




Coronary atherosclerosis is a major cause of morbidity and mortality. On diagnosis, all patients require appropriate lifestyle modification and lifelong drug therapy with aspirin, statins, and angiotensin-converting enzyme inhibitors plus β-blockers if their heart has been damaged. Instituting these measures is estimated to reduce adverse cardiovascular events by 75%–80% over a 5-year period.1 Revascularisation by percutaneous coronary intervention (PCI) or coronary artery bypass graft surgery plays an important role, but it is a double-edged sword. In the presence of significant myocardial ischaemia, revascularisation reduces symptoms2,3 and improves prognosis,4-6 but in its absence revascularisation worsens outcomes, even when the coronary lesion in question may have a diameter stenosis of 70% or greater.7,8
In Australia, as in other countries,9 most coronary lesions are revascularised on the basis of their angiographic characteristics, often without knowledge of whether the lesion is causing ischaemia or not. As such, many coronary lesions that are not physiologically significant are unnecessarily stented or bypassed, at considerable expense to the health system and to the detriment of the patient. Fortunately, new technology, namely computed tomography coronary angiography (CTCA) and measurement of coronary fractional flow reserve (FFR), if correctly applied, enables more accurate assessment of coronary anatomy and function and has the potential to substantially improve outcomes and lower costs. Here, we present and discuss a simple algorithm (Box 1) for the management of stable coronary artery disease (CAD) using this new technology.
The presence of coronary atherosclerosis can be assumed if the patient has presented with a proven acute coronary syndrome or has evidence of atherosclerosis elsewhere. In other circumstances, such as symptomatic patients or patients with multiple risk factors in whom CAD is suspected but not proven, diagnosis is less straightforward. The most reliable diagnostic test is a 64-slice (or higher) CTCA scan, which excludes significant CAD with a sensitivity and negative predictive value in excess of 96%.10 Atherosclerosis is predominantly a disease of the arterial wall, which may encroach on the vessel lumen over time. CTCA provides accurate information about the state of both the arterial wall and the lumen. A normal CTCA scan effectively excludes coronary atherosclerosis and portends an extremely low likelihood of coronary events over at least the next 5 years.11 If the CTCA scan shows atherosclerosis, but no luminal stenosis of greater than 50%, medical treatment (as described above) should be initiated. If the CTCA scan shows lesions of 50% or greater severity, then further testing for ischaemia may be appropriate (Box 1).
Coronary atherosclerosis cannot be cured and requires lifelong medical therapy. Once a diagnosis has been made, the only continuing diagnostic issue is that of myocardial ischaemia, for which CTCA is not the appropriate test.12 Therefore, subsequent CTCA scans, which are expensive ($500) and carry a radiation burden (although less than that of nuclear stress testing and invasive angiography13), are not indicated.
The presence of myocardial ischaemia can be assumed if a patient with known CAD has typical angina. In other cases, stress testing is the standard non-invasive means of diagnosing ischaemia. Irrespective of the type of stress test (standard electrocardiogram [ECG], nuclear stress test or echo stress test) used, a negative test result at a satisfactory workload effectively excludes any myocardial ischaemia significant enough to warrant intervention, and obviates the need for invasive angiography. Depending on the clinical circumstances, a positive test result is an indication for further investigation with invasive angiography (Box 1).
In most circumstances, the less expensive ECG exercise test (cost, $144) is adequate screening for this purpose,14 but in patients with a resting ECG abnormality or those unable to exercise, nuclear (cost, $984) or echo (cost, $406) stress tests are a more accurate means of assessing ischaemia. Both these tests have the additional advantage of localising the area of ischaemia; however, this attribute is now of limited value because FFR7,15 offers a more precise means of achieving this, particularly in multivessel CAD.16-18 Nuclear and echo stress tests provide comparable information with respect to myocardial ischaemia, but nuclear stress tests are more expensive and carry a significant radiation burden,13 and should therefore no longer be used for this purpose.
