





Volume 189 - Issue 9
Zygomycosis due to Saksenaea vasiformis caused by a magpie peck
Author: Paul A Wilson
Med J Aust 2008; 189 (9): 521-522. || doi: 10.5694/j.1326-5377.2008.tb02150.x
Published online: 3 November 2008
Published online: 3 November 2008
An immunocompetent patient developed a necrotising soft tissue infection after being pecked by a magpie. The infection was caused by the fungus Saksenaea vasiformis, an uncommon human pathogen. Special culture techniques are required to induce sporulation to enable identification of the organism.
Clinical record
An 84-year-old woman presented to our hospital emergency department with cellulitis of the left lower leg. There was a small, dry eschar and some adjacent purplish discolouration (Box 1, A). Eleven days previously, she had been pecked above the left ankle by a magpie (Gymnorhina tibicen), which her daughter kept as a pet.
The woman reported that within a week of the pecking incident she had experienced pain, swelling and redness on the lower leg near the injury site. Worsening symptoms had led her to present to hospital.
She had a history of acute myocardial infarction many years previously and mild chronic obstructive pulmonary disease. Surgical history included a hysterectomy and varicose vein ligation. She was an ex-smoker.
At the time of admission, capillary refill in the foot was sluggish and the patient was unable to bear weight on the affected leg. There was no fever, and the white cell count (8.9 × 109/L) was within the normal range. Treatment with intravenous dicloxacillin was commenced.
The patient’s leg failed to improve during the first week of treatment (Box 1, B), despite the addition of metronidazole on Day 5 after admission and gentamicin on Day 6. The antibiotics were changed to ticarcillin–clavulanic acid on Day 9. The patient had low-grade fevers from Day 7 and her white cell count progressively rose to 31.1 × 109/L.
A Doppler ultrasound scan of the thigh on Day 11 showed occlusion of the superficial femoral artery with reperfusion by collateral vessels, consistent with atherosclerotic peripheral vascular disease. Surgical exploration was performed on the same day, with wide resection of necrotic skin and subcutaneous tissue. Operative findings were of occluded vessels with absent blood flow in the areas of necrosis. Bacterial culture of the necrotic tissue showed profuse growth of Escherichia coli and Klebsiella pneumoniae, which led to a change in antibiotic treatment to ceftriaxone.
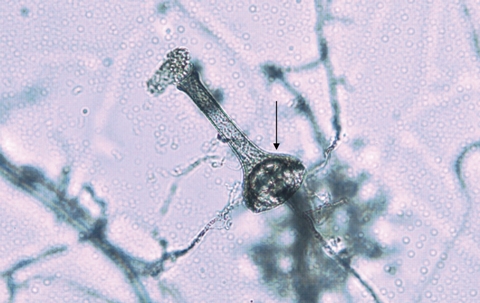
Histopathological examination of the debrided tissue showed coagulative necrosis with scattered fungal hyphae, especially within blood vessels. The hyphae had occasional septa and branched at variable angles. The more viable areas contained acute inflammatory cells. A white downy fungus grew in culture from a tissue specimen after 5 days, but the fungus was difficult to identify as it failed to sporulate in culture. When subsequently grown on Czapek Dox agar, the isolate eventually produced vase-shaped sporangia typical of Saksenaea vasiformis (Box 2).
Treatment with intravenous amphotericin B was commenced on receipt of the histopathology results. However, the patient’s foot became progressively more ischaemic, with development of frank gangrene by Day 16 after admission. Above-knee amputation was performed on Day 17. A computed tomography scan of the chest showed no evidence of pulmonary fungal infection. The antimicrobial agents were ceased 6 days after surgery, and the patient was eventually discharged to a nursing home on Day 44.
Discussion
Fungi of the class Zygomycetes are ubiquitous in nature, being found in soil and decaying organic matter. However, they are uncommon human pathogens. Zygomycosis in humans is usually seen either in immunosuppressed patients or in immunocompetent people after cutaneous inoculation from trauma or surgery.
