





Volume 178 - Issue 12
Update on treatment of menstrual disorders
Authors: Martha Hickey and Cynthia M Farquhar
Med J Aust 2003; 178 (12): 625-629. || doi: 10.5694/j.1326-5377.2003.tb05388.x
Published online: 16 June 2003
Published online: 16 June 2003
Abstract
There is evidence from well designed randomised controlled trials that modern medical and conservative surgical therapies (including endometrial ablation) are effective treatments for heavy menstrual bleeding for many women.
Submucous fibroids may be resected directly via the hysteroscope, reducing menstrual bleeding, although data are available only from case series.
Endometriosis is common, may also occur in young women and may present with atypical or non-cyclical symptoms; conservative laparoscopic surgery increases fecundity and reduces dysmenorrhoea and dyspareunia.
Randomised trials of the levonorgestrel intrauterine system in women with menorrhagia have shown that hysterectomy can be avoided in 80% of cases, and that this system is an effective therapy for menorrhagia.
The levonorgestrel intrauterine system may also be useful for managing symptoms of endometriosis, adenomyosis and endometrial hyperplasia, based on observational data.
Disturbances of menstrual bleeding are a major social and medical problem for women, their families and the health services, and a common reason for women to consult their general practitioners or gynaecologists. In the United Kingdom, each year one in 20 women consult their GPs about heavy menstrual bleeding.1
Heavy bleeding is the most common menstrual complaint. In most cases, this has no identifiable pelvic or systemic cause and is termed dysfunctional uterine bleeding. Irregular dysfunctional uterine bleeding is generally associated with anovulation. Historically, many women with heavy menstrual bleeding were advised to undergo hysterectomy, which was the only way of ensuring a "cure". However, a range of new and effective interventions can now be offered for dysfunctional uterine bleeding and other common causes of menstrual disorder, such as fibroids and endometriosis. These interventions may reduce bleeding and pain to acceptable levels and will induce amenorrhoea in some women.
We present case studies comparing the "traditional" approaches to common menstrual disorders with more recent developments.
Case 1 — Dysfunctional uterine bleeding
Presentation: A 39-year-old overweight woman presented with regular heavy menstrual bleeding. She had had three caesarean sections and a laparoscopic sterilisation. An ultrasound examination revealed a normal-sized uterus and irregular, thickened endometrium. The ovaries appeared normal.
Management: Traditional management might have included a trial of medical therapy, such as luteal-phase progestins. If this failed or was not acceptable to the patient, the next step was often an abdominal hysterectomy, as few other effective treatments were available. Current management would include hysteroscopy or saline infusion sonography to rule out submucous fibroids or large polyps, which may contribute to heavy bleeding. Subsequent treatment options include insertion of a levonorgestrel-releasing intrauterine system or endometrial ablation.
In this case, outpatient hysteroscopy revealed a normal uterine cavity and, after earlier counselling about likely disturbances in menstrual bleeding patterns, a levonorgestrel-releasing intrauterine system (20 μg/24 h) was inserted.
Intrauterine progestin therapy
Oral luteal-phase progestins may help regulate bleeding patterns in irregular bleeding secondary to anovulatory cycles but are ineffective in regular dysfunctional uterine bleeding and may actually increase menstrual bleeding.2,3 Longer regimens (Days 5–25 of the menstrual cycle) have been found to have similar effectiveness to the levonorgestrel intrauterine system in dysfunctional uterine bleeding when compared in a randomised controlled trial, but their acceptability is poor, with only 30% of patients reporting that they would have the treatment again.3
Intrauterine administration of progestins, as in the levonorgestrel-releasing intrauterine system, results in higher endometrial concentrations of progestin compared with oral administration, but relatively little systemic absorption. The Mirena system (Schering) releases 20 μg of levonorgestrel/24 h and, in women with ovulatory dysfunctional uterine bleeding, has been shown to produce an 86% reduction in objectively measured menstrual blood loss at 3 months and a 97% reduction at 12 months, with amenorrhoea in 50% of women at 12 months. This effect continues over a 5-year period.4 In addition, limited data from small case series suggest that this system may also be an excellent treatment for endometrial hyperplasia of most grades, and may thus be helpful in anovulatory dysfunctional uterine bleeding.5
A disadvantage of intrauterine progestin therapy is erratic vaginal bleeding or spotting, particularly during the early months of use, and women need to be warned that these disruptions may occur but are likely to improve and do not represent treatment failure. Mirena also offers highly effective contraception and rapid reversibility.
