





Volume 197 - Issue 5
Online chlamydia testing: an innovative approach that appeals to young people
Authors: Kellie S H Kwan, Edwina A Jachimowicz, Lisa Bastian, Lewis Marshall and Donna B Mak
Med J Aust 2012; 197 (5): 287-290. || doi: 10.5694/mja11.11517
Published online: 3 September 2012
Published online: 3 September 2012
Chlamydia, caused by the bacteria Chlamydia trachomatis, is a sexually transmitted infection (STI) and the most commonly notified disease in Australia and in Western Australia ...
Abstract
Objective: To evaluate data from an online chlamydia testing program (OLC) developed to increase young people’s access to testing for chlamydia, the most commonly notified disease in Australia and Western Australia, with a high proportion of notifications among young people (< 30 years).
Design and setting: The OLC was launched in February 2010, and our study covers the period February 2010 to June 2011. Without needing to first visit a doctor, OLC participants receive risk self-assessment, education, testing, and, if necessary, referral for treatment, and can complete an online satisfaction survey.
Main outcome measures: Number and proportion of downloaded pathology forms that resulted in a test; demographic characteristics of participants; prevalence of chlamydia; completeness and timeliness of follow-up of positive test results; and participant satisfaction.
Results: More than half (56%) of the 675 OLC pathology form downloads resulted in a test, and chlamydia was detected in 18% (66/377). Of those tested, over half were men (55%), and 71% were aged < 30 years. All participants with a positive test result received appropriate clinical management, with 50% being treated within 7 days of specimen collection. Of the 17% (55/332) who completed an online satisfaction survey, almost all said they would recommend the service to a friend.
Conclusion: Internet-based screening for chlamydia is an effective means of increasing access to testing for young people at risk of sexually transmitted infections and is a valuable addition to opportunistic, clinic-based strategies.
Chlamydia, caused by the bacteria Chlamydia trachomatis, is a sexually transmitted infection (STI) and the most commonly notified disease in Australia and in Western Australia.1 Between 2001 and 2010, the number of chlamydia infections reported to the Department of Health, WA (DoHWA) increased more than threefold, from 2707 notifications in 2001 to 10 249 in 2010.2 As in previous years, 84% of the chlamydia notifications in WA in 2010 were among young people (age, < 30 years), with peaks in those aged 20–24 and 15–19 years (36% and 28% of notifications, respectively).2 As asymptomatic chlamydia infection is common among men and women, infections may not be detected or treated in a timely fashion. This increases the likelihood of disease transmission and the development of complications, such as pelvic inflammatory disease and infertility.3
Increasing the number of people aged 16–25 years being tested for chlamydia infection is a key objective of Australia’s Second national sexually transmissible infections strategy 2010–2013.4 However, several barriers to achieving this increase have been identified, especially among young people with asymptomatic infections. These barriers include costs associated with testing, clinic waiting times, inconvenience, fear of medical procedures, stigma and lack of privacy.5-8 In addition, not all general practitioners in Australia routinely offer chlamydia testing to young people; in particular, men as well as young people in rural settings may be missing out on testing.9
Home-based chlamydia testing has been trialled in several countries as a means of overcoming traditional barriers to testing, with kits advertised and ordered online, or distributed by mail or in the community.10-18 In these models, vaginal and penile swabs or urine samples are taken at home and returned via post. However, uptake has generally been low, limiting the effectiveness of home-based testing. A potential reason for this may be that young people living with their parents, a sexual partner or in shared accommodation are less likely to order or use a chlamydia testing kit at home for fear of arousing suspicion; for example, when receiving an unmarked package in the mail.18
In 2010, the DoHWA established an online chlamydia testing program (OLC) that allows participants to complete a risk self-assessment for chlamydia online and submit a sample for testing at a laboratory without visiting a doctor. The OLC is described in detail in Box 1. Here, we evaluate the OLC from February 2010 to June 2011.
Methods
The main outcome measures of interest were: (i) the number and proportion of downloaded pathology forms that resulted in a test; (ii) the demographic characteristics of OLC participants; (iii) chlamydia prevalence among OLC participants; (iv) completeness and timeliness of follow-up of OLC participants with positive test results; and (v) participant satisfaction with the OLC. Each pathology test generated via the OLC is referred to as a “participant”.
