





Volume 192 - Issue 12
Acute abducens nerve palsy and weight loss due to skull base osteomyelitis
Authors: Jenson C S Mak, Lawrence H Kim, Lawrence T C Ong and Triet M Bui
Med J Aust 2010; 192 (12): 719-720. || doi: 10.5694/j.1326-5377.2010.tb03713.x
Published online: 21 June 2010
Published online: 21 June 2010
A 90-year-old man presented to the emergency department with multiple symptoms including double vision, reduced mobility, dysphagia, recent rapid weight loss, ear discharge and deafness. He had diabetes and other chronic medical problems, including otitis media with mastoiditis. This case highlights the difficulty of investigating weight loss in older people, who may not show the usual clinical features of infection, and of distinguishing between infection and malignancy when radiological findings are inconclusive. His eventual diagnosis was osteomyelitis of the skull base with cranial nerve involvement.
Clinical record
A 90-year-old, previously fit Estonian man was admitted to hospital from the emergency department (ED) with multiple symptoms including acute diplopia, difficulty with walking, several falls over 2 weeks, decreased taste sensation, dysphagia with solids over several months, a 10 kg weight loss over 5 months, and a 6-week history of otalgia, aural fullness, otorrhea, and deafness. Four months earlier, the patient had presented to the ED with acute onset of left facial nerve palsy, dysphonia and dysphagia. The facial nerve palsy had resolved spontaneously after 2 weeks without specific treatment.
The patient had several significant background medical problems: late-onset diabetes mellitus of 17 years’ duration; peripheral neuropathy; chronic atrial fibrillation; hypertension; and chronic left otitis media with effusion and mastoiditis, for which he had been treated with insertion of a tympanostomy tube 5 months before admission, and a short course of a topical corticosteroid and an oral antibiotic 1 month before admission. The dysphagia was investigated before admission with a barium meal, oesophageal manometry and gastroscopy, which showed severe oesophageal dysmotility and no obstructive lesion. The patient was an ex-smoker with a 55 pack-year smoking history, regular moderate alcohol intake, and occasional salted fish but no areca (or “betel”) nut consumption (which have been linked to nasal and oral cancers, respectively). There was no family history of cancer.
His regular medications included metformin, gliclazide, amiodarone, lercanidipine, frusemide and amitriptyline.
The main findings on examination included failure of abduction (but no medial deviation) of the left eye consistent with abducens nerve palsy, bilateral haemoserous ear discharge, cachexia, and unsteady gait. No other localising neurological signs were found. The patient remained afebrile throughout the admission. A bedside swallowing assessment by a speech pathologist demonstrated moderate pharyngeal dysphagia. Communication with the patient was conducted through writing.
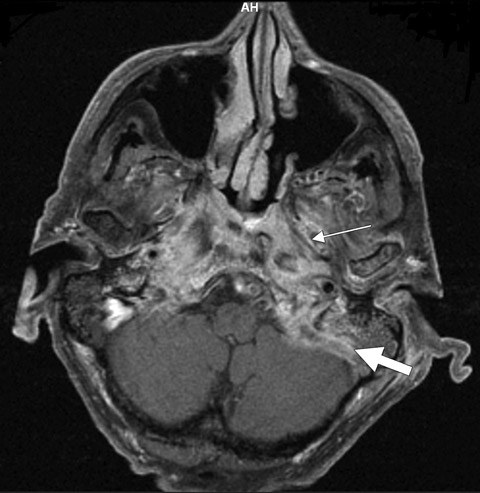
The results of blood tests were unremarkable: his creatinine level was 100 μmol/L (reference range [RR], 70–110 μmol/L); leukocytes, 9.0 × 109/L (RR, 4.0–10.0 × 109/L); glycated haemoglobin, 7.1%; and C-reactive protein (CRP), 51 mg/L (RR, < 5.0 mg/L). One week later, the leukocyte count remained within the normal range and his CRP level had fallen to 35 mg/L, remaining at this level throughout the admission without any specific treatment. A computed tomography (CT) scan and magnetic resonance imaging (MRI) of the brain showed extensive skull base and prevertebral soft tissue thickening with contrast enhancement, bilateral mastoid air cell opacification, and bony destruction of the clivus and both petrous parts of the temporal bones (Box). Bone scintigraphy, performed using technetium-99m hydroxymethane diphosphonate, and a fluorodeoxyglucose positron emission tomography (FDG-PET) scan showed intense tracer uptake in the nasopharynx, base of the skull and mastoid air cells. There was no evidence on the FDG-PET scan of distant uptake. A culture of ear discharge grew a mixture of Staphylococcus aureus and Pseudomonas aeruginosa that were sensitive to flucloxacillin and ciprofloxacin, respectively.
