





Volume 196 - Issue 9
Sudden limb weakness
Authors: Bill O’Brien, Mark W Parsons and Craig S Anderson
Med J Aust 2012; 196 (9): 572-577. || doi: 10.5694/mja12.10441
Published online: 21 May 2012
Published online: 21 May 2012
Stroke is a common neurological emergency and may occur in patients of all ages. Rapid assessment is crucial for patients with acute neurological symptoms suggestive of stroke because the opportunity for a positive outcome from thrombolytic treatment diminishes rapidly within the first few hours. Although plain non-contrast computed tomography of the brain is ...
Abstract
Stroke is a common neurological emergency and may occur in patients of all ages.
Rapid assessment is crucial for patients with acute neurological symptoms suggestive of stroke because the opportunity for a positive outcome from thrombolytic treatment diminishes rapidly within the first few hours.
Although plain non-contrast computed tomography of the brain is adequate to exclude haemorrhage and conditions such as malignancy, advanced multimodal imaging can be used to assist with decision making regarding the use of recombinant tissue plasminogen activator and mechanical clot-retrieval approaches without adding significant delay.
Excellent outcomes are possible with the early use of reperfusion therapies, even when large areas of brain ischaemia are present, provided that there is evidence of potentially salvageable brain and that treatment can commence without unnecessary delay and hazard.
Catherine’s story
The triage nurse in the emergency department (ED) of a metropolitan hospital contacted the hospital’s acute stroke team at 10 am regarding Catherine, an 82-year-old woman who presented with a “probable stroke” with left-sided symptoms. Catherine was found collapsed on the kitchen floor by her daughter, who had visited at about 9.15 am. According to her daughter, Catherine had been up and doing her usual activities from 7 am and was well when they had spoken on the telephone at 8 am. The electrocardiograph (ECG) monitor in the ambulance had shown Catherine to be in atrial fibrillation (AF) en route to the hospital. Apart from a history of treated hypertension, she had been in good health.
Soon after Catherine arrived at the ED, a rapid neurological examination undertaken by the neurology registrar showed that she was alert and obeying commands, but only with her right side. She was unable to look to the left (right gaze deviation) or appreciate finger movements on the left when presented as bilateral visual stimuli (left hemianopia). There was no movement in her left arm, which flopped back to her side when it was lifted up off the trolley. There was some movement in her left leg, but insufficient strength for her to raise it against gravity. She had reduced appreciation of touch sensation down her whole left side, most obvious in her left arm. The ECG monitor confirmed atrial fibrillation (heart rate, 100 beats/min) and her blood pressure was 180/90 mmHg. Apart from bruising on her left thigh from the fall, results of the rest of the physical examination were normal. This initial clinical assessment took only several minutes to complete.
APPROACH TO THE PROBLEM
Brief focused neurological examination
In Catherine’s case, the history of sudden collapse and left-sided weakness, and associated focal neurological signs, is highly supportive of the diagnosis of acute stroke. However, once the registrar identified right gaze deviation and complete paralysis (“plegia”) of the left arm and obtained a reliable time of onset of within the previous 2 hours, there was little more useful information to be gained from further physical examination that would effectively guide management.
A brief examination that focuses on detecting major neurological deficits enables rapid identification of the location and severity of any stroke. The most widely used structured grading system for assessing the severity of neurological deficit in the setting of acute stroke is the National Institutes of Health Stroke Scale (NIHSS). Assessment using the NIHSS takes less than 2 minutes, requires none of the paraphernalia of a full neurological examination (which is unnecessary in this situation) and is highly predictive of both short-term (in-hospital) and medium-term (at-home) functional outcomes (grade A evidence).1 Skilled use of the NIHSS requires only a few hours of training and accreditation (see http://www.americanheart.org and http://learn.heart.org/ihtml/application/student/interface.heart2/nihss.html). The NIHSS includes a useful grading system for limb paresis that is based on “limb drift”, which overcomes limitations of the traditional UK Medical Research Council grading system for muscle strength (0 for no movement to 5 for normal strength). The NIHSS assessment of limb strength requires the patient to raise an arm or leg off the bed. If he or she can raise it completely off the bed and hold it steady for 10 seconds, limb strength is considered normal and is scored 0. If drift is noticed but the limb can be kept off the bed throughout, a score of 1 is given. If the limb falls to the bed within 10 seconds, a score of 2 is given. Inability to overcome gravity scores 3, and no movement of the limb scores 4. If the patient is unable to adequately obey commands, the observation of spontaneous movement or drift (rapid return to the bed) after the assessor lifts the patient’s limb in the air can allow adequate assessment of motor function.
