





Volume 191 - Issue 2
“Barking up the right tree”: challenges for health care reform
Authors: Joachim P Sturmberg, Diana E O’Halloran, Claire Jackson, Christopher D Mitchell and Carmel M Martin
Med J Aust 2009; 191 (2): 64-66. || doi: 10.5694/j.1326-5377.2009.tb02691.x
Published online: 20 July 2009
Published online: 20 July 2009
Abstract
Current approaches to health care reform are largely based on the metaphor of imminent flood waves threatening to inundate the health care system. This metaphor reflects the system’s preoccupation with disease and disease management in a hospital-centric environment.
We suggest that the debate needs to be reframed around health, or more precisely the patient’s health experience. Most patients are healthy most of the time, and even those with identifiable morbidities generally regard themselves as being in good health.
The majority of people receive most of their care in the community from primary care professionals. An integrated, effective and efficient primary health care system supports continuity of care through a primary care provider and fosters clinical leadership that is supported by other primary health care professionals and medical specialists.
Each primary care setting will have its own model that best provides flexible and responsive services to meet its patients’ needs and expectations.
Health care reform is a perpetual “political hot potato”, with successive governments talking about the “right” solution for our ailing health system. The way we talk about these reforms matters: as Lakoff has pointed out, the metaphors we use unveil our perceptions, our ways of thinking, and most importantly, our ways of acting.1 So far, debate on health care reform has predominantly been about diseases, although in recent times, the issues of community-based health and illness care for the majority of people have begun to permeate the argument.
The prevailing metaphor: “flood waves threatening to inundate the health care system”
This metaphor suggests that the current challenges (our ageing population, increasing levels of chronic illness, high-cost interventions and health workforce shortages) are unmanageable. This is based on a view of health as a negative state — the absence of disease and infirmity (Box 1). Not surprisingly, the focus on disease and infirmity steers discussions towards disease-specific management by hospital specialists, the use of high-cost technologies and therapies, and the need to control medical practice.
The emphasis on a disease-oriented environment — reinforced by media hype — fuels people’s perceptions of a steady decline in their health, exaggerates anxieties about disease and disease risk,2 encourages the denial of death as the eventual endpoint of care, and perpetuates unrealistic expectations of cure or treatment for every ailment.
The reality looks somewhat different. Most people are healthy most of the time, and most people adapt to their non-life-threatening illnesses and still regard themselves as being in good health. Reframing the debate around patients’ experience of health should guide the discussion and lead to enlightening insights.
Over the past century, our disease-free life span and our capacity to manage ill health have increased dramatically. However, vested interest groups and the media are fostering the medicalisation of everyday life by overstating the relevance of everyday symptoms, the risk of future disease, and the successes of novel experimental treatments. Having conquered premature death from acute infectious disease, most of us live with, and will die from, chronic degenerative diseases. Archie Cochrane’s insights are pertinent in this context: “Cure is rare while the need for care is widespread, and ... the pursuit of cure at all costs may restrict the supply of care”.3
A metaphor for change: “barking up the right tree”
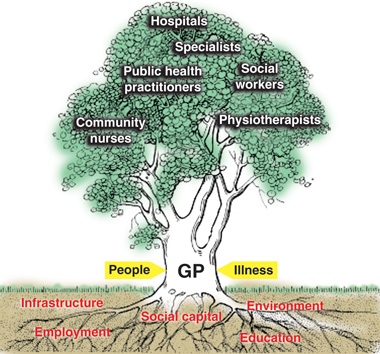
If we regard the current way of thinking as “barking up the wrong tree”, what would the right tree look like (Box 2)? Like a tree, which needs solid foundations to grow and thrive, the health system does not develop autonomously — it is bound and constrained by the broader health, societal and environmental system, and the functioning “whole” of the health system is clearly greater than the sum of its parts.
Medical care is embedded in society, and the impact of factors such as education, employment, social capital, physical infrastructure and the environment on health has been extensively described in the literature.
Patients commonly start their journey into the health care system by consulting a general practitioner, who, if need be, calls on the support of other primary health care professionals, consultant medical specialists, and hospitals. Public health, safety and environmental officers contribute to community health through their focus on matters such as the safety of our food and water, the safe disposal of sewage and air pollutants, and the safety of our transport infrastructure.
The focus of GPs/primary care physicians differs markedly from that of other medical professionals. We focus on people, not diseases. Primary care operates in the realm of uncertainty, as people present feeling ill — not diseased or pathological — and expect to be healed, in that they want to feel whole again, rather than achieve the absence of identifiable pathology.4 Healing, since the time of our ancient forebears, has been based on trust, an ongoing relationship between the doctor/healer and patient, and seeing and understanding the patient’s illness as a problem of the whole person in his or her environment.4
A primary health care-based health system?
Now that the prospect of greater community-based care has finally entered the debate, a major emphasis is being placed on the role of primary health care. How realistic is the expectation that primary health care can avert the coming flood when our health system remains largely grounded in hospital-, specialist- and disease-centric health service models?
We would suggest that primary health care’s capacity to deliver depends in large measure on the ability of decisionmakers to focus their thinking on health and to appreciate how the fundamental nature and characteristics of primary health care — and particularly general practice — enable it to meet the community’s expectations so effectively. It also depends, in part, on whether primary health care is regarded as a structure or a function of the health care system.