Continuation rates for Mirena vary, partly depending on the indication (treatment of heavy bleeding or contraception). A study of 250 women who used Mirena for contraception found 66% continuation at 2 years, with most removals in the first 6 months because of irregular bleeding.6 When Mirena is used to treat menorrhagia, continuation rates may be up to 80% at 1 year.7 In a randomised trial in which women awaiting hysterectomy received either Mirena or no treatment, 68% elected to continue with Mirena at 1 year,8 while 20% elected to undergo hysterectomy. Cost–benefit analysis showed that Mirena was three times cheaper than hysterectomy. Endometrial biopsy or hysteroscopy is not required routinely before Mirena insertion and should be carried out only if there are other clinical indications.
Endometrial ablation
Endometrial ablation is a minimally invasive therapy for dysfunctional uterine bleeding that preserves the uterus and is suitable for women who have completed childbearing. Many techniques have been developed. The first generation techniques (laser, transcervical resection of the endometrium and rollerball) require visualisation of the uterus with a hysteroscope and, although safe, require skilled surgeons.
New techniques have been introduced recently with the aim of providing simpler, quicker, safer and more effective procedures that can be used in outpatient settings. These include cryoablation, hydrothermal ablation (through irrigation with hot saline solution), heated balloon systems, diode laser hyperthermy, microwave ablation, thermal radiofrequency ablation, and photodynamic therapy (intrauterine light delivery).
Most women are satisfied with the reduction in bleeding after endometrial ablation, but an estimated 20% require further surgery, and 10% eventually undergo hysterectomy. Factors associated with negative outcomes include increasing uterine size, young age, fibroids, adenomyosis and failure to thin the endometrium with agents such as gonadotropin-releasing hormone (GnRH) agonists before the procedure.9,10
Counselling should include the fact that amenorrhoea cannot be guaranteed and that this surgery is not contraceptive, but that subsequent pregnancy may be dangerous for both mother and fetus.
It is also important to recognise that many of these techniques are still under development and investigation, and that "blind" therapies have the potential to cause unrecognised uterine damage. Overall, evidence suggests that success rates and complication profiles of most of the newer ablation techniques compare favourably with first generation methods.11 However, very few randomised controlled trials have assessed their efficacy, safety and acceptability.
Case 2 — Menorrhagia and fibroids
Presentation: A 45-year-old nulliparous woman presented with increasingly heavy menstrual bleeding and pain associated with the passage of clots. A trial of medical therapy with a non-steroidal anti-inflammatory drug had failed. Transvaginal ultrasound revealed a fibroid uterus with one 3 cm intramural fibroid, one 2 cm subserous fibroid, and a distorted endometrial cavity suggesting a submucous fibroid.
Management: Traditional management would probably have included an early resort to major abdominal surgery, such as abdominal hysterectomy or myomectomy. A newer approach is clear identification of the position of the fibroids in relation to the endometrial cavity, followed by removal of the submucous fibroids using hysteroscopic techniques with possible endometrial resection.
In this case, saline infusion sonohysterography confirmed the presence of a submucous fibroid. This was resected hysteroscopically under general anaesthesia, leading to a substantial reduction in menstrual bleeding and a reduction in dysmenorrhoea.
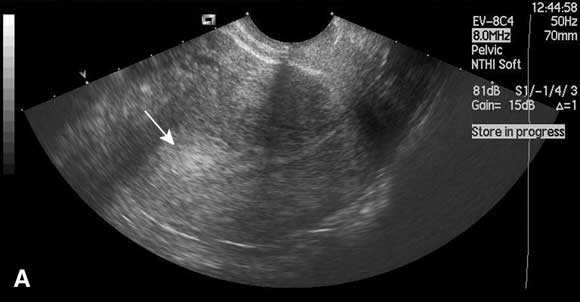
Saline infusion sonohysterography
In this technique, saline is instilled transcervically into the uterine cavity to distend the uterus and increase contrast, and the cavity is visualised using ultrasound (Box). Saline infusion sonohysterography is more accurate than transvaginal ultrasound alone in diagnosing submucous fibroids and endometrial polyps in women with abnormal uterine bleeding,12 and can be performed in the outpatient clinic. An alternative form of imaging is diagnostic hysteroscopy, but this is invasive and often performed under general anaesthesia. Use of saline infusion sonohysterography has been shown to reduce the need for diagnostic hysteroscopy.13
Hysteroscopic resection of fibroids
Submucous fibroids seem to be more commonly associated with menorrhagia than other uterine myomas, and their removal appears to substantially improve menstrual symptoms.14 However, hysteroscopic resection of submucous fibroids is unlikely to influence subsequent fibroid growth or symptoms associated with remaining myomas.
