





Volume 186 - Issue 9
Paediatric diabetes — which children can gain insulin independence?
Authors: Shubha Srinivasan and Kim C Donaghue
Med J Aust 2007; 186 (9): 436-437. || doi: 10.5694/j.1326-5377.2007.tb00991.x
Published online: 7 May 2007
Published online: 7 May 2007
Molecular genetics can facilitate a successful switch to oral diabetes therapy
The increase in type 1 and type 2 diabetes in childhood has been well documented worldwide and in Australia.1,2 In addition, the separate entity of monogenic diabetes is increasingly recognised in paediatric diabetes, and now encompasses neonatal diabetes mellitus and maturity onset diabetes of the young (MODY)3 (Box 1). Monogenic diabetes is defined as diabetes caused by a single gene defect. A diagnosis of monogenic diabetes should be considered in a child who is diabetes-associated-autoantibody negative, is diagnosed with diabetes in the first 6 months of life, has a parent with diabetes, and/or is not markedly obese. Although uncommon — its frequency is estimated to be 1%–3% of all childhood diabetes3 — the clinical relevance of this condition is that at least some of those affected (in particular, those with MODY1 and MODY3) can achieve very good diabetes control with sulfonylurea rather than insulin therapy.
Neonatal diabetes mellitus presents in the first 6 months of life with signs of hyperglycaemia — polyuria, dehydration, failure to thrive and, in many, frank diabetic ketoacidosis. Diabetic ketoacidosis is an important diagnosis to consider in an infant who presents critically unwell because the clinical picture may mimic sepsis. While the reported incidence of neonatal diabetes mellitus is one in 500 000 newborns,4 the estimated incidence is thought to be a lot higher, and it may be the cause of some unexplained infant deaths. About half of affected patients will have transient neonatal diabetes mellitus, where insulin treatment can be discontinued within a median of 3 months (although diabetes mellitus may recur in the second or third decade of life). In contrast, patients with permanent neonatal diabetes mellitus have, until recently, required insulin therapy for life. The revolution in patient management we describe here is due to molecular genetic analysis of the ATP-sensitive potassium (KATP) channel of the pancreatic beta cell (Box 2).
Sulfonylureas have traditionally been used to treat type 2 diabetes mellitus. They act by binding the sulfonylurea receptor (SUR1), which closes KATP channels, thereby stimulating endogenous insulin production from the pancreatic beta cell. Gloyn et al demonstrated that some patients with Kir6.2 potassium channel activating mutations secreted insulin in response to the intravenous sulfonylurea tolbutamide.5 Subsequently, the Neonatal Diabetes International Collaborative Group conducted a trial of glibenclamide, an oral sulfonylurea, in 49 patients with Kir6.2 mutations. This trial included two Australian centres, with three children — one white and two of Middle Eastern ethnicity. An impressive 90% of the trial patients were successfully switched from insulin to glibenclamide.8 Importantly, the responsiveness in vitro of mutant ATP channels to tolbutamide was proportionate to the patient’s response to glibenclamide. This enables a degree of predictability of whether a patient is likely to successfully switch from insulin to oral therapy.
Not only was oral therapy welcomed by families of patients, but the switch from insulin resulted in significant improvement of metabolic control, with glycated haemoglobin levels dropping from 8.1% to 6.4% after 12 weeks of treatment.8 Insulin response to oral glucose load was increased in those tested. Continuous glucose monitoring has also shown fewer fluctuations in postprandial glucose,9 which families report improves the child’s general wellbeing.
However, the story is not all rosy — some patients with Kir6.2 activating mutations known to have poor in-vitro response to tolbutamide may not be able to switch to oral therapy. It is therefore important to determine the exact genetic mutation involved, so that families can be counselled about the chances of a successful switch. In our experience, such counselling was helpful in lessening the disappointment when a 7-year-old girl with a Kir6.2 mutation, who had presented with ketoacidosis at 7 months of age, remained insulin-dependent despite maximal glibenclamide dose.
The diagnosis of neonatal diabetes mellitus should be considered in any critically ill infant, and the International Society for Pediatric and Adolescent Diabetes recommends that all infants who develop diabetes mellitus in the first 6 months of life be tested for a genetic mutation in the KATP channel.10 DNA from peripheral blood can be sent to a diabetes research laboratory in Exeter in the United Kingdom for testing (see http://www.diabetesgenes.org). To date, 20 Australian children, who had been insulin-dependent from less than 6 months of age, have been genotyped. Seven tested positive for mutations in Kir6.2 and three for mutations in SUR1 (Professor Andrew Hattersley, Peninsula Medical School, Exeter, UK, personal communication), and some have gained insulin independence.
While molecular genetics can now help classify and facilitate management of childhood diabetes, regardless of the type of diabetes (type 1, type 2, or monogenic), all children who present with severe fasting hyperglycaemia and ketoacidosis will initially require insulin therapy to reverse the metabolic abnormalities.
