





Volume 193 - Issue 5
Brain abnormalities detected on magnetic resonance imaging of amphetamine users presenting to an emergency department: a pilot study
Authors: Daniel M Fatovich, David L McCoubrie, Swithin J Song, David M Rosen, Nick D Lawn and Frank F Daly
Med J Aust 2010; 193 (5): 266-268. || doi: 10.5694/j.1326-5377.2010.tb03904.x
Published online: 6 September 2010
Published online: 6 September 2010
Abstract
Objectives: To determine the prevalence of occult brain abnormalities in magnetic resonance imaging of active amphetamine users.
Design, setting and participants: Prospective convenience study in a tertiary hospital emergency department (ED). Patients presenting to the ED for an amphetamine-related reason were eligible for inclusion. We collected demographic data, drug use data, and performed a mini-mental state examination (MMSE).
Main outcome measures: The proportion of patients with an abnormality on their MRI scan.
Results: Of 38 patients enrolled, 30 had MRI scans. Nineteen were male and their mean age was 26.7 ± 5.4 years (range 19–41 years). The mean age of first amphetamine use was 18 years (range 13–26 years). Sixteen patients used crystal methamphetamine (mean amount 2.5 g/week), nine used amphetamine (“speed”) (mean amount 2.9 g/week), and 23 used ecstasy (mean amount 2.3 tablets/week). Marijuana was smoked by 26 (mean amount 5.9 g/week), and 28 drank alcohol (mean amount 207 g/week). The median MMSE score was 27/30 (interquartile range, 26–29). Abnormalities on brain MRI scans were identified in six patients, most commonly an unidentified bright object (n = 4).
Conclusion: In this pilot study of brain MRI of young people attending the ED with an amphetamine-related presentation, one in five had an occult brain lesion. While the significance of this is uncertain, it is congruent with evidence that amphetamines cause brain injury.
Methamphetamine (MA) is a highly addictive substance that has caused serious public health problems globally.1,2 Recent population surveys report that 16% of people in the 20–29-year age group have used amphetamines.3 Of particular concern is emerging evidence of serious long-term effects of amphetamine use, including depression, anxiety, psychosis and memory disturbance.4
Neuroimaging studies demonstrate abnormalities in abstinent MA users.5-8 The aim of this study was to determine the prevalence of clinically occult cerebral abnormalities in active amphetamine users presenting to our emergency department (ED).9
Methods
This was a prospective convenience observational pilot study conducted in the ED at the Royal Perth Hospital (RPH), Western Australia, from 9 April 2008 to 27 July 2009. Patients with an amphetamine-related presentation were eligible for inclusion.
Exclusion criteria included lack of suitability to undergo a magnetic resonance imaging (MRI) scan, and psychosis in patients detained under the Mental Health Act 1996 (WA).
All patients received standard clinical management and a mini-mental state examination (MMSE) was performed.10 Detailed data on their drug use were collected. When possible, an MRI was performed during the time of patients’ attendance in the ED, or shortly after discharge. Any patient who was identified on MRI as having an abnormality was referred to the RPH neurology service for assessment.
The MRI scans were performed on a Siemens Sonata 1.5T MRI scanner (Siemens Medical Systems, Erlangen, Germany). The following sequences were undertaken: axial proton density; T2 fast spin echo; fluid attenuated inversion recovery (FLAIR); diffusion weighted imaging; sagittal FLAIR; three-dimensional magnetisation-prepared rapid acquisition with gradient echo; and a three-dimensional time-of-flight magnetic resonance angiography of the circle of Willis. The radiologist was not blinded to which patients were participating in the study.
We aimed to screen 30 patients in this pilot study. Also, we arbitrarily categorised the patients into two patterns of drug use: serious (injecting, snorting or smoking MA and other illicit drugs) or recreational (oral use only, including ecstasy, marijuana and alcohol).
Data were recorded onto an Excel database and analysed using SPSS version 17 (SPSS Inc, Chicago, Ill, USA). Descriptive statistics were used to describe the cohort.
The study was approved by the RPH Ethics Committee, and all participants gave written informed consent.
Results
Thirty-eight patients were enrolled, and 30 had MRI scans. Of these 30 patients, 19 were male, and their mean age was 26.7 years (SD, 5.4 years; range 19–41). The median time from last amphetamine use to ED attendance was 13.6 hours (interquartile range [IQR], 5.8–33.2), and the median time from last use to MRI scan was 2.8 days (IQR, 1.8–4.9). Nineteen patients required admission to hospital. Clinical presentations of the 30 patients who had MRI scans are shown in Box 1.
The demographic profile, clinical characteristics and drug-use history of the eight patients who did not have an MRI scan were similar to those who did have a scan.
The mean age at which the 30 patients who did have an MRI scan first started to use amphetamines was 18.0 years (SD, 3.1 years; range 13–26). Twenty-three were classified as serious drug users, and the remainder as recreational users. Box 2 shows a detailed history of their drug use. Other drugs used included cocaine (n = 6), heroin (n = 5), lysergic acid diethylamide (LSD; “acid”) (n = 5) and hallucinogenic mushrooms (n = 1). Twenty-five patients were cigarette smokers (mean usage was 21 cigarettes/day for 11 years), and two were ex-smokers.
Twenty-one patients reported problems with their mood, 19 reported problems with their concentration, 15 with their general health, and 14 reported memory problems. Nine reported having been admitted to a psychiatric hospital, 14 reported a history of depression, and seven reported a history of psychosis. Six patients had been prisoners in jail.