Pathology form download data were obtained from Google Analytics (http://www.google.com/analytics/index.html). All other clinical data were obtained from the dedicated OLC database at the B2 Sexual Health Clinic at Fremantle Hospital (Box 1).
Poisson regression, with a flexible scale parameter, was used to analyse the trend in the number of pathology form downloads and the number of pathology tests per month. Changes in the proportion of downloaded pathology forms resulting in a test was assessed using a χ2 test for trend.
Data were analysed using IBM SPSS Statistics, version 19 (SPSS Inc), and Excel (Microsoft). A significance level of 5% was used to assess statistical significance.
As a Medicare number or other proof of identify was not required for submitting a specimen for testing, participants may have submitted more than one specimen under different names. Thus, it was not possible to analyse the data based on unique individuals.
Results
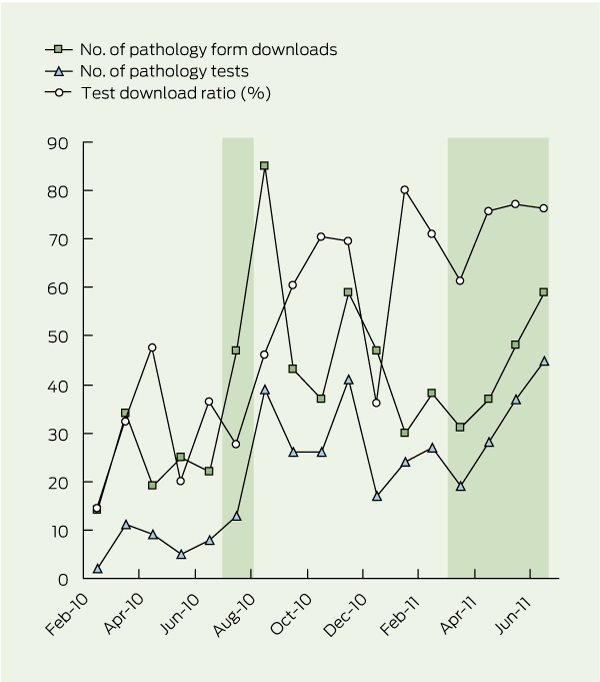
Between February 2010 and June 2011, there were 675 pathology form downloads and 377 pathology tests performed. While the frequency of pathology form downloads tended to increase with time, the effect was not statistically significant (monthly percentage change, 3.5%; 95% CI, −0.8% to 8.0%); however, the number of pathology tests increased significantly (monthly percentage change, 9.5%; 95% CI, 4.3%–14.9%) (Box 2). Fifty-six per cent (n = 377) of downloaded pathology forms resulted in a test, and this proportion increased over time (χ2 test for trend, 67.81; P < 0.001).
Demographic characteristics of the 377 participants tested, who were aged between 16 and 63 years, are shown in Box 3; 71% (n = 267) were aged < 30 years, men outnumbered women, and 37% (n = 141) reported current perceived STI symptoms, the presence of an STI in a sexual contact(s) and/or a past history of an STI. Chlamydia prevalence was 18% (66/377; 95% CI, 14%–21%) overall, and 47% (21/45; 95% CI, 32%–61%) and 68% (27/40; 95% CI, 53%–82%) in participants reporting current perceived STI symptoms and the presence of an STI in sexual contact(s), respectively.
All participants found to have chlamydia, and one additional participant found to have gonorrhoea, were treated with appropriate antibiotics, and partner notification and post-treatment follow-up were undertaken. The median time from specimen collection to treatment was 7 days, with 94% (62/66) of participants being treated within 14 days; the longest interval of 32 days occurred in a participant who went overseas after testing and was treated on return.
Of the 332 participants tested between February 2010 and May 2011, 17% completed the satisfaction survey (n = 55: 28 men and 27 women; 28 aged > 25 years and 27 aged < 25 years). Forty-five per cent (25/55) found out about the OLC via an internet search; other methods included mass media advertising, word of mouth and health care providers. Almost all respondents reported that the OLC was easy to use (53/55) and that they would recommend it to a friend (54/55).
Discussion
More than half (56%) of the 675 OLC pathology form downloads resulted in a test, and chlamydia was detected in 18%. Of those tested, over half were men (55%), and 71% were young people aged < 30 years. All participants with a positive test result underwent appropriate clinical management, with 50% being treated within 7 days of specimen collection. Among those completing the online survey, satisfaction with the OLC was high and almost all said they would recommend the service to a friend.