Appropriate use of investigations
Clinically, Catherine had had a significant stroke and was within the time window for considering thrombolysis, so the next step was an urgent computed tomography (CT) scan to rule out haemorrhage. It is not uncommon to find no acute ischaemic changes on an initial CT scan in patients who have had an acute stroke because visible ischaemic changes usually lag several hours behind what is actually happening in the cerebral tissue. While magnetic resonance imaging can detect early cerebral ischaemia, this is less readily available than CT scanning for urgent cases in hospitals. New software that enables advanced multimodal CT imaging in patients who are being considered for thrombolysis is gaining popularity in assisting clinicians in their decision making regarding the use of thrombolysis (grade C evidence).2,3
After Catherine’s initial clinical assessment, she proceeded to non-contrast CT of her head, which showed no acute ischaemic changes. Perfusion CT (CTP) and CT angiogram (CTA) were then carried out, which confirmed that she had a mid-M1 segment occlusion of the right middle cerebral artery. Despite minimal infarcted cerebral tissue, the whole of the middle cerebral artery territory was at risk (ie, there was an ischaemic penumbra) (Box 1).
PATHOPHYSIOLOGY OF CEREBRAL ISCHAEMIA
Despite significant advances in a range of imaging modalities for investigating the brain and neurovascular tree over recent decades, the diagnosis of acute stroke is largely based on clinical examination, where the goal is to detect features of a sudden onset of focal neurological symptoms and signs of presumed vascular origin. As the anterior circulation has a large region of supply to the cerebral hemispheres, it is most often involved in both ischaemic and haemorrhagic strokes.
Typical features of major strokes include varying degrees and/or combinations of paresis, dysphasia, dysarthria, visual field loss, and disturbance of hemisensory and visuospatial perception. While strokes rarely cause sudden cardiac arrest and death, they can result in an immediate loss of, or rapid deterioration in, a person’s level of consciousness. This can occur because of subarachnoid haemorrhage, mass effect of intracerebral haemorrhage producing cerebral midline or brainstem shift, direct ischaemia of the brainstem (basilar artery occlusion), or generalised seizures triggered by cerebral ischaemia or trauma.
In contrast, minor strokes can be subtle neurological events that may stutter or evolve over hours or days (Box 2). Thus without a history of sudden onset (from the patient or a reliable witness) and/or the presence of atypical, “positive” or inconsistent features, the likelihood of an underlying alternative diagnosis (ie, stroke mimic) is increased (Box 3). In the past, a cut-point of 24 hours was arbitrarily chosen as the duration of neurological symptoms used to separate the diagnosis of transient ischaemic attack from acute stroke in clinical and epidemiological research, but this is no longer clinically significant.
Most strokes (> 80%) are ischaemic and the remainder are due to haemorrhage, which can easily be differentiated on a non-contrast CT scan of the brain. Ischaemic stroke is caused by acute occlusion (clot) of an artery that leads to an immediate reduction in blood flow in the corresponding cerebrovascular territory. The size and site of the occlusion, and the efficiency of compensatory collateral blood flow, determine the extent of impaired blood flow and resulting neurological symptoms from at-risk brain tissue (the ischaemic penumbra [brain tissue that remains potentially salvageable but where blood supply is reduced to a level that unless restored will progress to infarction]) and/or dead brain tissue (the ischaemic core).4
Early spontaneous recanalisation may occur from the normal endogenous release of tissue plasminogen activator (tPA), a serine protease of the fibrinolytic system that converts the zymogen plasminogen into the active protease plasmin, which leads to cleavage of fibrin and dissolving of the newly formed thrombin clot. For most patients, however, and particularly those with large clots, this natural physiological function is inadequate to avoid the outcome of neurological disability from resulting cerebral infarction. Modern management of acute ischaemic stroke is, therefore, aimed at intervening as early as possible after symptom onset to facilitate rapid vessel recanalisation and reperfusion to preserve cerebral function and promote a good outcome.
