Aust Chiropr Assoc 1988; 18: 128-130.
- 14. Mootz RD, Cherkin DC, Odegard CE, et al. Characteristics of chiropractic practitioners, patients, and encounters in Massachusetts and Arizona. J Manipulative Physiol Ther 2005; 28: 645-653.
- 15. Blum C, Globe G, Terre L, et al. Multinational survey of chiropractic patients: reasons for seeking care. J Can Chiropr Assoc 2008; 52: 175-184.
- 16. Coulter ID, Hurwitz EL, Adams AH, et al. Patients using chiropractors in North America: who are they, and why are they in chiropractic care? Spine (Phila Pa 1976) 2002; 27: 291-296; discussion 297-298.
- 17. Dunn AS, Passmore SR. Consultation request patterns, patient characteristics, and utilization of services within a Veterans Affairs medical center chiropractic clinic. Mil Med 2008; 173: 599-603.
- 18. Hurwitz EL, Coulter ID, Adams AH, et al. Use of chiropractic services from 1985 through 1991 in the United States and Canada. Am J Public Health 1998; 88: 771-776.
- 19. Leboeuf-Yde C, Hennius B, Rudberg E, et al. Chiropractic in Sweden: a short description of patients and treatment. J Manipulative Physiol Ther 1997; 20: 507-510.
- 20. Rubinstein S, Pfeifle CE, van Tulder MW, Assendelft WJ. Chiropractic patients in the Netherlands: a descriptive study. J Manipulative Physiol Ther 2000; 23: 557-563.
- 21. Assendelft WJ, Pfeifle CE, Bouter LM. Chiropractic in The Netherlands: a survey of Dutch chiropractors. J Manipulative Physiol Ther 1995; 18: 129-134.
- 22. Christensen MG, Kollasch MW, Martin W, Hyland JK. Practice analysis of chiropractic: a project report, survey analysis and summary of the practice of chiropractic within the United States — 2010. Greeley, Colo: National Board of Chiropractic Examiners, 2010.
- 23. Britt H, Miller G, Henderson J, et al. General practice activity in Australia 2011–12. General practice series no. 31. Sydney: Sydney University Press, 2012.
- 24. Britt H, Miller G, Bayram C. The quality of data on general practice - a discussion of BEACH reliability and validity. Aust Fam Physician 2007; 36: 36-40.
- 25. Dillman DA. Mail and internet surveys: the tailored design method: with new internet, visual, and mixed-mode guide. 2nd ed. Hoboken, NJ: John Wiley & Sons, 2007.
- 26. Classification Committee of the World Organization of Family Doctors (WONCA). ICPC-2. International Classification of Primary Care, 2nd ed. Oxford: Oxford University Press, 1998.
- 27. University of Sydney Family Medicine Research Centre. ICPC-2 Plus: the BEACH coding system. http://sydney.edu.au/medicine/fmrc/icpc-2-plus/index.php (accessed Oct 2013).
- 28. Hawk C, Schneider M, Evans MW Jr, Redwood D. Consensus process to develop a best-practice document on the role of chiropractic care in health promotion, disease prevention, and wellness. J Manipulative Physiol Ther 2012; 35: 556-567.
- 29. Leboeuf-Yde C, Hestbaek L. Maintenance care in chiropractic–what do we know? Chiropr Osteopat 2008; 16: 3.
- 30. Charity MJ, French SD, Forsdike K, et al. Extending ICPC-2 PLUS terminology to develop a classification system specific for the study of chiropractic encounters. Chiropr Man Therap 2013; 21: 4.
- 31. Knox SA, Chondros P. Observed intra-cluster correlation coefficients in a cluster survey sample of patient encounters in general practice in Australia. BMC Med Res Methodol 2004; 4: 30.
- 32. World Health Organization. WHO guidelines on basic training and safety in chiropractic. Geneva: WHO, 2005. http://www.who.int/medicines/areas/traditional/Chiro-Guidelines.pdf (accessed Oct 2013).
- 33. Eaton S, Bonello R, Fernandez-Caamano R, et al. Demographic characteristics and perceptions of supply and demand of chiropractic services in Australia: results from stage 1 of the work force study survey. Chiropr J Aust 2012; 42: 82-90.
- 34. Walker BF, French SD, Page MJ, et al. Management of people with acute low-back pain: a survey of Australian chiropractors. Chiropr Man Therap 2011; 19: 29.
- 35. Bridges-Webb C. The Australian general practice morbidity and prescribing survey, 1969 to 1974. 2. Method, analysis and limitations. Med J Aust 1976; 2 (I Suppl): 6-7.
- 36. Bridges-Webb C. The Australian general practice morbidity and prescribing survey, 1969 to 1974. The Royal Australian College of General Practitioners. 1. Introduction. Med J Aust 1976; 2 (I Suppl): 5-6.
- 37. Cook JV, Dickinson HO, Eccles MP. Response rates in postal surveys of healthcare professionals between 1996 and 2005: an observational study. BMC Health Serv Res 2009; 9: 160.
Abstract
Objectives: COAST (Chiropractic Observation and Analysis Study) aimed to describe the clinical practices of chiropractors in Victoria, Australia.
Design: Cross-sectional study using the BEACH (Bettering the Evaluation and Care of Health) methods for general practice.
Setting and participants: 180 chiropractors in active clinical practice in Victoria were randomly selected from the list of 1298 chiropractors registered on Chiropractors Registration Board of Victoria. Twenty-four chiropractors were ineligible, 72 agreed to participate, and 52 completed the study.
Main outcome measures: Each participating chiropractor documented encounters with up to 100 consecutive patients. For each chiropractor–patient encounter, information collected included patient health profile, patient reasons for encounter, problems and diagnoses, and chiropractic care.
Results: Data were collected on 4464 chiropractor–patient encounters from 52 chiropractors between 11 December 2010 and 28 September 2012. In most (71%) encounters, patients were aged 25–64 years; 1% of encounters were with infants (age < 1 year; 95% CI, 0.3%–3.2%). Musculoskeletal reasons for encounter were described by patients at a rate of 60 per 100 encounters (95% CI, 54–67 encounters) and maintenance and wellness or check-up reasons were described at a rate of 39 per 100 encounters (95% CI, 33–47 encounters). Back problems were managed at a rate of 62 per 100 encounters (95% CI, 55–71 encounters). The most frequent care provided by the chiropractors was spinal manipulative therapy and massage.
Conclusions: A range of conditions are managed by chiropractors in Victoria, Australia, but most commonly these conditions are musculoskeletal-related. These results can be used by stakeholders of the chiropractic profession in workforce development, education and health care policy.