Conventional hysteroscopic resection of submucous fibroids requires general anaesthesia. Future prospects include outpatient removal of fibroids with devices such as the operating bipolar microhysteroscope. This device vaporises lesions through diathermy; it can operate in a saline environment, and its small size means it can be used without cervical dilatation, thereby allowing intervention to be combined with diagnostic hysteroscopy.
Endometrial ablation
Microwave endometrial ablation has also been shown to be effective for the management of heavy menstrual bleeding associated with both submucous and intramural fibroids, providing they are less than 5 cm in diameter.15 Hydrothermal endometrial ablation may also be effective in the presence of fibroids.
Embolisation
Embolisation of symptomatic uterine fibroids is an alternative to surgical myomectomy. It has been widely used in the last 5–10 years and is well accepted by patients and apparently successful in reducing fibroid size and ameliorating symptoms in some.16 Embolisation may avert the need for hysterectomy for some women with symptomatic uterine fibroids.17 However, the relative benefits of embolisation and myomectomy have not yet been tested in a prospective randomised study, and embolisation has been associated with serious side effects, such as infection, bowel obstruction and loss of ovarian function.18 There is also concern about the integrity of areas embolised during any subsequent pregnancies.
Fertility
There is potential for newer techniques to preserve or restore fertility, but their place has not yet been established. A trial is underway in the United Kingdom comparing the relative effects of embolisation and myomectomy on fertility, but results will not be available for several years.
Medical therapies for menorrhagia
Aside from intrauterine progestin therapy there have been few new medical therapies for dysfunctional uterine bleeding. Intrauterine progestin therapy can be used for heavy menstrual bleeding associated with uterine fibroids, but there is some evidence that expulsion rates may be increased in the presence of submucous fibroids.19 However, the success of medical therapy can be optimised by accurate clinical selection of patients and use of the most effective methods.
Tranexamic acid is an antifibrinolytic agent which significantly reduces heavy menstrual bleeding, by an average of 110 mL per cycle,20 and is more effective than mefenamic acid and ethamsylate for objectively measured menorrhagia.21 However, there has been a reluctance to prescribe tranexamic acid because of possible side effects, such as increased risk of thrombogenic disease (deep venous thrombosis). Long-term studies in Sweden failed to demonstrate any increase in thrombosis in women using tranexamic acid above that in the general population.22
Prostaglandin synthetase inhibitors, such as mefenamic acid, taken during menstruation may decrease bleeding by an average of 124 mL per cycle,20 and have the added advantage of relieving dysmenorrhoea.23
Case 3 — Endometriosis
Presentation: A 26-year-old woman presented with a history of dysmenorrhoea since menarche and perimenstrual pain on passing bowel motions. She had never been pregnant and had been sexually active for 2 years without using contraception. She had recently been prescribed the oral contraceptive pill, with only a minor reduction in symptoms.
Management: In the past, this patient might have been diagnosed with primary "spasmodic" dysmenorrhoea and not further investigated. The presence of bowel symptoms may have led to a diagnosis of irritable bowel syndrome. It should be recognised that these symptoms may represent endometriosis, even in a young woman. A new approach would include transvaginal ultrasound examination to rule out ovarian abnormality followed by laparoscopic surgery or medical therapy, depending on the reason for treatment (infertility or pain) and the severity of symptoms.
In this case, ultrasound examination revealed bilateral ovarian masses suggestive of endometriomas. This was confirmed at laparoscopy, which demonstrated extensive endometriosis (score, III–IV on the American Fertility Society scale) with obliteration of the pouch of Douglas. Laparoscopic removal of endometriomas and excision of deep endometriosis was performed, leading to a reduction in dysmenorrhoea and bowel symptoms, which was maintained at 6 months. However, future recurrence is likely.