MANAGEMENT
Acute stroke can be treated rapidly and effectively in an ED with the basic clinical skills that all physicians have. This case highlights the crux of acute intervention in ischaemic stroke — reperfusion of the ischaemic penumbra.5 Intravenous recombinant tissue plasminogen activator (rtPA) is the only treatment licensed by the TGA for treatment of ischaemic stroke, and in a substantial number of patients will result in effective dissolution of the clot.
Current imaging guidelines rely on non-contrast CT but advances in technology are now at a point where a more accurate assessment can be made with multimodal imaging. Treatment is effective but it has limitations (less than 30% of patients with proximal occlusions [eg, terminal internal carotid or origin middle cerebral artery] will have successful dissolution of the clot). As more powerful thrombolytics become available and intra-arterial approaches gain a foothold, patient outcomes will undoubtedly be advanced further.
Thrombolytic treatment
There is compelling evidence to support the routine use of intravenous rtPA in patients with acute ischaemic stroke when carried out in experienced centres with adequate expertise available (grade A evidence).6
While the role of rtPA in acute ischaemic stroke has been debated, particularly within the emergency medicine community, current guidelines from the National Stroke Foundation (which are endorsed by the Australasian College for Emergency Medicine) and licensing by the Therapeutic Goods Administration reflect the evidence for use of rtPA up to 4.5 hours after symptom onset.7 Given that the chance of benefit is greatest when rtPA is used early, because ischaemia causes at-risk brain tissue to rapidly progress to irreversible infarction, the “time is brain” motto is most pertinent in defining systems of care for assessing patients who are potentially eligible for thrombolytic treatment. With a rapid chain of referral, thrombolysis rates of over 20% can be achieved (grade C evidence).8 Although there are risks of bleeding associated with rtPA, the most serious of which is intracerebral haemorrhage that is large enough to produce neurological deterioration, the risks and benefits, when given within the current time window, favours treatment, and this translates into one fewer patient dead or dependent for every 10 patients treated.6 Although the patient characteristics that predict the least to gain or the greatest hazard from rtPA have not been adequately defined, rtPA should be used with caution in certain situations (grade C evidence) (Box 4). It is clear that the benefit of rtPA is very much dependent on there being a clear time of onset of symptoms. This is not possible in up to one-fifth of patients. If a patient cannot provide a reliable history, then the onset of the stroke must be taken as the time when he or she was last seen well. This can be particularly challenging when the patient’s symptoms are present on waking (“wake-up stroke”), in which case the onset time must be taken as when he or she was last known to be well before going to sleep.
While inclusion and exclusion screening questionnaires are readily available for patients who are being considered for thrombolysis, the main practical issue of interest is an assessment of the risk of haemorrhage.7 Although blood tests, including tests of coagulation profile, are routinely undertaken for patients who have had a stroke, the results are usually normal in those who have previously been well and should not hold up the administration of rtPA (grade B evidence). However, in patients on warfarin therapy, rtPA should be avoided or used with caution if the international normalised ratio is above 1.7.7
Further history-taking
Premorbid functioning is an important aspect of enquiry in older patients, as the balance of benefits and risks of thrombolysis is not as well defined in older patients as it is in younger adults. As such, clinicians can be presented with an ethical dilemma over the appropriate use of thrombolysis — a complex and risky treatment — in those older than 80 years.9 A global assessment of premorbid functioning can be made with specific enquiry regarding the patient’s ability to manage daily affairs, such as whether he or she is able to do his or her own shopping. Another useful guide of function is how long a family member would be prepared to leave the person on their own — for example, during the day or overnight. Age alone does not preclude the use (and potential benefits) of thrombolysis but an accurate assessment of premorbid functioning helps guide decision making (grade B evidence).7 As a general rule, patients of any age who have had a large “completed” stroke with large area of cerebral infarction before treatment do poorly irrespective of treatment.
When the neurology registrar enquired about Catherine’s premorbid functioning, her daughter described her as being independent in all daily activities, including shopping, and cognitively sharp without memory problems.
