





Volume 189 - Issue 7
Misdiagnosis of acute eye diseases by primary health care providers: incidence and implications
Authors: Michael O Statham, Anamika Sharma and Anthony R Pane
Med J Aust 2008; 189 (7): 402-404. || doi: 10.5694/j.1326-5377.2008.tb02091.x
Published online: 6 October 2008
Published online: 6 October 2008
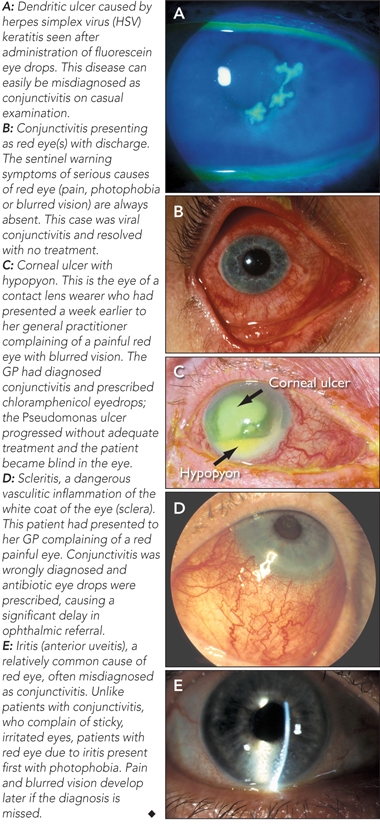
Patients who notice a red eye or other acute ophthalmic symptoms often present first to their general practitioner, optometrist or local hospital emergency department. Although the most common acute eye diseases in primary practice are the usually benign conditions of viral, bacterial and allergic conjunctivitis, rarer but more serious causes of red eye such as iritis, keratitis and acute glaucoma can lead to permanent loss of vision.
The primary health care provider’s initial diagnosis and management can be critical to the patient’s ophthalmic outcome. In one United Kingdom study of 55 patients in which an ophthalmologist had diagnosed a red-eye disorder, only nine had been correctly diagnosed by the referring practitioner.1 To our knowledge, no study of the accuracy of diagnosis of eye conditions by primary health care providers in Australia has yet been published. We audited the hospital records of 1062 new patients presenting to the eye emergency services of the ophthalmology departments of the two major Brisbane hospitals, and analysed the accuracy of the diagnosis and implications of the initial care provided to these patients by their local doctor or optometrist.
Lessons from practice
Patients with acute eye problems presenting to primary health care providers are often misdiagnosed or mismanaged.
Topical antibiotic therapy is overprescribed for acute eye conditions.
Particular attention should be paid to sentinel warning symptoms — in particular the presence of one or more of pain, photophobia or blurred vision — as these symptoms almost always indicate serious acute eye disease rather than conjunctivitis.
If a patient with a red eye reports pain, photophobia or blurred vision he or she should be given no treatment and referred immediately.
Methods
Patient records from consecutive presentations to eye emergency services of ophthalmology departments at two hospitals — Princess Alexandra Hospital (PAH) from 18 April to 25 October 2006 and the Royal Brisbane and Women’s Hospital (RBWH) from 1 July to 30 September 2006 — were collected and reviewed. Approval for the project was obtained from the Director of Surgery, Head of Ophthalmology and Ethics Committee of each hospital.
Inclusion criteria were initial presentation to a primary health care provider (PHCP) — defined as a GP, optometrist or hospital emergency department doctor — and subsequent referral or patient self-presentation to an eye emergency service for the same complaint. The diagnosis in the ophthalmology department was compared with that by the PHCP, and the accuracy of diagnosis was determined. A preventable adverse outcome was deemed to have occurred if the patient had eye pain, loss of vision, or had been given inappropriate medication that could have been avoided with appropriate initial management or prompt referral. A further subjective assessment of the severity of the adverse outcome was then made.
Results
Data were collected for 1062 patients during the designated periods at the two hospitals: 614 (57.8%) from PAH and 448 (42.2%) from RBWH. The referring PHCP was a GP in 50.4%, hospital emergency department doctor in 38.9%, and an optometrist in 10.7% of cases. The 10 most common reasons that PHCPs referred patients to ophthalmology departments are shown in Box 1.
Accuracy of primary health care practitoners’ diagnoses
A correct initial diagnosis (ie, matching the final ophthalmology department diagnosis) was given for 192 (35.9%) of the 535 patients referred by GPs, 173 (41.9%) of the 413 patients referred by emergency department doctors and 55 (48.2%) of the 114 patients referred by optometrists.
Implications of initial inappropriate care by primary health care providers
Preventable adverse outcomes: In 123 of the 1062 patients (11.6%), there was an adverse outcome resulting from misdiagnosis or mismanagement by the PHCP. Adverse outcomes in these 123 patients were mild in 63 (51%), moderate in 49 (40%) and severe in 11 (9%). Conditions that were misdiagnosed and subsequently associated with a severe adverse patient outcome are shown in Box 2. In most cases (74%), adverse outcomes were associated with misdiagnosis by PHCPs; in the remainder (26%), there had been a correct initial diagnosis, but subsequent incorrect treatment, or a significant delay in referral. In the 123 patients with preventable adverse outcomes resulting from misdiagnosis or mismanagement, the PHCP was a GP in 78%, an emergency department doctor in 17% and an optometrist in 5% of cases. The 11 most severe preventable adverse outcomes are described in Box 3.