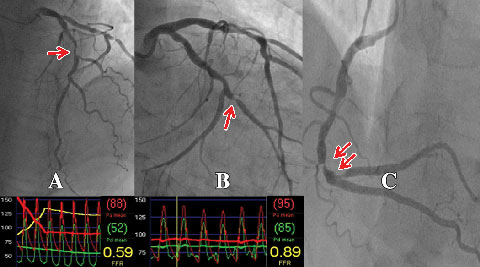
An important recent advance has been the ability to accurately determine the physiological significance of an individual coronary lesion by measuring FFR.7,15 FFR is defined as the ratio between coronary pressure distal to the stenosis in question and aortic pressure measured simultaneously during adenosine-induced hyperaemia. Coronary pressure is obtained by passing a pressure guide wire distal to the coronary stenosis in a manner analogous to passing a guide wire for the purpose of PCI.7,15 As such, it can be easily and safely performed by those experienced in performing PCI. If PCI is indicated as a result of the FFR measurement, the coronary pressure wire can be used for stent delivery. In the case of multiple lesions in one or more vessels, each individual lesion can be examined by the pressure wire (Box 2). In this way, the lesion or lesions causing ischaemia can be determined in a more precise manner than the traditional method of correlating the angiographic findings with the results of stress testing, or by using angiographic criteria alone.
A wealth of data has validated the accuracy of FFR as a measure of myocardial ischaemia.7,15,19 An FFR value of ≤ 0.80 identifies ischaemia-causing coronary stenoses with an accuracy of greater than 90%. An FFR > 0.80 excludes ischaemia with a predictive accuracy of 95%.15
Several important studies have conclusively demonstrated the clinical utility of FFR in decision making concerning PCI.7,20 The FAME (Fractional Flow Reserve Versus Angiography for Multivessel Evaluation) study demonstrated that FFR guidance of coronary artery stenting in patients with multivessel disease resulted in a significantly lower rate of adverse events than traditional angiography-guided PCI. In the FAME study, 1005 patients with multivessel CAD were randomly assigned to undergo PCI guided by angiography alone or with the addition of FFR measurements.7 Before randomisation, lesions thought to require PCI were identified based on their angiographic appearance. Patients randomly assigned to the angiography-guided PCI group underwent stenting of all indicated lesions, whereas those randomly assigned to FFR-guided PCI underwent stenting of indicated lesions only if the FFR was ≤ 0.80. The results are shown in Box 3 and demonstrate that, in this representative group of patients, the use of FFR resulted in significantly improved outcomes at significantly lower costs.21
An important observation in the FAME study was that 65% of lesions judged on angiographic criteria to be between 50% and 70% in severity, and 20% of lesions between 71% and 90% in severity were not physiologically significant based on FFR criteria.22 These angiographically but not physiologically significant lesions accounted for 36% of stented lesions in the angiographic arm of the FAME study.22 Extrapolation of these data leads to the conclusion that more than a third of elective stenting in stable multivessel CAD is unnecessary, potentially harmful and costly to the health system.
In light of the results of the FAME study, patients with stable CAD should undergo coronary angiography with a view to FFR-guided revascularisation if they are found to have significant myocardial ischaemia (Box 1). Angiographic lesions of > 90% severity can be assumed to be ischaemia-generating and can be appropriately revascularised without resort to FFR.22 Likewise, a single lesion in a single vessel with ischaemia demonstrated by stress testing can be appropriately stented without measurement of FFR. It is likely that these two circumstances account for less than 25% of cases. All other coronary lesions should be stented or bypassed only if the FFR is ≤ 0.80.
Coronary pressure wires to measure FFR have been available in Australia for over 5 years but, according to Medicare statistics, are used in < 5% of cases.23 There are several reasons for this low uptake. The cost of a pressure wire is $1300, compared with $300 for a standard wire. In the public system, where there is no separate diagnosis-related group for procedures involving the pressure wire, casemix funding discourages the use of more expensive equipment, even when the use of that equipment may save money in the long term. In the private system, health insurance companies either do not or only partially cover the cost of the pressure wire. Thus, although the use of a pressure wire saves substantial amounts of money, the method of reimbursement in both the public and private systems militates against its use.