S. vasiformis was first described in 1953 by Saksena as a new zygomycete isolated from forest soil in India.1 Infection due to S. vasiformis was first observed in 1977 in a young man who had sustained severe cranial trauma in a motor vehicle accident. The infection involved the eye and brain.2 A total of 29 cases of human infection due to S. vasiformis have since been reported in the English language literature.3,4 Most cases occurred as cutaneous zygomycosis in immunocompetent patients after traumatic inoculation. S. vasiformis typically requires special culture techniques to induce sporulation and enable definitive identification. It shares these characteristics with Apophysomyces elegans, another zygomycete.5
Reports in the literature of skin or soft tissue infections following bird pecking injuries are sparse. These include a Pseudomonas aeruginosa infection of the finger after a swan bite6 and a Bacteroides scalp infection after an owl attack.7 More serious infections relating to trauma involving a bird have included septic arthritis of the knee after a chicken bite8 and a fatal brain abscess in a child caused by a rooster peck.9 Zygomycoses have been transmitted by insect or spider bites, with the pathogens reported as Rhizopus spp,10,11 Apophysomyces elegans12 and Mucor hiemalis.13
The infection in our patient was in some ways typical of infection with S. vasiformis, in that it occurred in an immunocompetent patient after trauma, albeit of an unusual nature. The presence of pre-existing peripheral vascular disease may have contributed to the aggressive course of the infection in this patient.
Zygomycetes are rapidly growing fungi with a tendency to invade blood vessels, causing occlusion and infarction. An unusual infective agent must be considered in the setting of worsening soft tissue infection despite broad-spectrum antibiotic therapy, and early debridement accompanied by fungal culture may enable diagnosis. Trauma related to a bird-pecking injury should be added to the list of predisposing risk factors for zygomycosis, as exemplified by this case.

Competing interests
None identified.
Acknowledgements
I would like to thank Dr Stephen Cox, General Surgeon at Calvary Mater Newcastle, for allowing me to see the patient and publish this report; Sr Theresa Richards, Clinical Nurse Specialist in wound care at Calvary Mater Newcastle, for the photographs of the patient; and Mr David Pacey, Medical Laboratory Scientist, for identifying the fungus and providing photographs of its morphology.
References
- Saksena SB. A new genus of the Mucorales. Mycologia 1953; 45: 426-436. 0_i1091881
- Dean DF, Ajello L, Irwin RS, et al. Cranial zygomycosis caused by Saksenaea vasiformis. J Neurosurg 1977; 46: 97-103. 0_i1091883
- Vega W, Orellana M, Zaror L, et al. Saksenaea vasiformis infections: case report and literature review. Mycopathologia 2006; 162: 289-294. 0_i1091885
- Blanchet D, Dannaoui E, Fior A, et al. Saksenaea vasiformis infection, French Guiana. Emerg Infect Dis 2008; 14: 342-344. 0_i1091887
- Chakrabarti A, Kumar P, Padhye AA, et al. Primary cutaneous zygomycosis due to Saksenaea vasiformis and Apophysomyces elegans. Clin Infect Dis 1997; 24: 580-583. 0_i1091889
- Ebrey RJ, Hayek LJHE. Antibiotic prophylaxis after swan bite. Lancet 1997; 350: 340. 0_i1091891
- Davis B, Wenzel RP. Striges scalp: Bacteroides infection after an owl attack. J Infect Dis 1992; 165: 975-976. 0_i1091893
- Huang C-M, Chou C-T, Chen H-T, Jim Y-F. Septic arthritis following a chicken bite. Clin Rheumatol 1998; 17: 540-542. 0_i1091895
- Berkowitz FE, Jacobs DW. Fatal case of brain abscess caused by rooster pecking. Pediatr Infect Dis J 1987; 6: 941-942. 0_i1091897
- Adam RD, Hunter G, Di Tomasso J, Comerci G Jr. Mucormycosis: emerging prominence of cutaneous infections. Clin Infect Dis 1994; 19: 67-76. 0_i1091899
- Hicks WL Jr, Nowels K, Troxel J. Primary cutaneous mucormycosis. Am J Otolaryngol 1995; 16: 265-268. 0_i1091901
- Weinberg WG, Wade BH, Cieny G III, et al. Invasive infection due to Apophysomyces elegans in immunocompetent hosts. Clin Infect Dis 1993; 17: 881-884. 0_i1091903
- Prevoo RL, Starink TM, de Haan P. Primary cutaneous mucormycosis in a healthy young girl. Report of a case caused by Mucor hiemalis Wehmer. J Am Acad Dermatol 1991; 24: 882-885. 0_i1091905