Topical antibiotic therapy: Of the total of 1062 patients, 199 (18.7%) had been prescribed topical antibiotic therapy at their initial consultation with their PHCP. Of the 535 patients referred by GPs, 108 (20.2%) had been prescribed antibiotic eye drops before referral. In 54% of these 108 patients, the therapy was judged inappropriate or unnecessary on ophthalmic review, and was ceased.
Iritis: There were 59 patients with iritis (acute anterior uveitis), representing 5.6% of the total 1062 patients. Less than a third of patients with iritis (16 of 59; 27%) were diagnosed correctly by the PHCP. Eleven of the 59 patients with iritis (19%) were initially misdiagnosed as having conjunctivitis and treated with topical antibiotic therapy by their GP. Fourteen patients were given no diagnosis and no therapy. Seven patients had their condition misdiagnosed as red eye and were given no therapy. Iritis was misdiagnosed as glaucoma in three patients, hyphaema in two patients, keratitis in two patients, cataract in two patients, and as macular oedema and pain in one patient. The average time to referral or self-presentation to an eye emergency service for patients with iritis was 2.4 days (range, 0–16 days).
Discussion
Patients with acute eye problems presenting to PHCPs, especially GPs, are often misdiagnosed or mismanaged. In most cases, this does the patient no harm — for example, misdiagnosing viral conjunctivitis as bacterial conjunctivitis and inappropriately prescribing antibiotic eye drops is unlikely to cause complications, and the patient will spontaneously recover from the infection. However, in some acute eye conditions, the prescription of topical antibiotics can be very harmful indeed — not through any ill effects of the drug, but through the subsequent delay in referral. In the case of serious acute eye conditions like severe iritis or acute glaucoma, a delay of even a few days can result in permanent loss of vision or even blindness. Examples of potentially serious eye diseases that may present to PHCPs are shown in Box 4.
In our survey, of 11 patients identified as having had a preventable, severe adverse outcome, 10 had initially presented to their PHCP with a unilateral red eye. All 10 were incorrectly diagnosed as having conjunctivitis and all had been inappropriately prescribed chloramphenicol eye drops as treatment. All had reported ocular pain, photophobia or blurred vision to their PHCP at the initial consultation. The 11th patient had retinal detachment.
There is a perception among many ophthalmologists that many GPs “call every red eye conjunctivitis” and that topical antibiotics are overprescribed for acute eye problems. In our review, in more than 50% of cases in which topical antibiotic therapy had been commenced by the PHCP, it was immediately ceased at the first ophthalmology review as being unnecessary or inappropriate. In addition to contributing to a serious delay in patient referral, topical antibiotic use can occasionally cause serious local and rarely systemic complications2 (eg, agranulocytosis from chloramphenicol). There may also be concerns that using antibiotics unnecessarily contributes to increasing antibiotic resistance of organisms.3
How can the situation be improved? A major problem is the lack of equipment, expertise and time available to a GP in a busy practice facing a new patient with an acute eye problem. Many eye conditions (including iritis and acute glaucoma) cannot be diagnosed without a slit lamp microscope and a means of measuring intraocular pressure — equipment that is rarely available to GPs. In addition, many GPs have had little ophthalmological training, and have limited time to spend with each patient.
To address these problems, it is suggested that GPs pay careful attention to the symptoms reported by patients with eye complaints, given the difficulty of accurately evaluating their signs. Particular attention should be paid to sentinel warning symptoms — in particular the presence of one or more of pain, photophobia or blurred vision — as these symptoms almost always indicate serious acute eye disease rather than conjunctivitis.4 Patients reporting one or more of these symptoms should be given no treatment, and referred to an ophthalmologist urgently. It should also be recognised by GPs that although unilateral viral conjunctivitis is common, a single red eye should be viewed with more suspicion than bilateral red eyes, which are more likely due to conjunctivitis.
1 The 10 most common reasons that primary health care providers referred patients to ophthalmology department emergency services
2 Conditions originally misdiagnosed by primary health care providers, leading to adverse events for patients
3 Severe adverse outcomes in 11 patients as a result of misdiagnosis or mismanagement by primary health care providers*
Competing interests
None identified.
References
- Harrison RJ, Wild JM, Hobley AJ. Referral patterns to an ophthalmic outpatient clinic by general practitioners and ophthalmic opticians and the role of these professionals in screening for ocular disease. BMJ 1988; 297: 1162-1167. 0_CHDECJCA
- Smith JR, Wesselingh S, Coster DJ. Is it time to stop using chloramphenicol? Aust N Z J Ophthalmol 1997; 25: 83-88. 0_BDCEAIED
- Rang HP, Dale MM, Ritter JM, Moore PK. Pharmacology. 5th ed. Edinburgh: Churchill Livingstone, 2003: 644-645. 0_i1092060
- Pane A. Practical ophthalmology: a survival guide for doctors and optometrists. Edinburgh: Churchill Livingstone, 2005. 0_i1092062