On review of Catherine’s eligibility for rtPA, she was found to be in AF, which had not been previously diagnosed. (Undiagnosed AF is not uncommon in patients who have had a stroke, because AF is often asymptomatic and intermittent before becoming persistent, with common triggers including alcohol intake, acute illness and obstructive sleep apnoea.) She had not been taking any antithrombotic treatment and had no history of bleeding. Her blood pressure was less than 185/110 mmHg (the cut-off for treatment with rtPA).
A frank discussion with Catherine and her daughter involved outlining the benefits and risks of thrombolysis, including the potential for symptomatic haemorrhage. Based on the additional information gained from advanced CT imaging, it was very likely that Catherine would develop major infarction and have significant long-term disability if rapid recanalisation and perfusion of the at-risk cerebral hemisphere did not occur. Catherine and her daughter agreed to proceed with the recommended decision of intravenous rtPA treatment, which was given as per the standard protocol (0.9 mg/kg total dose; 10% bolus and the remainder by infusion over 1 hour).
Catherine was transferred to the hospital’s stroke unit for close monitoring of her vital and neurological signs over the next 24 hours. Two hours after completion of the rtPA infusion, a transcranial colour doppler ultrasound showed return of normal flow in the right middle cerebral artery. She could look to the left and had antigravity movement in her left arm and leg.
A “Lazarus-like” response such as this occurs in about one in 10 rtPA-treated patients; it results from there being minimal early infarction before treatment combined with early reperfusion of a large region of ischaemic brain. Thus, in the presence of a pattern of small infarct core and large ischaemic penumbra on advanced CT imaging (or magnetic resonance imaging), the Lazarus effect is quite common, although it is dependent on the rtPA being successful in rapidly dissolving the occlusive clot (grade C evidence).10
On review the next day, Catherine had no focal neurological deficit, and complete reperfusion and minimal infarction were shown on MRI (Box 1). She was commenced on long-term warfarin therapy. She was reviewed by allied health staff to check on her cognition, mobility and self-care activities, to ensure that it was safe for her to be discharged home. On Day 5, she was back to her premorbid level of functioning and was discharged.
Five weeks later, Catherine was followed up in an outpatient stroke clinic. She had maintained an adequate level of anticoagulation according to weekly testing.
Other interventions
Other proven interventions in the management of acute stroke include admission to and management in a stroke unit with the associated nursing and allied health expertise and, in patients with ischaemic stroke, commencement of aspirin therapy (100–150 mg daily) within 48 hours of symptom onset (grade A evidence).7 These should be considered for all patients who have had an ischaemic stroke, regardless of whether they are eligible for rtPA.
Follow up
An outpatient stroke clinic allows the opportunity to: undertake outstanding investigations and review the results; check that patients are recovering satisfactorily, adjusting to residual disability, and adhering to lifestyle modifications (particularly cessation of smoking) and secondary stroke prevention strategies; review continuity of follow-up rehabilitation or support services; review communication with the patient’s general practitioner; check that the patient and his or her family have a reasonable understanding of stroke and its aetiology; and check that there are no major complications or comorbid consequences of the stroke event (Box 5).
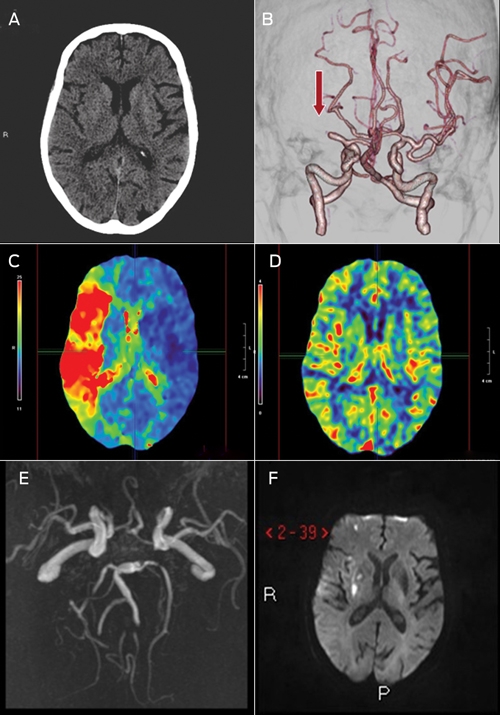
1 Multimodal computed tomography (CT) and magnetic resonance imaging (MRI) images of Catherine’s brain before and after treatment with recombinant tissue plasminogen activator
A: Non-contrast CT showing no acute changes, as is often the case in acute stroke.