Implementation of the management strategy outlined in Box 1 would result in more CTCA scans, but the additional expense related to this would be minor in comparison to the savings that would be achieved if the measures listed in Box 4 were to be adopted. Furthermore, by eliminating nuclear stress tests, “diagnostic” coronary angiography and unnecessary stenting, patient outcomes would be improved and radiation burden reduced. The pros and cons of this approach are summarised in Box 5.
Changes to the health system that would facilitate a more evidence-based and cost-effective approach to the management of stable CAD are listed in Box 6. These changes are likely to be opposed by nuclear physicians and sections of the cardiology community. Nevertheless, in our opinion, instituting these changes would undoubtedly result in improved outcomes and substantial savings.
4 Measures that would reduce costs
Confining stress tests to the diagnosis of myocardial ischaemia in known coronary artery disease (CAD)
Greater reliance on the standard electrocardiogram stress test
Replacement of nuclear stress tests with stress echocardiography
Elimination of “diagnostic” invasive coronary angiography
Routine use of fractional flow reserve measurement in multilesion CAD to avoid unnecessary stenting
5 Pros and cons of the proposed management strategy
6 Suggested changes to the health system
The Medicare item number for nuclear stress tests should be abolished
There should be a Medicare item number for computed tomography coronary angiography, but this should only be applicable to an individual with no known coronary artery disease and only once every 5 years
Use of the Medicare item number for coronary angiography should be confined to accredited interventional cardiologists
There should be separate diagnosis-related groups and Medicare item numbers for coronary angiography with the use of a pressure wire and percutaneous coronary intervention (PCI) with the use of a pressure wire
Hospitals and cardiologists performing PCIs should be accredited to do so, with continuing accreditation based on robust quality assurance programs
- Richard W Harper1
- Brian S Ko2
- MonashHeart, Southern Health, Monash Medical Centre, Melbourne, VIC.
None identified.
- 1. Yusuf S, Natarajan M, Karthikeyan G, Taggart D. Management of stable angina. BMJ 2009; 339: b2789.
- 2. Rita-2 trial participants. Coronary angioplasty versus medical therapy for angina: the second Randomised Intervention Treatment of Angina (RITA-2) trial. Lancet 1997; 350: 461-468.
- 3. Fihn SD, Williams SV, Daley J, et al. Guidlines for the management of patients with chronic stable angina: treatment. Ann Intern Med 2001; 135: 616-632.
- 4. Erne P, Schoenenberger AW, Burckhardt D, et al. Effects of percutaneous coronary interventions in silent ischemia after myocardial infarction: the SWISSI II randomized controlled trial. JAMA 2007; 297: 1985-1991.
- 5. Shaw LJ, Berman DS, Maron DJ, et al. Optimal medical therapy with or without percutaneous coronary intervention to reduce ischemic burden: results from the Clinical Outcomes Utilizing Revascularization and Aggressive Drug Evaluation (COURAGE) trial nuclear substudy. Circulation 2008; 117: 1283-1291.
- 6. Yusuf S, Zucker D, Peduzzi P, et al. Effect of coronary artery bypass graft surgery on survival: overview of 10-year results from randomized trials by the Coronary Artery Bypass Graft Surgery Trialists Collaboration. Lancet 1994; 344: 563-570.
- 7. Tonino PA, De Bruyne B, Pijls NH, et al; FAME Study Investigators. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention. N Engl J Med 2009; 360: 213-224.
- 8. Botman CJ, Schonberger J, Koolen S, et al. Does stenosis severity of native vessels influence bypass graft patency? A prospective fractional flow reserve-guided study. Ann Thorac Surg 2007; 83: 2093-2097.
- 9. Boden WE, O’Rourke RA, Teo KK, et al. Optimal medical therapy with or without PCI for stable coronary disease. N Engl J Med 2007; 356: 1503-1516.
- 10. Vanhoenacker PK, Heijenbrok-Kal MH, Van Heste R, et al. Diagnostic perfomance of multidetector CT angiography for assessment of coronary artery disease: meta-analysis. Radiology 2007; 244: 419-428.
