





Volume 181 - Issue 1
Leading Australian doctors and clinical researchers set new priorities
Authors: Ruth M Armstrong, Helen M Randall and Martin B Van Der Weyden
Med J Aust 2004; 181 (1): 14-19. || doi: 10.5694/j.1326-5377.2004.tb06150.x
Published online: 5 July 2004
Published online: 5 July 2004
Even for nonagenarians, anniversaries are an opportunity for looking forward as well as looking back. Wondering what sort of articles the MJA might be publishing in the near future, and what might be the areas of focus and challenge for the medical profession, we asked over 40 of Australian medicine’s current opinion leaders:
“. . . what area in your discipline is not currently researched or not resourced [by conventional conservative funding bodies], but ought to be developed as it will yield dividends.”
In true editorial spirit, each contributor was asked to answer the question in less than 100 words, and to “think outside the square”.
The replies came in thick and fast and we can’t publish them in full in print. However, a number of themes emerged, within which we have grouped excerpts from contributors’ responses. (The full text from the contributors is available here)
Promising technologies


For complex reasons, medicine lags behind the rest of the world in its use of information technology, but several contributors say it’s time we caught up!
Information technology allows the “bedside" to be anywhere a mobile phone data signal can be received (photo courtesy m.Net Corporation).
Cameron (emergency medicine) believes that patient-held electronic health records would save lives. An unconscious patient is brought “lights and sirens” to the emergency department. “The ED team work feverishly to save the person’s life, knowing nothing of the past medical history, medications, allergies or advance directives”. Why aren’t we already using these “health cards”? “The technology exists but the political will and the resources do not.” Discussing anaesthetics, Kerridge was on the same wavelength. The current speed and complexity of inpatient care have increased the need for “rapid access to comprehensive patient and other information, and decision making in the face of uncertainty”. To ensure that care remains “safe and high-quality”, we need to develop both clinical information and decision-support systems.
Roberton (paediatrics) would like to see information technology used for research and policy development to ensure the wellbeing of children. The “singularly important need”, he believes, is “development and linkage of databases relevant to child health”. Databases to be linked might include those relating to perinatal statistics, mortality/morbidity data, immunisation records, health service utilisation and prescribing data, cancer databases, educational outcome assessments, and Australian Bureau of Statistics and Social Health Atlas information. While Roberton referred to his proposal as a “policy and funding challenge”, Scott, Braund and Ng (internal medicine) were bolder, entitling their contribution, “Stop funding laboratory benches. Start funding decision support and communication!”. As patients present with more and more comorbidities, we need mobile computers to provide real-world decision support at the bedside. Research findings should appear as “critically appraised evidence summaries and guidelines, accessible via desktop icons”. The justification for shifting our efforts to decision support? — “remembering to apply what’s known saves more lives than new knowledge”.
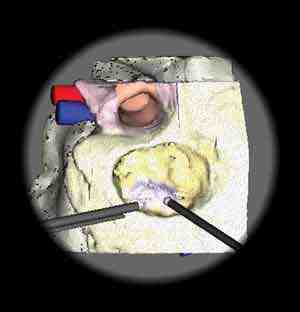
Computer-assisted knee-joint replacement surgery. A camera detects markers on the patient and the instruments, and transmits information to a computer monitor. Size, position and alignment can be computer modelled before surgical bone cuts, or selection of a definitive implant (photo courtesy Professor Peter Choong).
Contributors saw the computer age as a boon for the surgical specialties. According to Choong (orthopaedics), “the power of the computer will revolutionise, innovate, and enhance our understanding of what we do as surgeons”. Computer-assisted surgery in orthopaedics can improve surgical precision and accuracy. “While prosthetic implantation is a major beneficiary of computer-assisted surgery, so too is minimally invasive surgery, which will change not only how surgery is performed, but also the type of surgery possible, implant design, and patient outcomes.” O’Leary (ear, nose and throat surgery) finds the idea of virtual-reality surgical training exciting. “Immersed in a 3-D environment . . . trainee surgeons may one day be able to ‘see’ and ‘feel’ their virtual patient as they acquire skills in ear and nose surgery.” Improvements in safety, standardisation, access and quality control are reasons to develop this technology “now”.