Looking specifically at general practice (rather than the broader primary health care system), we regard it as a function of the health system and emphasise the characteristics associated with its proven cost-effectiveness: person-focused care and the C’s of primary care — competence, continuity, comprehensiveness and coordination, inevitably associated with communication, collaboration, compliance and balancing competing demands (Box 3).5
Viewed from this perspective, reconfiguration of existing health system structures would need to be reordered towards quite different objectives. How could this be achieved?
The production of health
The core function of a tree is to produce fruit; the core function of the health system is to produce health. The fruits of care are represented by our patients’ experience of health, both in the presence and absence of identifiable pathologies.6,7
The reconfigured health system we envisage will primarily measure health, rather than focusing on disease-specific indicators or mortality statistics to demonstrate its achievements.6,7 The difference is important, as recent experiences in the United Kingdom have shown that an undue focus on disease-specific processes and outcomes (especially if imposed without adequate professional review, and attracting financial reward) can rapidly distract from the central components of care that achieve good health outcomes.8-10 The UK has realised the importance of patient health measures and has started to develop indicators.7
Patients demand and deserve holistic health care in the presence or absence of identifiable pathology, the latter being far more common than the former. If we want to achieve health for our patients, primary care needs to be strengthened to allow the most effective local primary care service to emerge.
The way forward
Internationally, there is now a strong move towards people-centred health care, with flexible teams configured around the primary care physician.4 This is known to be associated with better, more equitable and more cost-effective care.11
The current Australian health care reform process is embracing the notions of people-centred health care, and suggestions so far herald significant opportunities in this area.
The National Health and Hospitals Reform Commission’s interim report highlights the centrality of the individual and family as the focus for our future reform energies.12 The National Primary Health Care Strategy has identified the importance of continuity of care and a holistic health focus, and the recently established Preventative Health Taskforce will explore the powerful link between health and behaviour.
It has been suggested that the trunk of the health care tree need not be the physician, and that any other suitably trained health professional would be equally effective in that role. We disagree — not through self-interest, but rather, based on sound evidence that the primary care physician’s core skills relate to the ability to deal with the uncertainties and complexities of illness in the community, be it acute infectious or chronic degenerative disease, and to manage modifiable risk efficiently.
These skills are particularly important when dealing with patients affected by multiple morbidities, whose management requires integration and coordination, ideally delivered within flexible team-based arrangements at the practice level.13 This is teamwork through clinical leadership, expanded health professional roles and delegation, rather than role substitution. The crucial importance of continuity of care with a primary care provider, rather than a service, is increasingly emerging as the missing ingredient in health care reform, both in Australia and internationally.
Notwithstanding the accumulating persuasive evidence of the benefits of people-centred primary health care, those driving reform still appear to be giving mixed messages. For example, policies promoting workforce substitution disregard the evidence that personal ongoing relationships are the key to good patient health and threaten to cause even greater fragmentation of care, whereas workforce supplementation policies would enable the delivery of more integrated, effective and efficient care. Information systems are important for documentation and transfer of information, and are critical to quality and safety, but they can never be a substitute for the knowledge carried in the heads of the patient and doctor.
The Australian Government has recognised that the funding of health care services misses the needs of patients. However, suggested actions have largely focused on the hospital system, with some recognition of the need to provide more appropriate non-acute care for older Australians.
The 2020 Summit went further, recommending the development of a single, integrated community-based health care system, operating through a person- and family-centred collaborative approach, across disciplines, services and sectors provided by a diverse health workforce with new boundaries.
Let us take this recommendation to heart and step beyond the disease and sickness focus of the past, build on the emerging evidence base for continuing and comprehensive whole-person care and its benefits, and chart a new holistic vision for healthy populations of the future.
Competing interests
None identified.
References
- Lakoff G, Johnsen M. Metaphors we live by. Chicago: University of Chicago Press, 2003. 0_i1092010
- Barsky A. The paradox of health. N Engl J Med 1988; 318: 414-418. 0_i1092012
- Cochrane AL. Effectiveness and efficiency: random reflections on the health services. London: Nuffield Hospitals Trust, 1972. 0_i1092014
- Sturmberg JP. The foundations of primary care: daring to be different. Oxford: Radcliffe Publishing, 2007. 0_i1092016
- Kroenke K. The many C’s of primary care. J Gen Intern Med 2004; 19: 708-709. 0_i1092018
- Hart J. Expectations of health care: promoted, managed or shared? Health Expect 1998; 1: 3-13. 0_i1092020
- Timmins N. NHS goes to the PROMS. BMJ 2008; 336: 1464-1465. 0_i1092022
- Campbell SM, McDonald R, Lester H. The experience of pay for performance in English family practice: a qualitative study. Ann Fam Med 2008; 6: 228-234. 0_i1092024
- Guthrie B, McLean G, Sutton M. Workload and reward in the Quality and Outcomes Framework of the 2004 general practice contract. Br J Gen Pract 2006; 56: 836-841. 0_pgfId-1092026
- Steel N, Maisey S, Clark A, et al. Quality of clinical primary care and targeted incentive payments: an observational study. Br J Gen Pract 2007; 57: 449-454. 0_i1092027
- Wennberg D, Berkson D, Rider B. Building partnerships: addressing overuse, underuse and misuse of care. Healthc Exec 2008; 23: 8-10, 12, 14-15. 0_i1092030
- National Health and Hospitals Reform Commission. A healthier future for all Australians. Interim report December 2008. Canberra: NHHRC, 2009. http://www.nhhrc.org.au/internet/nhhrc/publishing.nsf/Content/interim-report-december-2008 (accessed May 2009).
- Martin CM, Sturmberg JP. Complex adaptive chronic care. J Eval Clin Pract 2009; 15: 571–577. 0_i1092034