- 11. Russo V, Zavalloni A, Bacchi Reggiani ML, et al. Incremental prognostic value of coronary CT angiography in patients with suspected coronary artery disease. Circ Cardiovasc Imaging 2010; 3: 351-359.
- 12. Meijboom WB, Van Mieghem CA, van Pelt N, et al. Comprehensive assessment of coronary artery stenoses: computed tomography coronary angiography versus conventional coronary angiography and correlation with fractional flow reserve in patients with stable angina. J Am Coll Cardiol 2008; 52: 636-643.
- 13. Fazel R, Krumholz HM, Wang Y, et al. Exposure to low-dose ionizing radiation from medical imaging procedures. N Engl J Med 2009; 361: 849-857.
- 14. Weiner DA, Ryan TJ, McCabe CH, et al. Prognostic importance of a clinical profile and exercise test in medically treated patients with coronary artery disease. J Am Coll Cardiol 1984; 3: 772-779.
- 15. Kern MJ, Samady H. Current concepts of integrated coronary physiology in the catheterization laboratory. J Am Coll Cardiol 2010; 55: 173-185.
- 16. Ragosta M, Bishop AH, Lipson LC, et al. A comparison between angiography and fractional flow reserve versus single-photon emission computed tomographic myocardial perfusion imaging for determining lesion significance in patients with multivessel coronary disease. Am J Cardiol 2007; 99: 896-902.
- 17. Melikian N, De Bondt P, Tonino P, et al. Fractional flow reserve and myocardial perfusion imaging in patients with angiographic multivessel coronary artery disease. JACC Cardiovasc Interv 2010; 3: 307-314.
- 18. Rieber R, Jung P, Erhard I, et al. Comparison of pressure measurement, dobutamine contrast stress echocardiography and SPECT for the evaluation of intermediate coronary stenoses. The COMPRESS trial. Int J Cardiovasc Intervent 2004; 6: 142-147.
- 19. Pijls NH, De Bruyne B, Peels K, et al. Measurement of fractional flow reserve to assess the functional severity of coronary-artery stenoses. N Engl J Med 1996; 334: 1703-1708.
- 20. Pijls NH, van Schaardenburgh P, Manoharan G, et al. Percutaneous coronary intervention of functionally nonsignificant stenosis: 5-year follow-up of the DEFER Study. J Am Coll Cardiol 2007; 49: 2105-2111.
- 21. Pijls NH, Fearon WF, Tonino PA, et al. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention in patients with multivessel coronary artery disease: 2-year follow-up of the FAME (Fractional Flow Reserve Versus Angiography for Multivessel Evaluation) study. J Am Coll Cardiol 2010; 56: 177-184.
- 22. Tonino PA, Fearon WF, De Bruyne B, et al. Angiographic versus functional severity of coronary artery stenoses in the FAME study: Fractional Flow Reserve Versus Angiography in Multivessel Evaluation. J Am Coll Cardiol 2010; 55: 2816-2821.
- 23. Medicare Australia. MBS item statistics reports. https://www.medicareaustralia.gov.au/statistics/mbs_item.shtml (accessed Dec 2010).
Abstract
Revascularisation, either by stenting or bypass grafts, is commonly performed in patients with stable coronary artery disease but is a double-edged sword. In the presence of ischaemia, revascularisation improves outcomes; in its absence, outcomes are worsened.
In current practice, the decision of whether to revascularise is mainly made on the basis of the angiographic appearance of the coronary lesion in question. Physiological assessment of coronary lesions by the use of a pressure wire and measurement of fractional flow reserve (FFR) often shows that lesions thought to be sufficiently severe to warrant stenting or bypass do not cause ischaemia.
A recent randomised study has shown that using FFR measurements to guide coronary stenting resulted in a lower use of stents, decreased costs and superior outcomes at 2 years, compared with traditional angiographic assessment alone.
We believe that changes to the methods of health reimbursement are needed in both the public and private health systems, to facilitate greater use of FFR measurement.