B: CT angiogram showing occlusion of the mid-M1 segment of the middle cerebral artery (arrow) with no distal flow.
C: CT perfusion time-to-peak map showing a significant delay in contrast flow (red area) affecting the right hemisphere, indicating that the entire territory is at risk of infarction without timely reperfusion.
D: CT perfusion mean-transit-time map showing that, despite the significant perfusion deficit on the time-to-peak map, cerebral blood flow in the right hemisphere is preserved (with no obvious asymmetry compared with the left hemisphere), which suggests that as yet little hypoperfused tissue has progressed to established infarction.
E: Magnetic resonance angiography 24 hours after treatment showing complete recanalisation of the middle cerebral artery.
F: Diffusion-weighted MRI (a very sensitive measure of acute infarction) 24 hours after treatment showing a few small acute infarcts (high signal in right hemisphere), but essentially complete salvage of the territory that had been at risk.
Perfusion brain imaging (with CT or MRI) involves use of an intravenous contrast bolus followed by serial imaging of the brain over about 1 minute, with tracking of the contrast as it flows through the vascular bed, allowing assessment of cerebral blood flow, cerebral blood volume, time to peak and mean transit time. Delayed contrast transit on time-to-peak or mean-transit-time maps is most often used to identify tissue that is at risk and areas where severely reduced cerebral blood volume (or blood flow) represents irreversibly injured tissue.
2 Minor stroke syndromes that require particular attention in assessment
3 Common stroke and transient ischaemic attack (TIA) mimics, and features that may differentiate them from acute stroke and TIA
4 Situations where intravenous recombinant tissue plasminogen activator should be used with caution
Large area of infarction on initial non-contrast computed tomography scan, indicating that time since onset is likely to be > 4.5 hours
Evidence of proximal vessel (terminal internal carotid [“carotid T”]) occlusion — in which case the patient may benefit from mechanical clot extraction procedures
Patient is older than 80 years
Patient is taking warfarin and has an international normalised ratio > 1.7, or is taking other therapeutic anticoagulants
Significant trauma from fall at time of stroke onset
5 Aspects of stroke that should be reviewed at a follow-up clinic
Competing interests
No relevant disclosures.
References
- Kasner SE. Clinical interpretation and use of stroke scales. Lancet Neurol 2006; 5: 603-612. 0_i1140747
- Muir KW, Buchan A, von Kummer R, et al. Imaging of acute stroke. Lancet Neurol 2006; 5: 755-768. 0_i1140749
- Parsons MW. Perfusion CT: is it clinically useful? Int J Stroke 2008; 3: 41-50. 0_i1140751
- Donnan GA, Fisher M, Macleod M, Davis SM. Stroke. Lancet 2008; 371: 1612-1623. 0_i1140753
- Rha JH, Saver JL. The impact of recanalization on ischemic stroke outcome: a meta-analysis. Stroke 2007; 38: 967-973. 0_i1140756
- Lees KR, Bluhmki E, von Kummer R, et al. Time to treatment with intravenous alteplase and outcome in stroke: an updated pooled analysis of ECASS, ATLANTIS, NINDS, and EPITHET trials. Lancet 2010; 375: 1695-1703. 0_i1140758
- National Stroke Foundation. Clinical guidelines for stroke management 2010. Melbourne: NSF, 2010. http://www.strokefoundation.com.au/news/welcome/clinical-guidelines-for-acute-stroke-management (accessed Apr 2012).
- Quain DA, Parsons MW, Loudfoot AR, et al. Improving access to acute stroke therapies: a controlled trial of organised pre-hospital and emergency care. Med J Aust 2008; 189: 429-433. 0_i1140763
- Mishra NK, Ahmed N, Andersen G, et al. Thrombolysis in very elderly people: controlled comparison of SITS International Stroke Thrombolysis Registry and Virtual International Stroke Trials Archive. BMJ 2010; 341: c6046. 0_i1140765
- Parsons M, Spratt N, Bivard A, et al. A randomized trial of tenecteplase versus alteplase for acute ischemic stroke. N Engl J Med 2012; 366: 1099-1107. 0_i1140767
Provenance: Commissioned; externally peer reviewed.