Twenty-one patients required sedation for agitation in the ED, most commonly with benzodiazepines. The median time from last amphetamine use to interview was 27 hours (IQR, 11–60 hours), and the median time from last sedative dose to interview was 2 hours (IQR, 0–9 hours). The median MMSE score was 27/30 points (IQR, 26–29). The most common deficits were seen in the questions on orientation, attention and calculation, recall and language. Conditions in patients’ medical histories that might be associated with abnormalities seen on MRI scans, such as migraine, were similar in those with and without abnormalities.
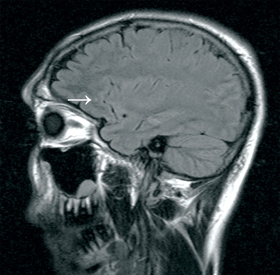
Six patients had abnormalities showing on their MRI scan. Four of these six were male, with a median age of 29 years. The most common MRI abnormality seen (n = 4) was an unidentified bright object (UBO). This is a T2 hyperintensity in subcortical white matter, without a corresponding diffusion-weighted imaging abnormality. Three of the four UBOs seen were in the frontal lobes (Box 3). One patient had cortical atrophy, and one had hippocampal oedema and sclerosis.11 Five of the 23 serious users had abnormalities showing on their MRI scans.
Discussion
In our pilot study we found that one in five patients had abnormality on their MRI brain scan, the most common being a UBO. Katzman reported only five UBOs as incidental findings in 1000 asymptomatic volunteers (mean age 30.6 years).12 Most UBOs in our study were in the frontal region of the brain; this finding is consistent with reports of frontal abnormalities in MA users.5,13 Whether or not these UBOs are associated with long-term clinical effects is unknown, but our finding supports the possibility of amphetamine use being a risk for cognitive decline, and perhaps an increased risk of stroke.
The main limitations of our study are the small sample size, a patient group for whom reliable follow-up was not possible, with no age-matched controls, and the difficult type of research (in that it is difficult to attribute causation in users of multiple drugs). Many of our patients are chaotic, poly-drug users who access whatever is available, so other drugs could be contributing to the changes seen on MRI. Reporting bias is possible and minor abnormalities in MMSE scores are likely to have been influenced by the acute effects of intoxication, and, for some, the effects of sedation.
In this pilot study of MRI brain scans of young people attending the ED for amphetamine-related reasons, one in five had an occult brain lesion suggesting injury. While the significance of this is uncertain, it is congruent with evidence that amphetamines cause brain injury, and therefore could have public health implications.
1 Clinical presentations of the 30 patients who had magnetic resonance imaging scans after using amphetamines
Competing interests
The RPH Medical Research Foundation funded the MRI scans.
Acknowledgements
This study was supported by a grant from the RPH Medical Research Foundation. We are grateful for the support of the MRI team.
References
- Gunter TD. Control of methamphetamine misuse. BMJ 2007; 334: 1176-1177. 0_i1095629
- United Nations Office on Drugs and Crime. World Drug Report 2009. New York, 2009. http://www.unodc.org/unodc/en/data-and-analysis/WDR-2009.html (accessed Jul 2010).
- Australian Institute of Health and Welfare. 2007 National Drug Strategy Household Survey. Canberra, AIHW: 2008. http://www.aihw.gov.au/publications/index.cfm/title/10579 (accessed Jul 2010).
- Meredith CW, Jaffe C, Ang-Lee K, Saxon AJ. Implications of chronic methamphetamine use: a literature review. Harv Rev Psychiatry 2005; 13: 141-154. 0_i1095635
- Berman S, O’Neill J, Fears S, et al. Abuse of amphetamines and structural abnormalities in the brain. Ann N Y Acad Sci 2008; 1141: 195-220. 0_i1095637
- Chang L, Alicata D, Ernst T, Volkow N. Structural and metabolic brain changes in the striatum associated with methamphetamine abuse. Addiction 2007; 102: 16-32. 0_pgfId-1100063
- Ernst T, Chang L, Leonido-Yee M, Speck O. Evidence for long-term neurotoxicity associated with methamphetamine abuse: A 1H MRS study. Neurology 2000; 54: 1344-1349. 0_pgfId-1100070
- Thompson PM, Hayashi KM, Simon SL, et al. Structural abnormalities in the brains of human subjects who use methamphetamine. J Neurosci 2004; 24: 6028-6036. 0_i1095641
- Gray SD, Fatovich DM, McCoubrie DL, Daly FF. Amphetamine-related presentations to an inner-city tertiary emergency department: a prospective evaluation. Med J Aust 2007; 186: 336-339. 0_i1095643
- Dick JP, Guiloff RJ, Stewart A, et al. Mini-mental state examination in neurological patients. J Neurol Neurosurg Psychiatry 1984; 47: 496-499. 0_i1095645
- Gardner H, Lawn N, Fatovich DM, Archer JS. Acute hippocampal sclerosis following ecstasy ingestion. Neurology 2009; 73: 567-569. 0_i1095647
- Katzman GL, Dagher AP, Patronas NJ. Incidental findings on brain magnetic resonance imaging from 1000 asymptomatic volunteers. JAMA 1999; 282: 36-39. 0_i1095649
- Bae SC, Lyoo IK, Sung YH, et al. Increased white matter hyperintensities in male methamphetamine abusers. Drug Alcohol Depend 2006; 81: 83-88. 0_i1095652