Some contributors whose specialties use evolving technologies nominated areas of promise in their disciplines. Peters (radiation oncology) believes more research is needed on a new technique which uses “the single greatest attribute of radiation as a therapeutic tool — the accuracy and certainty with which a specified dose can be delivered to any site in the body.” The technique involves using targeted beams of radiation to activate toxic pro-drugs within tumour-bearing tissues. Meanwhile, Rowe (nuclear medicine) predicts an expanding role for positron emission tomography. “Over the next decade, PET will become routine, not only for cancer staging, but also for tailoring treatment. It will be used to assess early response, plan radiotherapy and, through the use of more specific tracers, will permit better treatment selection.”
Virtual ear surgery trainer developed by the University of Melbourne and the CSIRO (photo courtesy Associate Professor Stephen O'Leary, University of Melbourne, and CSIRO).
Two contributors commented on the way we use existing technology. Cicuttini (rheumatology) believes an area that has received little attention is the most cost-effective way to investigate common painful conditions. “As in many other areas of medicine, there has been a history of adding new investigations to the old ones, rather than substituting new for old.” She suggests the need for research on the rational use of investigations. For instance, does a patient with back pain still need a plain radiograph of the spine? Also ripe for research, says Cordner (forensic pathology), is the use of new imaging techniques at autopsy. He believes that this will lead to “improved characterisation of pathology, and, in some cases, improved decision making about the value of autopsy”.
Bringing into focus


A group of contributors suggested a new angle or a new focus for research in their specialties.
In the first two of these, the results of the research may also benefit other disciplines. Those dealing with inflammatory or immunological disease processes may well be interested in Marks’ (dermatology) suggestion that, instead of continuing to investigate what turns on the inflammatory/immunological response in atopic disease, we should be focusing on what turns off the response. O’Hehir (allergy and immunology), surprised by the escalating use of alternative therapies, wants not only clinical and laboratory research on alternative therapies, but also “well-conducted qualitative studies to determine motivations for their uptake”. These data might be useful in other disciplines.
Baby with atopic eczema. What turns off the inflammatory response? (photo courtesy Professor Robin Marks).
Chronic venous disease is the forgotten child of vascular surgery, says Myers, and the costs of treating varicose veins and their complications are enormous. We must understand the pathogenesis. “Do abnormal haemodynamics distend normal veins or do normal pressures distend abnormal veins? Intensive biochemical and cellular research is needed to devise biological mechanisms to retard varicose disease.”
In gastroenterology, there is a new subspecialty — neurogastroenterology. The gut is unique for the complexity of its intrinsic nervous system, says Hebbard. In 30%–50% of patients with disordered gastrointestinal function, no organic causes can be found. Research in neurogastroenterology is classifying the disorders; subclassifying patients by epidemiological, psychological and symptom analysis; measuring function by motor and sensory testing; and expanding understanding of the neurophysiology of the enteric system.
The deplorable state of the health of Aboriginal and Torres Strait Islander peoples troubled several contributors. After decades of research in the epidemiology of Indigenous health, says Anderson (Aboriginal health), the “research agenda needs to be refocused on the development and evaluation of interventions in clinical care and population health, and an investigation of systemic barriers to providing accessible and effective healthcare”. Marks (respiratory medicine) hypothesises that suppurative airway disease in Indigenous Australian children and adults, and obstructive lung disease in Indigenous adults, may have a common pathological pathway. He calls for research focusing on “understanding the respective roles of a pathogenic environment and compromised airway and mucosal defences”. There may be ancillary benefits for control of respiratory infectious diseases in the wider community.
House dust mite – a common cause of asthma and hayfever. What motivates people to seek out alternative remedies?
In renal medicine, research efforts and resources have concentrated on end-stage kidney disease, but Walker (renal medicine) says the focus has shifted to earlier kidney disease (proteinuria and/or impaired glomerular filtration rate), “which has assumed epidemic proportions, is a major cause of morbidity and mortality, and an independent and highly significant risk factor for a dramatically increased, all-causes cardiovascular disease mortality.” Funding is required for large-scale, intervention randomised-controlled trials.
Out of the vacuum
Many contributors expressed a desire to reconnect medicine with the person; a replacement of the reductionist approach by a more holistic view.
