





Volume 189 - Issue 9
Disseminated Saksenaea vasiformis in an immunocompetent host
Authors: Dean J Trotter, Gena Gonis, Erin Cottrill and Christopher Coombs
Med J Aust 2008; 189 (9): 519-520. || doi: 10.5694/j.1326-5377.2008.tb02149.x
Published online: 3 November 2008
Published online: 3 November 2008
Clinical record
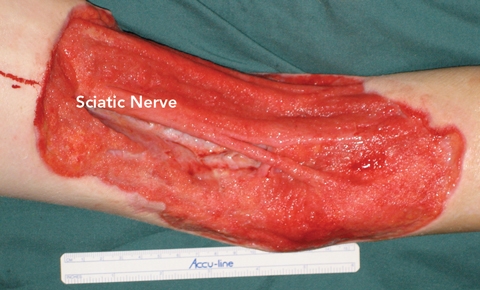
A previously healthy 11-year-old boy presented to the Royal Children’s Hospital (RCH) with a 20 × 12 cm necrotising wound of the left popliteal fossa (Figure A). A further inflammatory lesion was evident on the anteromedial left thigh, extending into the groin. The boy was febrile and cachectic, weighing 30 kg.
The patient had a history of a suspected insect bite in the area of the popliteal fossa 5 months earlier. The suspected bite wound had developed into an 8 cm necrotic lesion over several months. The patient had initially presented to a regional centre (a few days after the suspected bite), where he was treated with oral twice-daily Augmentin Duo Forte (amoxycillin–clavulanate) (GlaxoSmithKline Australia) 750 mg, excisional debridement and split-skin grafting, with 90% graft take. The wound was treated topically with dressings. The patient then emigrated with his family to Dubai. The wound subsequently broke down and was serially debrided, with further skin grafting and antibiotic coverage with amoxycillin and ciprofloxacin. Despite 4 weeks of treatment, the wound progressed and the family was referred by a doctor in Dubai to the RCH.
Investigations at our hospital revealed a white cell count of 27.4 × 109/L (reference range [RR], 4.5–13.5 × 109/L), a C-reactive protein level of 29 mg/L (RR, < 8 mg/L) and an albumin level of 26 g/L (RR, 33–47 g/L). An ultrasound scan confirmed the presence of a necrotic lymph nodal mass in the left groin.
Antibiotic therapy with 6-hourly intravenous Timentin (ticarcillin–clavulanate) (GlaxoSmithKline Australia) 1.5 g was commenced. Wound and tissue cultures revealed the presence of Staphylococcus aureus and Prevotella species. Although fungal cultures were requested, no fungal pathogen was isolated. The popliteal fossa wound and necrotic inguinal nodes were surgically debrided over the following 2 weeks. This revealed extensive necrosis of the biceps femoris and semimembranosus muscle, with undermining subcutaneous fat necrosis immediately adjacent to the wound. Ten centimetres of sciatic nerve and the popliteal vessels were exposed. Both wounds were treated by topical negative pressure (vacuum) dressing (VAC Therapy System, Kinetic Concepts Inc, San Antonio, Tex, USA).
When the patient failed to improve after 5 days of intravenous antibiotic treatment, clinical suspicion of an atypical disease was heightened. Multidisciplinary discussions led to a specific request to the microbiology department to attempt to identify fungal disease. Further tissue cultures under specific conditions (see below) showed growth of the fungus Saksenaea vasiformis. Histopathological analysis of resected tissue revealed extensive subcutaneous fat necrosis with calcification and many non-septate hyphae with irregular diameters and branching — features consistent with zygomycosis (mucormycosis).1 These features were not seen on Gram stain.
Antifungal therapy was initiated with amphotericin B 45 mg given via central venous line over 24 hours initially and then intravenous liposomal amphotericin B 150 mg daily. Major predisposing factors to zygomycosis were excluded: specifically, hyperglycaemia, ketoacidosis and immunosuppressive disorders.1 Notable findings included a raised IgE level. Although this can be associated with hyper-IgE syndrome, the patient had no other signs of this disease.
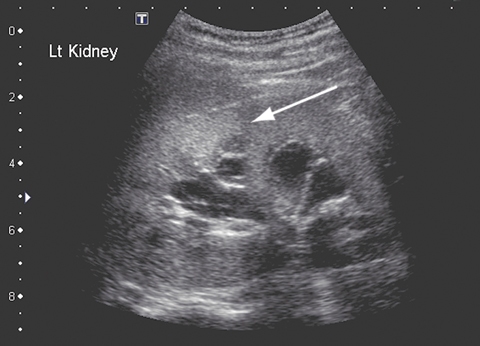
After 5 weeks of treatment with amphotericin B, the patient became unwell, with a high fever and moderate renal impairment. His creatinine level had increased from 0.06 to 0.17 mmol/L (RR, 0.03–0.08 mmol/L); his urea level was 18.7 mmol/L (RR, 2.1–6.5 mmol/L), and the glomerular filtration rate was 29 mL/min (RR, 100–140 mL/min). A renal ultrasound scan revealed parenchymal fungal spores (Figure B). Amphotericin B treatment was ceased and twice daily oral posaconazole 400 mg commenced. Renal function normalised within about 7 days. Follow-up imaging 6 weeks later revealed resolution of renal fungal disease.