The observed proportions of pathology form downloads resulting in a test (56%) and positive tests (18%) were higher than those reported in many other comparable internet-based testing strategies, in which test return rates ranged from 34% to 62%13,19 and positive test results from 3% to 14%.10,13,15,17,19,20 Our results, coupled with the fact that 71% of OLC participants were < 30 years of age, indicate that this service is being used by young people who are actually at risk of STI, rather than by the “worried well”. They also suggest that the OLC method of internet-based testing may be more appealing to young people, as it eliminates some of the concerns preventing them from accessing traditional STI testing strategies,5-8 and therefore is an effective means of increasing testing rates among this cohort.
Another strength of the OLC is its potential to reach traditionally difficult-to-access populations for chlamydia testing and sexual health education. In Australia, only 1.6% and 6.3% of 15–24-year-old men and women, respectively, are opportunistically tested for chlamydia by their GP.9 The relative overrepresentation of males among OLC participants suggests that this method of accessing testing is acceptable to young men. The requirement to complete an online risk self-assessment before accessing the test request form also provides an opportunity for participants, especially those who are less likely to access health care (such as young men), to learn about, or be reminded of, behaviours and symptoms associated with chlamydia and other STIs.
Completeness of clinical management for all participants with positive test results indicates that participants were serious about getting tested and willing to provide their correct contact details on an online pathology form. The median time from specimen collection to treatment of 7 days was comparable with the range of 5–7 days reported from Australian and overseas sexual health clinics.21,22
Limitations of our study include the fact that only 17% of participants completed the satisfaction survey, and that the data could not be analysed by unique individuals because participation did not require proof of identify.
Two groups were underrepresented among OLC participants: Aboriginal people (1% of OLC participants v 4% of WA’s estimated 15–29-year-old population in 2009); and people living outside the metropolitan area (9% of OLC participants v 26% of WA’s estimated 15–29-year-old population in 2010) (Rates Calculator, version 9.5.3.1, Epidemiology and GIS Branch, DoHWA, Perth, 2009). This may reflect the “mainstream” nature of DoHWA’s mass media campaigns undertaken to raise awareness of the OLC, poorer access to internet services and/or reduced access to PathWest collection centres, especially in remote areas.
The internet is an important source of sexual health information among young people in Australia,23 and 45% of OLC participants found out about the program through an internet search. Internet-based chlamydia screening strategies are competitively cost-effective in comparison with traditional clinic-based screening approaches.24 However, a cost-effectiveness analysis was outside the scope of our study.
The accessibility and effectiveness of the OLC may therefore increase, as the popularity of the internet as a sexual health information resource also increases over time. Promotion of the OLC using internet-based social media sites to increase uptake may be considered in the future.
The results of our study demonstrate that internet-based screening for chlamydia is a highly effective means of increasing access to testing among young people at risk of STIs and is a valuable addition to traditional opportunistic, clinic-based strategies.
1 Online chlamydia testing program (OLC) of the Western Australia Department of Health (DoHWA)
Program launch: The OLC was launched in February 2010 and, for logistical reasons, until July 2010, it was accessible only through the DoHWA’s youth sexual health information website, “Get the facts” (www.getthefacts.health.wa.gov.au). Since then, it has also been available from the DoHWA’s chlamydia information website, “Could I have it” (www.couldihaveit.com.au). To raise awareness of the program among 16–25-year-olds, mass media campaigns (print, radio and convenience advertising in pubs, clubs, cafes and universities) were conducted from 25 July to 7 August 2010 (2 weeks) and from March to June 2011 (4 months). Participants: Participants must be ≥ 16 years, have a mobile telephone number, access to the internet and a printer, and be able to visit a PathWest Laboratory Medicine WA (PathWest) collection centre (> 70 throughout WA). Online prompts refer people aged < 16 years to the Sexual Health Helpline (a telephone advice service run by FPWA Sexual Health Services) or to a clinical service, and also advise those with symptoms of a sexually transmitted infection (STI) to immediately see a medical practitioner. Online risk self-assessment: A six-question risk self-assessment is completed by participants to determine any history of unprotected oral, anal or vaginal sex; new sexual contact(s) in the past 6 months; past and current symptoms of chlamydia; history of an STI, and presence of an STI in sexual contact(s). PathWest test request: Participants then complete a PathWest test request form online with mandatory fields including first name, surname, date of birth, sex, Aboriginality, address and mobile telephone number. The write-protected form can then be printed and taken by the participant to |