Kerridge (anaesthesia) called for a shift from “small studies using surrogate endpoints, such as physiological or biochemical changes”, to “large, multicentre trials which examine common ‘simple’ interventions in ‘normal’ patient care”, measuring “ ‘real’ outcomes such as mortality, morbidity, or length of stay.” Cameron (rehabilitation medicine) was similarly minded, citing a need for research to “. . . understand better what will improve life for people with disability in the long term through careful epidemiological studies and clinical trials, looking particularly at appropriate environmental and personal factors”. At the same time he saw a need to reorient healthcare services to provide “rehabilitation with a community focus”. Mendelson (radiology) says imaging specialists have been slow to take up the challenge of measuring the effects of their craft on patient outcomes and quality of life. For instance, “Does the detection of ‘incidentalomas’ benefit the patient or just cause anxiety, expense and morbidity? Does recurrent imaging of patients receiving palliative therapy for malignancy confer any benefit?” These are questions which need to be considered in this era of expensive and limited technology.
Connecting with the community

Several contributors saw the need to begin taking patient and community preferences into account. Scott, Braund and Ng (internal medicine) applied this to research: “Meta-analyses of effectiveness address the physician’s perspective. Patients need meta-analyses of the downside (risk) as well.” Others, such as Maddern (surgery), see it as imperative that we live up to community expectations to be “competent, up-to-date and able to achieve world-class results”. In doing this, he says, surgical research will need to be able to demonstrate not only that procedures are effective in the short term, but to show “long-term results in terms of cure or function within communities”. The establishment of optimal training environments (so surgeons and their teams can master the necessary skills before treating patients), ongoing national audit of surgeons, hospitals and operative approaches, and corrective systems are important if we are to achieve these results.
Then there is a need for greater understanding of community values and societal pressures. Harris (general practice) points out that, while GPs can offer patients more options than ever before, “our patients are increasingly sceptical and misinformed (especially by the media and Internet)”. He believes we need more research on “how much Australian GPs and their patients agree on management or what factors or supports can make agreement easier or harder to achieve”.
Wodak sees community values as creating tension in the area of drugs and alcohol as “the irresistible obstacle of community abhorrence of illicit drugs opposes the irresistible force of demand for these drugs”. The future should see us looking for compromises. Similar to the current acceptability of methadone, he suggests we need to develop “some form of regulated supply of orally well-absorbed, dilute and mild opiates, stimulants and hallucinogens” which are “reasonably acceptable to both the drug-abhorring majority and the drug-seeking minority”.
Compassion and a need to research and resource ways to improve quality of life were also emphasised by some. Cordner (forensic medicine) sees a need to provide resources to “consult families about autopsy (eg, tissue retention for transplantation, research or diagnosis) and provide them with its results”. Meanwhile, in developing countries, the lack of appropriate expertise in detecting human rights abuses has led to “community mistrust of the criminal justice system, and therefore continuing instability and poverty”. These countries require aid to train forensic physicians and pathologists. In palliative care, Currow believes we should provide care for the caregivers through “. . . information, emotional support and respite that is responsive and funded”. Furthermore, palliative-care services should be judged on the carers’ outcomes, including “the ability to have health, create a life without the person for whom they have cared, and achieve a level of function with which they are satisfied”.
Even our opinion leader in the world of health informatics regarded the human and systemic factors as being as important as the IT infrastructure. Coiera describes the computer as “the sacred ground in health informatics research”. This includes multiple information systems, such as the electronic health record, the Internet and mobile computing. However, he adds that “the profane ground, largely ignored, is the broader human system that is needed to make anything actually work. Technological systems repeatedly fail for cultural and organisational reasons”. The focus now needs to be on fusing the human and technical elements into effective systems.
The da Vinci robot for radical prostatectomy. Brilliant advance or expensive toy? (© 2004 Intuitive Surgical, Inc).
Hirst (urology) takes a broader cultural and societal view, saying that “the last 30 years has seen a significant shift in medicine from a moral economy to an increasingly market-based economy”. Several forces, such as pharmaceutical, instrument and device manufacturers and competitive behaviour within the profession, contribute to this. The shift has had most impact on procedural specialties like urology, and we need to take steps to ensure that its impact on quality, cost and training is positive.
Age shall not weary us
Not surprisingly, several contributions acknowledged the implications for future clinical practice of the “greying” of the Australian population.
Flicker (geriatric medicine) is concerned about the dire lack of evidence to guide the management of people in advanced old age, and wants to see “evaluation of multicomponent interventions for the many coexisting diseases in old people with reduced physiological reserves”. Dobb (intensive care) was similarly concerned: as the cohort of elderly people is growing, so is our ability to ensure survival after severe illness. “We need to target intensive care to the patients who will truly benefit”, which requires understanding more about “the effects of age, comorbidities and functional status on recovery from severe illness”.