Nasopharyngeal carcinoma was strongly suspected by the treating medical team on the basis of radiological findings, significant weight loss (even though the weight loss could be partially attributed to dysphagia), and only a moderate rise in the CRP level. However, the treating ear, nose and throat (ENT) surgeon was of the strong opinion that the abnormalities were due to an infective process and that nasopharyngeal biopsy was not necessary. In view of the radically different nature of the treatments for the two conditions, the divergent opinions about the diagnosis, and the patient’s family wanting more certainty, the opinion of a second ENT surgeon was sought. Subsequent nasopharyngeal biopsy results showed only submucosal chronic inflammation.
A diagnosis of skull base osteomyelitis complicating otitis media was made. The patient was started on oral ciprofloxacin 500 mg twice a day (to be continued long term), rehabilitated (practice in transfers, ambulation and self-care), and discharged after 31 days, having shown improvements in weight, mobility and other functional status. At 4-month follow-up, diplopia and abducens nerve palsy had resolved, the patient’s CRP level was 0.3 mg/L and he had gained 8 kg in weight. At 7-month follow-up, there was no ear discharge, the patient’s weight was stable, he felt well and had returned to his previous level of activity. Using hearing aids, the patient was able to converse. Cessation of ciprofloxacin would be considered at 1-year follow-up if there were signs of resolution of osteomyelitis on gallium imaging and repeat bone scan and MRI.
Discussion
Osteomyelitis of the base of the skull is commonly associated with malignant otitis externa. However, this patient had chronic otitis media and mastoiditis. Involvement of lower cranial nerves (VI to X) is common in skull base osteomyelitis due to their anatomical proximity to the clivus.1,2 Accurate diagnosis of abnormalities in the base of the skull is important but difficult. Both infection and malignancy can result in severe disability and death, but a good clinical outcome can be achieved with the correct treatment.2 The difficulty of diagnosing either infection or malignancy in similar cases has been reported previously.3-5 However, this patient’s case is unique because of his advanced age, complete resolution of symptoms, attainment of his ideal body weight and full return to his previous level of functioning. The diagnosis at discharge relied on the negative biopsy result for malignancy, the history of complicated chronic otitis media with effusion, and the patient’s improvement after antibiotic treatment. Subsequent clinical improvement at follow-up gave further support to the diagnosis of infection. Although weight loss was the major sign raising suspicion of malignancy, it is not a common feature of nasopharyngeal carcinoma without distant metastases.6 As occurs in many older patients, this patient did not have the usual clinical features of infection. CT, MRI and bone scans demonstrated the extent and location of abnormalities but could not distinguish between infection and malignancy. The FDG-PET scan indicated there were no metastases.
Ciprofloxacin was chosen on the basis of the ear discharge culture result and because P. aeruginosa has been implicated as the major pathogen causing skull base osteomyelitis related to ear infections — especially in people with diabetes who have otitis externa.7 S. aureus was thought likely to be a colonising organism rather than a copathogen; the clinical response to the ciprofloxacin was consistent with this. A challenging question with this patient was the optimal duration of ciprofloxacin treatment, especially when the ear discharge persisted for up to 7 months. The decision to stop treatment with the antibiotic would be a matter of judgement based on clinical features, persistently normal CRP levels and improvements on serial scans. After cessation of antibiotic treatment, the patient would require regular and prolonged follow-up to detect early relapse of infection.
Magnetic resonance image showing skull base osteomyelitis and otitis media
Competing interests
None identified.
References
- Kulkarni S, Lee A, Lee JH. Sixth and tenth nerve palsy secondary to pseudomonas infection of the skull base. Am J Ophthalmol 2005; 139: 918-920. 0_i1091886
- Mani N, Sudhoff H, Rajagopal S, et al. Cranial nerve involvement in malignant external otitis: implications for clinical outcome. Laryngoscope 2007; 117: 907-910. 0_i1091888
- Subburaman N, Chaurasia MK. Skull base osteomyelitis interpreted as malignancy. J Laryngol Otol 1999; 113: 775-778. 0_i1091890
- Ducic Y. Skull base osteomyelitis. South Med J 2006; 99: 1051. 0_pgfId-1091892
- Singh A, Al Khabori M, Hyder MJ. Skull base osteomyelitis: diagnostic and therapeutic challenges in atypical presentation. Otolaryngol Head Neck Surg 2005; 133: 121-125. 0_i1091893
- Wei WI, Sham JS. Nasopharyngeal carcinoma. Lancet 2005; 365: 2041-2054. 0_i1091895
- Sreepada GS, Kwartler JA. Skull base osteomyelitis secondary to malignant otitis externa. Curr Opin Otolaryngol Head Neck Surg 2003; 11: 316-323. 0_i1091898