a PathWest collection centre. Locations of the collection centres are listed on the request form. Specimen collection: Participants are advised that men will be asked to provide a urine sample, and women will be asked to provide a self-obtained lower vaginal swab. Instructions on specimen collection can be downloaded when completing the test request form. Specimen collection equipment is provided at the collection centre. Participants are advised that the test also detects gonorrhoea, as the nucleic acid amplification test used by PathWest routinely tests for both organisms. The DoHWA pays the Medicare rate for each test, so no cost is incurred by participants. Test results: All test results are reported to the B2 Sexual Health Clinic at Fremantle Hospital (B2 Clinic). Participants are advised that their test result should be available in 3 working days in the Perth metropolitan area and 5 working days in the non-metropolitan area. All participants may call the B2 Clinic registered nurse on a toll-free telephone number to find out their test result or ask questions. All participants obtaining results also receive a sexual health risk assessment, safer sex education and, if appropriate, referral for further testing. Treatment: A registered nurse from the B2 Clinic contacts participants who have a positive chlamydia and/or gonorrhoea test result using the mobile telephone number provided by the participant, and advises them to visit a doctor for antibiotic treatment. With the participant’s permission, a letter of referral to his or her nominated GP explaining the program and the result can be emailed to the participant. Alternatively, participants may elect to be treated at the B2 Clinic or another DoHWA-funded sexual health service. Contact tracing and DoHWA notification are also done by the B2 Clinic nurses. Participants’ clinical data are stored at the B2 Clinic in a dedicated, password-protected Access database (Microsoft). Satisfaction survey: All participants who contact the B2 Clinic are asked to complete an anonymous online participant-satisfaction survey enquiring about how they found out about the OLC and their satisfaction with the service. |
||||||||||||||
2 Online chlamydia testing program (OLC) — number of downloads of test request forms and pathology tests performed, and proportion of downloaded forms resulting in a test, by month, February 2010 to June 2011*
* Shaded areas indicate periods during which a mass media campaign was conducted to raise awareness of the program (25 July to 7 August 2010 and March to June 2011).
3 Chlamydia prevalence in an online chlamydia testing program, by demographic characteristics of participants and self-reported reason(s) for testing, February 2010 to June 2011
Competing interests
No relevant disclosures.
Acknowledgements
We thank Melanie Lau for undertaking the Poisson regression component of data analysis.
References
- The Kirby Institute. HIV/AIDS, viral hepatitis and sexually transmissible infections in Australia annual surveillance report 2011. Sydney: The Kirby Institute, The University of New South Wales, 2011. http://www.med.unsw.edu.au/NCHECRweb.nsf/resources/2011/$file/KIRBY_ASR2011.pdf (accessed Nov 2011).
- Government of Western Australia Department of Health. The epidemiology of notifiable sexually transmitted infections and blood-borne viruses in Western Australia 2010. Perth: DoH, WA, 2011. http://www.public.health.wa.gov.au/cproot/4221/2/2010_Annual_STI_BBV_Report.pdf (accessed Nov 2011).
- Workowski KA, Berman S; Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2010. MMWR Recomm Rep 2010; 59: 1-110. 0_i1149886
- Australian Government Department of Health and Ageing. Second national sexually transmissible infections strategy 2010–2013. Canberra: DoHA, 2010. http://www.health.gov. au/internet/main/publishing.nsf/Content/ohp-national-strategies-2010-sti/$File/sti.pdf (accessed Sep 2011).
- Tilson EC, Sanchez V, Ford CL, et al. Barriers to asymptomatic screening and other STD services for adolescents and young adults: focus group discussions. BMC Public Health 2004; 4: 21. 0_i1149890
- Pavlin NL, Gunn JM, Parker R, et al. Implementing chlamydia screening: what do women think? A systematic review of the literature. BMC Public Health 2006; 6: 221. 0_pgfId-1155185
- Rose SB, Smith MC, Lawton BA. “If everyone does it, it’s not a big deal.” Young people talk about chlamydia testing. N Z Med J 2008; 121: 33-42. 0_pgfId-1155192
- Balfe M, Brugha R. What prompts young adults in Ireland to attend health services for STI testing? BMC Public Health 2009; 9: 311. 0_i1149894
- Kong FYS, Guy R, Boyle DJ, et al. Chlamydia testing rates in general practices across Australia: the Australian Collaboration for Chlamydia Enhanced Sentinel Surveillance (ACCESS). Australasian Sexual Health Conference; 2008 Sep 15-17; Perth, Australia. https://secure.ashm.org.au/ei/viewpdf.esp?id=37&file=c%3A%5CCertain%5CEventwin%5Cdocs% 5Cpdf%5Cashm08Abstract00382%2Epdf (accessed Sep 2011).
