





Volume 188 - Issue 2
Mediastinal lymphadenopathy in a patient with previously treated T-cell acute lymphoblastic leukaemia
Authors: Narayan Karanth, Kumar P Prabhash, Pranjali N Karanth, Tanuja Shet, Shripad D Banavali and Purvish M Parikh
Med J Aust 2008; 188 (2): 117-118. || doi: 10.5694/j.1326-5377.2008.tb01537.x
Published online: 21 January 2008
Published online: 21 January 2008
Mediastinal lymphadenopathy in a patient with previously treated T-cell acute lymphoblastic leukaemia is a diagnostic problem. The differential diagnosis in an adult is sarcoidosis, metastases, lymphoma or, rarely, tuberculosis. Mediastinal lymph node involvement is uncommon in tuberculosis. In view of its relative rarity but good prognosis, it is important to distinguish tuberculous mediastinal lymphadenitis in adults from other causes of mediastinal masses.
Clinical record
An 11-year-old boy presented in September 1995 with bilateral cervical lymph node enlargement for 2 months and fever for 10 days. There was no significant medical or family history. On examination, he had generalised lymphadenopathy. Systemic examination was normal. He had a high white blood cell count (60 × 109/L) and a low platelet count. The diagnosis on bone marrow aspiration was T-cell acute lymphoblastic leukaemia. He was treated with the MCP-841 protocol as induction therapy,1 after which his bone marrow was reported to be in complete remission. He then underwent consolidation chemotherapy and prophylactic cranial radiotherapy and subsequently received six cycles of maintenance chemotherapy, which were completed by December 1997. He was lost to follow-up.
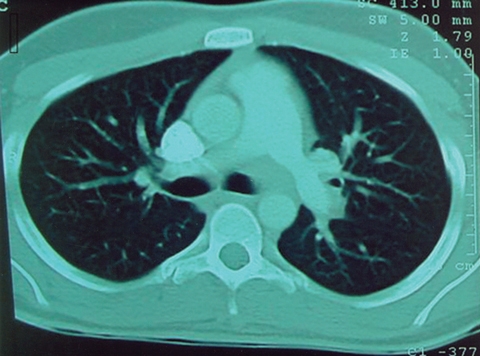
He presented again in January 2006 with hoarseness of 2 months’ duration. His complete blood count was normal. The erythrocyte sedimentation rate was 40 mm/h (reference range, 0–10 mm/h). His chest x-ray appeared normal. The Hopkins test (indirect laryngoscopy) showed a fixed left vocal cord. A subsequent computed tomography (CT) scan of the chest showed lymph nodes in the left para-aortic and aortopulmonary windows (Box 1). CT-guided fine-needle aspiration cytology was reported as inconclusive.
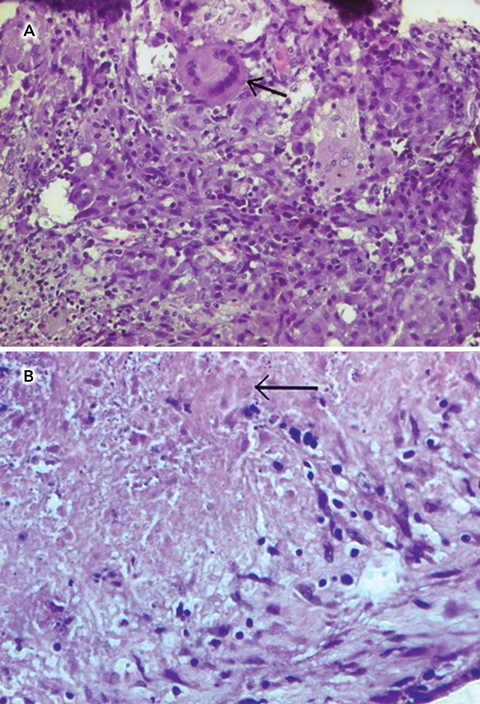
Fluorodeoxyglucose F18 positron emission tomography (PET) scan of the whole body showed active disease foci in lymph nodes in the aortopulmonary window and left axillary regions (Box 2). A bone marrow aspirate appeared normal, and bone marrow biopsy showed mildly hypocellular normal marrow. Video-assisted thoracoscopic surgical biopsy of the aortopulmonary lymph node showed histiocytic collections forming epithelioid granulomas with foreign-body and Langhans giant cells suggestive of necrotising granulomatous inflammation typical of tuberculosis (Box 3A and Box 3B). Stains for acid-fast bacilli and fungi were negative. Biopsy cultures for mycobacteria and fungi were negative. A Mantoux test was negative.
In April 2006, the patient was started on antituberculosis treatment with the standard four-drug regimen consisting of rifampicin, pyrazinamide, ethambutol and isoniazid. After 2 months of treatment, he was symptom-free and was started on a two-drug regimen of isoniazid and rifampicin for 7 months.
