





Volume 181 - Issue 8
Electrocardiogram artefacts caused by an abdominal electrostimulator
Authors: Robert F Bonvini and Edoardo Camenzind
Med J Aust 2004; 181 (8): 455. || doi: 10.5694/j.1326-5377.2004.tb06377.x
Published online: 18 October 2004
Published online: 18 October 2004
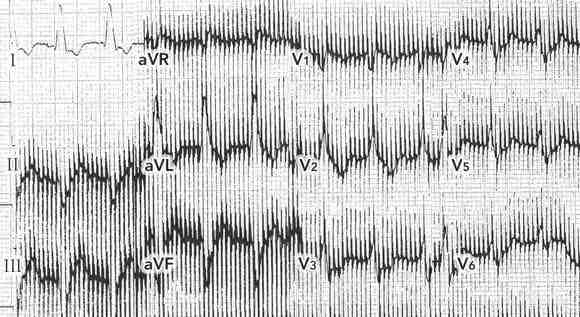
A 74-year-old woman presented to hospital with dyspnoea of sudden onset. She was in cardiogenic shock, with blood pressure of 90/50 mmHg, and pulse rate of 115 bpm. The electrocardiogram (ECG) was difficult to interpret because of severe, persistent and inexplicable artefacts (Box 1A). Chest x-ray showed acute pulmonary oedema thought secondary to left ventricular failure. Echocardiography showed a left ventricular ejection fraction of 40% and anterior akinesia. Coronary angiography confirmed a proximal occlusion of the left anterior descending coronary artery, which was successfully treated by direct angioplasty and stenting.
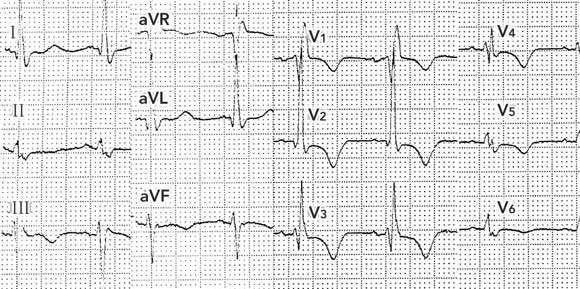
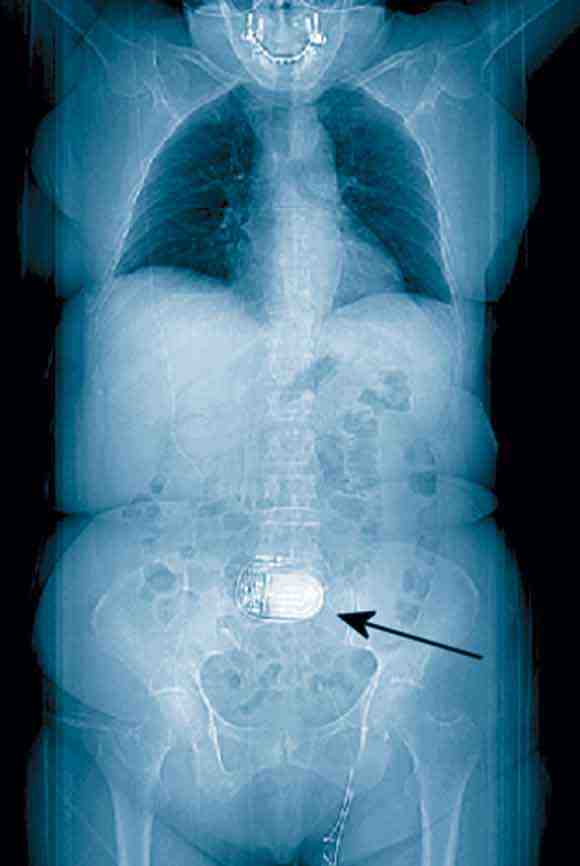
Review of the patient’s previous medical records revealed, on a thoracoabdominal image derived from computed tomography data, a foreign body in the central abdominal region (Box 2). Questioning of the patient after the angioplasty revealed that this was an electrostimulator (Itrel II, Medtronic, Minneapolis, USA) implanted a few years earlier as part of a dynamic graciloplasty to treat faecal incontinence. An ECG performed 12 hours after the angioplasty with the device deactivated (by the patient’s control programmer) produced an ECG tracing free of artefacts (Box 1B).
Persistent and inexplicable ECG artefacts should raise the suspicion of interference from a device generating high frequency electrical impulses. Such devices may include minute ventilation rate-responsive pacemakers1 and central or transcutaneous neurostimulators (eg, deep brain neurostimulators used in Parkinson’s disease,2 and spinal neurostimulators used in chronic back pain3). Occasionally, when the vector of impulses is perpendicular to an ECG lead, the tracing from that lead may be free of artefacts (eg,Box 1A, lead I).
Intrathoracic devices are usually discovered on physical examination or standard chest x-ray, but devices in other parts of the body may not be obvious. In dynamic graciloplasty to treat anal incontinence, the gracilis muscle is transposed around the anal canal and electronically stimulated by a device placed in a subcutaneous pocket in the abdominal wall.4 In our case, this device led to ECG artefacts potentially interfering with the ability to diagnose the acute myocardial infarction.
Implanted electrostimulation devices are being used increasingly in medicine and should be considered as a possible source of ECG artefacts, especially by frontline clinicians confronted daily with such life-threatening conditions as acute coronary syndromes.
References
- Southorn PA, Kamath GS, Vasdev GM, Hayes DL. Monitoring equipment induced tachycardia in patients with minute ventilation rate-responsive pacemakers. Br J Anaesth 2000; 84: 508-509.
- Martin WA, Camenzind E, Burkhard PR. ECG artifact due to deep brain stimulation. Lancet 2003; 361: 1431. i1085599
- Siddiqui MA, Khan IA. Differential electrocardiographic artifact from implanted spinal cord stimulator. Int J Cardiol 2003; 87: 307-309. i1085601
- Christiansen J, Rasmussen OO, Lindorff-Larsen K. Dynamic graciloplasty for severe anal incontinence. Br J Surg 1998; 85: 88-91. i1085603