The dilemma of the upper-age entry limit (70 years) for clinical trials in cancer therapy — and that half the patients with cancer are now aged over 70 at diagnosis — was raised by Fox (medical oncology). “There is insufficient evidence-based data to guide management of ageing patients. We need to recognise that cancer will be predominantly a disease of the aged, and investigate it and manage it as such.” Constable (ophthalmology) reminds us about the epidemic of age-related macular degeneration. While Australian research has contributed to the epidemiology of macular degeneration, we know little about genetic predisposition and biological determinants. “Cellular biology, genetic manipulation, transplantation and induction of animal models will accelerate our understanding, create intellectual property and result in an early interventional approach.”
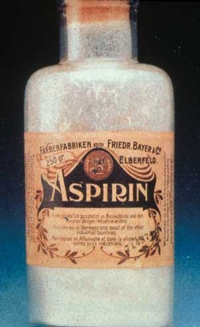
Tonkin (cardiology) takes the bull by the horns and suggests “a public-interest trial: aspirin for primary cardiovascular prevention in the elderly.” The rationale? Previous trials mostly involved middle-aged males, and the risk of bleeding increases with age. At present, only a third of Australians 70 years and over, including those with overt disease, take aspirin routinely. “Aspirin is cheap and equitable; it may be extraordinarily cost-effective; and it may also prevent cognitive decline, depression and cancer.” There is a drawback — “with few gains for industry, this trial appears unfundable — 20 500 subjects, 5 years’ follow-up, $35 million!” How about it, Bill and Melinda?
Finally, Flicker points out that we still need to establish “which mix of lifestyle, health and social activities would maximise our chances of ageing well, an outcome which is not simply the absence of disease”.
Connections between silos
One of the biggest changes in medicine since the MJA was born 90 years ago is ever-increasing subspecialisation. Some contributors saw a need to broaden the knowledge base of their disciplines.
Sawyer, Sanci and Patton (adolescent health) say young people’s health problems are complex, but that the responses to problems such as depression, chronic physical illness, eating disorders and obesity often draw on “too narrow a skill-set from single-discipline practitioners who claim clinical expertise and responsibility”. More effective clinical, research and training responses will require “broader engagement of the health system and other sectors”.
Wesselingh also sees a need for “adequately resourced, multidisciplinary responses” in the field of infectious diseases. Despite the extraordinary success and high profile of Australian infectious diseases research, he identifies three significant failures that warrant a multidisciplinary approach. “Firstly, our Aboriginal communities still suffer from excessive infection-related morbidity; secondly, our hospitals remain environments with a significant risk of acquiring infection with a multiresistant organism; and, thirdly, the Asia-Pacific region is following Africa towards an HIV/AIDS- and TB-led catastrophe.”
In considering burns care, Wood (plastic surgery) believes we need a multidisciplinary scientific approach “to ensure the quality of the scar is worth the pain of survival”. This approach has potential for dealing with the three management steps: assessment (using multimodality imaging, including confocal microscopy and synchrotron technology); debridement (combining autolytic and image-guided physical debridement techniques); and reconstruction (using nanotechnology to provide the framework for appropriate tissue regeneration).
The new genetics
As genetics is a newer “basic science” discipline, contributors called for more integration with clinical research and practice. Waring (molecular genetics) notes that the availability of genetic tests for many diseases, such as inherited neurological and cardiovascular conditions and cancer, has created strong clinical demand. There is now “an urgent need to build integrated clinical and laboratory genetic infrastructure and to train scientists, pathologists and clinicians in molecular genetics”. Also required are a national strategy and a funding model for molecular genetics.
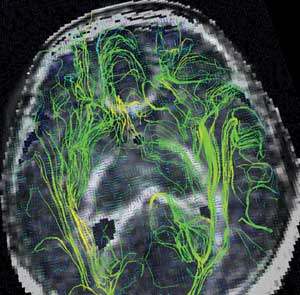
Understanding how the brain works. MRI, showing brain fibre tracks in an infant with brain injury (photo courtesy Professor Terrie Inder).
Williamson (genetics) says that “the Human Genome Project has given lots of data on genes of known function, and we know about single-gene diseases caused by their mutations. However, two-thirds of our genes are still a mystery”. Where are these genes? Mostly in the brain, he says, where genetic and environmental factors interact to produce “brain function, intelligence, consciousness, values and culture”. Williamson’s wish is for a project which integrates the Human Genome Project, neurogenetics, psychology, MRI fetal imaging and artificial intelligence “so we can really understand how the brain works”.
