





Volume 178 - Issue 8
Muir–Torre syndrome and early detection of internal malignancy
Authors: Celia S Chen, Lindy Loweinstein, Shyamala C Huilgol, Dinesh Selva and Craig James
Med J Aust 2003; 178 (8): 368. || doi: 10.5694/j.1326-5377.2003.tb05251.x
Published online: 21 April 2003
Published online: 21 April 2003
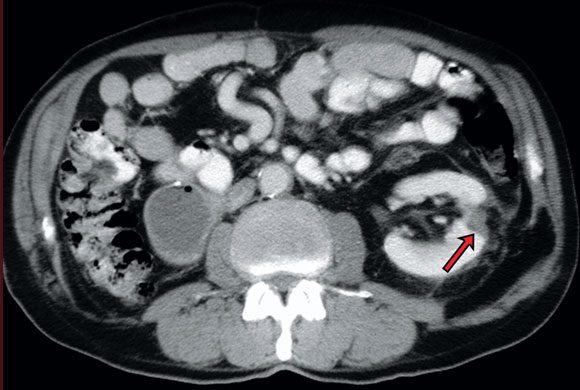
A 71-year-old man with a past history of right-sided, renal cell carcinoma presented with a recurrent, right upper eyelid lesion (Box, Figure A). The initial biopsy showed Bowen's disease, but review after Mohs micrographic surgery revealed focal sebaceous differentiation suggestive of in-situ sebaceous carcinoma. A diagnosis of Muir–Torre syndrome was suspected, and the patient was referred for genetic counselling and targeted cancer surveillance. This led to the discovery of multiple dysplastic colonic adenomas and a left renal cell carcinoma (Box, Figure B).
Muir–Torre syndrome is an autosomal-dominant genodermatosis characterised by cutaneous sebaceous neoplasia and one or more visceral malignancies. Diagnostic criteria include at least one sebaceous gland adenoma, epithelioma, or carcinoma, and at least one internal malignancy. The diagnosis of sebaceous carcinoma can be difficult, particularly in the periocular region, where it often masquerades clinically as blepharoconjunctivitis or recurrent chalazia. Furthermore, sebaceous carcinoma often displays only focal differentiation and, as seen in our patient, may be histologically misdiagnosed as squamous-cell or basal-cell carcinoma. A history of internal malignancy in patients presenting with sebaceous gland carcinoma should raise the possibility of Muir–Torre syndrome. Correct diagnosis in this case enabled early detection of dysplastic colonic polyps and renal cell carcinoma.

References
- Cohen PR, Kohn SR, Davis DA, Kurzrock R. Muir–Torre syndrome. Dermatol Clin 1995; 13: 79-89.
- Hussein MR, Wood GS. Microsatellite instability and its relevance to cutaneous tumorigenesis. J Cutan Pathol 2002; 29: 257-267.
- Loeffler M, Hornblass A. Characteristics and behaviour of eyelid carcinoma (basal cell, squamous cell, sebaceous gland and malignant melanoma). Ophthal Surg 1990; 21: 513-518.