1 Classification of primary diabetes mellitus in children
Type 1 diabetes is characterised by the presence of diabetes-associated autoantibodies (islet cell, insulin, glutamic acid decarboxylase, and tyrosine phosphatase). A number of children with type 1 diabetes may be obese at diagnosis. Type 2 diabetes is characterised by obesity, negative antibodies and raised C-peptide levels. It is more common in non-white people than type 1 diabetes. Comorbid obesity can make the distinction between these two types of diabetes difficult. Monogenic diabetes is caused by a single gene abnormality. Maturity onset diabetes of the young (MODY) 1 and MODY3 are due to transcription factor mutations. Children with monogenic diabetes are not generally obese. Some children with monogenic diabetes present in the neonatal period with ketoacidosis.
2 Subunit structure of the ATP-sensitive potassium (KATP) channel of the pancreatic beta cell*
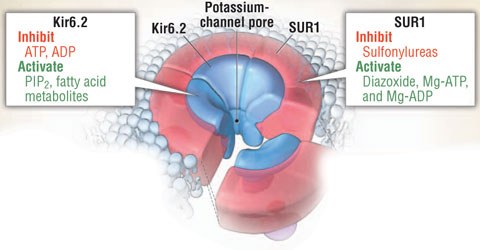
The KATP channel consists of four sulfonylurea receptor (SUR1) subunits and four potassium channel (Kir6.2) subunits. Closure of the KATP channel is required for glucose-stimulated insulin secretion from the pancreatic beta cell. Conversely, opening of the KATP channel inhibits insulin secretion. Inactivating mutations of genes encoding both SUR1 (ABCC8) and Kir6.2 (KCNJ11) subunits keep the channel closed and are known to cause uncontrolled insulin secretion, resulting in congenital hyperinsulinism.
It was hypothesised that activating mutations of these genes would keep the KATP channel open and cause permanent neonatal diabetes mellitus (PNDM). In 2004, Gloyn et al reported six novel heterozygous mutations in 10 of 29 patients with PNDM, including a 5-year-old Sydney girl who had been treated with insulin from 6 weeks of age.5 Subsequently, Proks et al reported a patient with activating mutations of ABCC8,6 and Babenko et al reported ABCC8 mutations in two of 29 patients with PNDM and seven of 44 patients with transient neonatal diabetes mellitus.7
KATP channels are also found in skeletal muscle and neurones throughout the brain, and some patients with Kir6.2 activating mutations have extrapancreatic features — motor skill and language delay, muscle contractures, epilepsy, and dysmorphic features — leading to the description of a new syndrome, known as DEND (Developmental delay, Epilepsy, Neonatal Diabetes) syndrome. In-vitro studies of mutant KATP channels have shown a correlation between the degree of KATP channel insensitivity and severity of the clinical phenotype.5
* Adapted from: Sperling MA. ATP-sensitive potassium channels — neonatal diabetes mellitus and beyond [editorial]. N Engl J Med 2006; 355: 507-510. PIP2 = phosphatidyl-inositol-4,5-bisphosphate.
References
- Taplin CE, Craig ME, Lloyd M, et al. The rising incidence of childhood type 1 diabetes in New South Wales, 1990–2002. Med J Aust 2005; 183: 243-246. 0_i1091841
- McMahon SK, Haynes A, Ratnam N, et al. Increase in type 2 diabetes in children and adolescents in Western Australia. Med J Aust 2004; 180: 459-461. 0_i1091843
- Craig ME, Hattersley A, Donaghue K; International Society for Pediatric and Adolescent Diabetes. ISPAD clinical practice consensus guidelines 2006–2007. Definition, epidemiology and classification. Pediatr Diabetes 2006; 7: 343-351. 0_i1091845
- von Muhlendahl KE, Herkenhoff H. Long-term course of neonatal diabetes. N Engl J Med 1995; 333: 704-708. 0_i1091847
- Gloyn AL, Pearson ER, Antcliff JF, et al. Activating mutations in the gene encoding the ATP-sensitive potassium-channel subunit Kir6.2 and permanent neonatal diabetes. N Engl J Med 2004; 350: 1838-1849. 0_i1091849
- Proks P, Arnold AL, Bruining J, et al. A heterozygous activating mutation in the sulphonylurea receptor SUR1 (ABCC8) causes neonatal diabetes. Hum Mol Genet 2006; 15: 1793-1800. 0_i1091851
- Babenko AP, Polak M, Cave H, et al. Activating mutations in the ABCC8 gene in neonatal diabetes mellitus. N Engl J Med 2006; 355: 456-466. 0_i1091853
- Pearson ER, Flechtner I, Njolstad PR, et al; Neonatal Diabetes International Collaborative Group. Switching from insulin to oral sulfonylureas in patients with diabetes due to Kir6.2 mutations. N Engl J Med 2006; 355: 467-477. 0_i1091855
- Zung A, Glaser B, Nimri R, Zadik Z. Glibenclamide treatment in permanent neonatal diabetes mellitus due to an activating mutation in Kir6.2. J Clin Endocrinol Metab 2004; 89: 5504-5507. 0_i1091857
- Hattersley A, Bruining J, Shield J, et al; International Society for Pediatric and Adolescent Diabetes. ISPAD clinical practice consensus guidelines 2006–2007. The diagnosis and management of monogenic diabetes in children. Pediatr Diabetes 2006; 7: 352-360. 0_i1091861