After 6 weeks of antifungal treatment and no growth evident on serial tissue cultures, the wounds were surgically closed. The popliteal fossa wound was treated with a pedicled medial gastrocnemius muscle flap and skin graft to cover the exposed neurovascular structures. The groin wound was closed with a sartorius muscle turnover flap and skin graft. Both the wound and donor sites fully healed without complication (Figure C).
 |
|
A: Necrotising wound of the left popliteal fossa on presentation. |
 |
 |
Since it was first isolated in 1953,2 Saksenaea vasiformis has been reported to cause human infection in about 30 cases. In only two cases has disseminated disease been reported, both occurring in immunocompetent patients and having fatal outcomes.3,4 S. vasiformis belongs to the class Zygomycetes and order Mucorales. The usual manifestation of disease is reported to be skin and soft-tissue infections, most commonly occurring secondary to trauma,1 but can also follow haematogenous dissemination.
Lessons from practice
Multidisciplinary care is fundamental in dealing with complex or unusual conditions.
Always consider atypical pathogens, particularly fungi, when a condition fails to respond to the perceived ideal treatment.
If considering a fungal pathogen, consult microbiological opinion to aid identification of the species.
Posaconazole can be used safely and successfully in children to treat disseminated fungal disease.
Although the two previously reported cases of disseminated S. vasiformis infection were fatal, our report details the successful treatment of disseminated disease by a combination of surgery and systemic antifungal therapy. This case thus highlights several important issues in the treatment of zygomycosis.
A multidisciplinary team approach is essential for a successful outcome. Exclusion of underlying immunodeficiency is paramount, as its presence often leads to a fatal outcome.1
Surgical treatment combined with appropriate antifungal therapy is the mainstay of treatment. In the case we describe, the patient required serial debridements and the use of vacuum dressings until microbiological evidence of eradication of fungi was achieved. Vacuum dressings were a good alternative to more labour-intensive and painful forms of dressing. The dressings were changed in theatre every 3–5 days. Negative pressure dressings have been shown to improve wound healing by increasing tissue oxygenation via a reduction of interstitial fluid5,6 and reducing bacterial counts in the wound.7
Diagnosis and identification of the fungus is important. Zygomycosis must be suspected in any wound that is worsening despite appropriate treatment. Tissue culture, rather than routine wound swabs, provides the most appropriate specimen. It is important to inform the microbiology laboratory of clinical suspicion of zygomycosis. The tissue should be cultured intact to preserve the viability of the irregularly septate zygomycete hyphae. This also ensures that cultures are incubated for the extended period necessary for fungal isolation. S. vasiformis is a fast-growing organism and can usually be isolated from culture within 72 hours.1,8 Once isolated, full identification for fungi may require extended time and specialist media in a reference laboratory.
Antifungal therapy is essential to the treatment of this organism, and amphotericin B has traditionally been the agent of choice. However, its significant side effects, notably nephrotoxicity, often affect treatment, as seen in this case. Our patient’s renal impairment resolved after cessation of amphotericin treatment, confirming its nephrotoxicity. Treatment with posaconazole, a new generation triazole antifungal, was initiated after withdrawal of amphotericin treatment, without leading to any complication or relapse of the disease.
There is little information on the treatment of zygomycosis with posaconazole. To our knowledge, ours is the first reported case of successful salvage treatment of disseminated zygomycosis with this drug.
Posaconazole has been shown to be effective against zygomycosis when other therapy has been ineffective or complications have occurred due to the therapy.9 As posaconazole is not generally used in children under the age of 13 years, its safety profile in children is unknown. The drug is available as an oral suspension and is generally administered at a dose of 800 mg daily in divided doses. The patient described here received 400 mg twice daily without complication. The duration of therapy is dictated by the presence of disease. Minor common side effects include nausea and headache. Serious side effects are rare, but hepatic impairment may occur, so liver function should be monitored every 2–3 weeks during therapy. Posaconazole interacts with several immunosuppressive agents and has few contraindications.
In conclusion, this report shows that disseminated zygomycosis, specifically S. vasiformis infection, may occur in immunocompetent individuals. It also shows how, with multidisciplinary care, mortality may be avoided.
Competing interests
None identified.
References
- Holland J. Emerging zygomycoses of humans: Saksenaea vasiformis and Apophysomyces elegans. Curr Top Med Mycol 1997; 8: 27-34. 0_i1091898
- Saksena SB. A new genus of the Mucorales. Mycologia 1953; 45: 426-436. 0_i1091900
- Torell J, Cooper BH, Helgeson NG. Disseminated Saksenaea vasiformis infection. Am J Clin Pathol 1981; 76: 116-121. 0_i1091902
- Hay RJ, Campbell CK, Marshall WM, et al. Disseminated zygomycosis (mucormycosis) caused by Saksenaea vasiformis. J Infect 1983; 7: 162-165. 0_i1091904
- Bucalo B, Eaglstein WH, Falanga V. Inhibition of cell proliferation by chronic wound fluid. Wound Repair Regen 1993; 1: 181-186. 0_i1091906
- Argenta LC, Morykwas MJ. Vacuum-assisted closure: a new method for wound control and treatment: clinical experience. Ann Plast Surg 1997; 38: 563-576. 0_i1091908
- Morykwas MJ, Argenta LC, Shelton-Brown EI, McGuirt W. Vacuum-assisted closure: a new method for wound control and treatment: animal studies and basic foundation. Ann Plast Surg 1997; 38: 553-562. 0_i1091910
- Padmaja IJ, Ramani TV, Kalyani S. Cutaneous zygomycosis: necrotising fascitis due to Saksenaea vasiformis. Indian J Med Microbiol 2006; 24: 58-60. 0_i1091912
- MIMS online drug information for posaconazole. http://www.mims.com.au (accessed Sep 2008).