- Ford CA, Viadro CI, Miller WC. Testing for chlamydial and gonorrhoeal infections outside of clinic settings: a summary of the literature. Sex Transm Dis 2004; 31: 38-51. 0_CHDFCADJ
- Tebb KP, Paukku MH, Pai-Dhungat MR, et al. Home STI testing: the adolescent female’s opinion. J Adolesc Health 2004; 35: 462-467. 0_pgfId-1155274
- van Bergen JE, Postma MJ, Peerbooms PG, et al. Effectiveness and cost-effectiveness of a pharmacy-based screening programme for Chlamydia trachomatis in a high-risk health centre population in Amsterdam using mailed home-collected urine samples. Int J STD AIDS 2004; 15: 797-802. 0_pgfId-1155281
- Novak DP, Karlsoon RB. Simplifying chlamydia testing: an innovative Chlamydia trachomatis testing approach using the internet and a home sampling strategy: population based study. Sex Transm Infect 2006; 82: 142-147. 0_i1149903
- Jones HE, Altini L, de Kock A, et al. Home-based versus clinic-based self-sampling and testing for sexually transmitted infections in Gugulethu, South Africa: randomised controlled trial. Sex Transm Infect 2007; 83: 552-557. 0_pgfId-1155302
- Lippman SA, Jones HE, Luppi CG, et al. Home-based self-sampling and self-testing for sexually transmitted infections: acceptable and feasible alternatives to provider-based screening in low-income women in São Paulo, Brazil. Sex Transm Dis 2007; 34: 421-428. 0_i1149906
- Marrazzo JM, Scholes D. Acceptability of urine-based screening for Chlamydia trachomatis in asymptomatic young men: a systematic review. Sex Transm Dis 2008; 35 (11 Suppl): S28-S33. 0_pgfId-1155317
- Buhrer-Skinner M, Muller R, Bialasiewicz S, et al. The check is in the mail: piloting a novel approach to Chlamydia trachomatis testing using self-collected, mailed specimen. Sex Health 2009; 6: 163-169. 0_i1149909
- Sacks-Davis R, Gold J, Aitken CK, Hellard ME. Home-based testing of young people attending a music festival — who will pee and post? BMC Public Health 2010; 10: 376. 0_i1149911
- Gaydos CA, Dwyer, K, Barnes M, et al. Internet-based screening for Chlamydia trachomatis to reach non-clinic populations with mailed self-administered vaginal swabs. Sex Transm Dis 2006; 33: 451-457. 0_i1149913
- Martin L, Freedman E, Burton L, et al. The C-project: use of self-collection kits to screen for Chlamydia trachomatis in young people in a community-based health promotion project. Sex Health 2009; 6: 157-162. 0_i1149915
- Malik AI, Huppert JS. Interval to treatment of sexually transmitted infections in adolescent females. J Pediatr Adolesc Gynecol 2007; 20: 275-279. 0_i1149917
- Welch J. Follow-up of clients with chlamydia at Clinic 275 in 2001. Adelaide: Royal Adelaide Hospital, 2009. http://www.stdservices.on.net/stats/qsr200203/Follow%20up%20of%20 clinic%20clients%20with%20chlamydia.htm (accessed Nov 2011).
- Smith A, Agius P, Mitchell A, et al. Secondary students and sexual health 2008. Monograph Series No. 70. Melbourne: Australian Research Centre in Sex, Health & Society, La Trobe University, 2009. http://www.latrobe.edu.au/arcshs/downloads/arcshs-research-publications/secondary-students-and-sexual-health-2008.pdf (accessed Oct 2011).
- Huang W, Gaydos CA, Barnes MR, et al. Cost-effectiveness analysis of Chlamydia trachomatis screening via internet-based self-collected swabs compared with clinic-based sample collection. Sex Transm Dis 2011; 38: 815-820. 0_i1149925