Wiley (haematology) believes we now have “a major opportunity to explore genetic risk factors for pathogens which, in some people, survive and flourish in our intracellular environment”. Pathogens such as mycobacteria, chlamydia, toxoplasma and leishmania are killed by macrophages of the innate immune system, following similar pathways, but we are not sure which genetic factors in the host predispose to these diseases. “Studies which bridge haematology, immunology and infectious diseases are much needed to define genetic defects in innate immunity.”
Just do it!
A sense of urgency pervaded several of the contributions.
“The world desperately needs an HIV vaccine”, says Kent (HIV medicine). “How can this slippery virus be checkmated? Where is its Achilles heel? What cells can be manipulated to exploit any weaknesses? What is the innate immune system doing? Can we generate an immune barrier to resistant strains? History will judge our dedication to this task.”
Driscoll (occupational health) sees an urgent imperative for research into “establishing links between occupational exposure and disease, preferably at a stage early enough to modify the disease process”. We also need “better understanding of health risks (and benefits) associated with the large-scale transfer of jobs from heavy industry to information and service industries”. Mindel (sexual health) says there is an urgent need to control the commonest bacterial sexually transmitted infection in Australia. “Chlamydia is a leading cause of infertility and a significant drain on the public purse.” A national strategy is needed to encourage yearly screening of sexually active adults under 25 years (with a suitable urine chlamydia test), with treatment of those infected and their contacts, supplemented by promotion of consistent condom use, and testing and treatment for other STIs.
For Mitchell (psychiatry) it is time to “grasp the nettle”. We now have new investigatory tools (genetic markers, structural and functional brain imaging), and have “rediscovered” gene–environment interactions (gene variants that increase the risk of mental illness, but only in conjunction with environmental factors). Thus, “the time is ripe for funding of large-scale, longitudinal studies to examine the roles and contributions of these factors combined (and in isolation) in determining the development and timing of onset of the major mental illnesses — schizophrenia, bipolar disorder and depression. Potential benefits in understanding aetiology, and thereby designing ‘tailored’ therapies, are enormous.”
Leeder (public health) also takes a “just do it” attitude. He quotes Jeffrey Sachs, Director of the Earth Institute at Columbia University (New York), who says public health is “whatever it takes to improve the public’s health”. And what are the imperatives in public health? “Developing a robust ethic for public health; inviting private enterprise, unions, insurers and the public to the public health table; and learning the skills to speak eloquently with these people. Whatever it takes!”
A doubling in prevalence of type 2 diabetes in Australia since 1980 means we simply can’t wait 10–15 years to do conventional research studies, says Chisholm (endocrinology). Intensive interventions (modified diet plus physical activity) can dramatically reduce diabetes incidence in predisposed people, but are prohibitively costly for whole communities. “To combat diabetes, obesity and cardiovascular disease, Australia should immediately implement ‘best-guess’ measures with progressive research analysis and modification (as was done to reduce cigarette smoking).”
In short, let’s just do it! The future belongs to those who dare!
Contributors: A/Prof Ian P Anderson, Dr Wilton Braund, Prof Ian D Cameron, Prof Peter A Cameron, Prof Donald J Chisholm, Prof Peter F M Choong, A/Prof Flavia M Cicuttini, Prof Enrico W Coiera, Prof Ian J Constable, Prof Stephen M Cordner, Prof David C Currow, Dr Geoffrey J Dobb, Dr Tim Driscoll, Prof Leon A Flicker, Prof Richard M Fox, Prof Mark F Harris, Dr Geoffrey S Hebbard, Dr Geoffrey H L Hirst, A/Prof Stephen J Kent, Dr Ross K Kerridge, Prof Stephen R Leeder, Prof Guy J Maddern, Dr Guy B Marks, Prof Robin Marks, A/Prof Richard M Mendelson, Prof Adrian Mindel, Prof Philip B Mitchell, Prof Kenneth A Myers, Dr Kenneth Ng, Prof Robyn E O’Hehir, A/Prof Stephen J O'Leary, Prof George Patton, Prof Lester J Peters, Prof Donal M Roberton, Dr Christopher C Rowe, Dr Lena A Sanci, Prof Susan Sawyer, A/Prof Ian A Scott, Prof Andrew M Tonkin, A/Prof Rowan G Walker, A/Prof Peter Waring, Prof Steve L Wesselingh, Prof James S Wiley, Prof Robert Williamson, Dr Alex D Wodak, Prof Fiona M Wood.