Discussion
Isolated mediastinal lymphadenopathy can be a challenge for the best of clinicians, more so when the patient has a history that might influence the diagnosis. In mediastinal lymphadenopathy, the differential diagnosis has to include both benign and malignant causes, because the therapeutic implications and prognosis of both are broad. Childhood lymphoblastic leukaemia is usually assumed to have been permanently eradicated in patients in long-term remission,but occasionally can recur after many years.2 In post-treatment relapses, or even very late relapses (5 to 20 years after diagnosis) in children, the tumour cells are clonally related to the leukaemic cells at diagnosis (shown by immunoglobulin heavy-chain locus or T-cell receptor gene sequencing), and are considered, therefore, to represent a slow re-emergence or escape of the initial cells.3 In a retrospective study of 2169 patients, the cumulative incidence of secondary neoplasm was 4.17% (SE, 0.46%) at 15 years and increased substantially after 20 years, reaching 10.85% (SE, 1.27%) at 30 years.4 In our case, the disease-free interval was 9 years. A diagnosis of relapse was initially suspected, but the peripheral smear and bone marrow results were normal.
As the CT-guided fine-needle aspiration cytology, done to clinch the diagnosis of relapse, had inconclusive results, a PET scan was planned to avoid an invasive procedure. PET is more efficacious than CT in differentiating benign from malignant focal lesions. However, fluorodeoxyglucose is not a cancer-specific agent, and false-positive findings have been reported. Infectious diseases (mycobacterial, fungal and bacterial), sarcoidosis, radiation pneumonitis and postoperative surgical conditions are reflected by intense uptake of fluorodeoxyglucose on PET scan.5
The results of bone marrow aspiration to rule out relapse were normal. Hence, it was decided to go ahead with a video-assisted thoracoscopic surgical biopsy of the active focus in the aortopulmonary window, which led finally to the diagnosis of tuberculosis. Although mediastinal lymphadenopathy is not a common manifestation of tuberculosis in an adult, the possibility should be considered in the differential diagnosis.6
In a study of 1161 patients admitted to hospital for tuberculosis, the incidence of lymph node tuberculosis without pulmonary involvement was reported to be about 5.1% (60 patients). Of these, 1.3% (16) had isolated mediastinal lymphadenopathy.7 Mediastinal lymphadenopathy may occur as a complication of pulmonary tuberculosis or as a primary disease without pulmonary involvement. Tuberculous adenitis of the mediastinum manifests itself as dysphagia, stridor, acute respiratory distress, chest pain or perforation of the oesophagus or tracheobronchial tree.8
Paralysis of the recurrent laryngeal nerve caused by mediastinal lymphadenopathy due to tuberculosis is an extremely rare condition. We have come across just two published cases.9,10 Awareness of the occurrence of mediastinal tuberculous lymphadenopathy could lead to early diagnosis by bronchoscopy or thoracoscopy and early implementation of antitubercular chemotherapy. This would help to reduce the significant morbidity associated with mediastinal complications.
In our case, the diagnostic dilemma was compounded by the fact that the patient had previously been treated for T-cell acute lymphoblastic leukaemia.
1 Computed tomography scan of the thorax
 |
|
Contrast-enhanced image shows soft tissue density in the region of the aortopulmonary window corresponding with uptake of fluorodeoxyglucose F18. |
2 Positron emission tomography (PET) scan
 |
|
Fluorodeoxyglucose F18 PET scan showing uptake in the aortopulmonary lymph nodes. |
3 Biopsy specimen of aortopulmonary lymph node
Competing interests
None identified.
References
- Magrath I, Shanta V, Advani S, et al. Treatment of acute lymphoblastic leukaemia in countries with limited resources; lessons from use of a single protocol in India over a twenty year period [corrected]. Eur J Cancer 2005; 41: 1570-1583. 0_pgfId-1094167
- Vora A, Frost L, Goodeve A, et al. Late relapsing childhood lymphoblastic leukaemia. Blood 1998; 92: 2334-2337. 0_pgfId-1094174
- Ford AM, Fasching K, Panzer-Grümayer ER, et al. Origins of “late” relapse in childhood acute lymphoblastic leukemia with TEL-AML1 fusion genes. Blood 2001; 98: 558-564. 0_pgfId-1094181
- Hijiya N, Hudson MM, Lensing S, et al. Cumulative incidence of secondary neoplasms as a first event after childhood acute lymphoblastic leukemia. JAMA 2007; 297: 1207-1215. 0_pgfId-1094188
- Chang JM, Lee HJ, Goo JM, et al. False positive and false negative FDG-PET scans in various thoracic diseases. Korean J Radiol 2006; 7: 57-69. 0_pgfId-1094195
- Liu CI, Fields WR, Shaw CI. Tuberculous mediastinal lymphadenopathy in adults. Radiology 1978; 126: 369-371. 0_pgfId-1094205
- Geldmacher H, Taube C, Kroeger C, et al. Assessment of lymph node tuberculosis in Northern Germany: a clinical review. Chest 2002; 121: 1177-1182. 0_pgfId-1094212
- Venkateswaran RV, Barron DJ, Brawn WJ, et al. A forgotten old disease: mediastinal tuberculous lymphadenitis in children. Eur J Cardiothorac Surg 2005; 27: 401-404. 0_pgfId-1094219
- Meral M, Akgun M, Kaynar H, et al. Mediastinal lymphadenopathy due to mycobacterial infection. Jpn J Infect Dis 2004; 57: 124-126. 0_i1091852
- Kawasaki T, Gotoh T, Nakamura T, et al. [Tuberculous mediastinal lymphadenitis presenting as hoarseness] [Japanese]. Nihon Kyobu Shikkan Gakkai Zasshi 1996; 34: 1244-1248. 0_CBFGJJHG