Improvements in diagnosis
Traditional gynaecological teaching held that endometriosis was a condition of late reproductive life. It is increasingly acknowledged that endometriosis is also common in teenagers and younger women, and that this diagnosis must be considered in premenopausal women with persistent dysmenorrhoea, dyspareunia and bowel symptoms. In addition, some women with endometriosis present with symptoms that are atypical or non-cyclical. In women with dysmenorrhoea, the incidence of endometriosis ranges from 40% to 60%, and in women with subfertility it ranges from 20% to 30%.24 Diagnosis in this group is often delayed, resulting in prolonged and poorly controlled symptoms.
Conservative laparoscopic surgery
A traditional surgical approach is laparoscopic removal of superficial endometriosis by techniques such as diathermy or laser ablation. More recently, complete removal of all visible endometriosis, including deep endometriosis and nodules, has been advocated, with stripping of the peritoneum if necessary.25 Both approaches are conservative in that they preserve the uterus and ovaries.
There is increasing evidence from randomised controlled trials that conservative laparoscopic surgery for endometriosis, especially when it is complete, increases fecundity and reduces disease-related symptoms, such as dysmenorrhoea and dyspareunia.26,27 However, there is a substantial risk of some symptoms persisting and of recurrence or exacerbation within 6 months.28,29
The combination of laparoscopic laser ablation and adhesiolysis has been demonstrated in a case series to be beneficial for pelvic pain associated with minimal, mild and moderate endometriosis over a 1-year follow-up period.30
Medical therapy
Traditional medical therapy for endometriosis has included danazol, oral progestins and GnRH analogues. These drugs do not enhance fertility but may be helpful in some patients to relieve symptoms and prevent their recurrence, either alone or in combination with surgery. However, there is little good evidence to support use of medical therapy, with few randomised placebo-controlled trials, and many questions remain unanswered. It is unclear how long treatment should continue and what the long-term effects are, and this information is likely to be difficult to obtain. Although ovarian suppression with GnRH analogues relieves symptoms of endometriosis, it is necessary to "add back" hormone replacement therapy to prevent bone demineralisation if they are given for more than 6 months.31 No clear differences have been shown between the above drugs except in adverse events.32
There is preliminary evidence from case series that the levonorgestrel-releasing intrauterine system may reduce the size of rectovaginal endometriotic deposits and alleviate pain,26 and that it may be a suitable therapy for symptomatic endometriosis and adenomyosis. While this system will not help women desiring pregnancy, it offers an exciting possibility for the future medical treatment of endometriosis.
Future developments
Possible future developments in management of menstrual disorders include improved understanding of the mechanisms of menstrual disturbance and the factors that control the establishment and progression of endometriosis. In the latter condition, specific therapies directed at molecular targets regulating the growth of ectopic endometrium are a possibility. Similarly, improved understanding of the molecular and genetic factors controlling fibroid growth may lead to targeted therapies to prevent or limit their proliferation.
In addition, new roles for established therapies, such as the levonorgestrel-releasing intrauterine system, are still being explored, including the treatment of symptomatic endometriosis and endometrial hyperplasia. The management of one of the most common complaints in women's health, menstrual disorders, is likely to continue to improve over the coming years.

Competing interests
None identified.
References
- Vessey M, Villard-Mackintosh L, McPherson K, et al. The epidemiology of hysterectomy: findings in a large cohort study. Br J Obstet Gynaecol 1992; 99: 402-407. i1082626
- Preston JT, Cameron IT, Adams EJ, Smith SK. Comparative study of tranexamic acid and norethisterone in the treatment of ovulatory menorrhagia. Br J Obstet Gynaecol 1995; 102: 401-406. i1082628
- Irvine GA, Campbell-Brown MB, Lumsden MA, et al. Randomised comparative trial of the levonorgestrel intrauterine system and norethisterone for treatment of idiopathic menorrhagia. Br J Obstet Gynaecol 1998; 105: 592-598. i1082630
- Anderson JK, Rybo G. The levonorgestrel releasing intra-uterine contraceptive device in the treatment of menorrhagia. Br J Obstet Gynaecol 1990; 97: 690-694. i1082632
- Perino A, Quartararo P, Catinella E, et al. Treatment of endometrial hyperplasia with levonorgestrel releasing intrauterine devices. Acta Eur Fertil 1987; 18: 137-140. i1082634
- Hidalgo M, Bahamondes L, Perrotti M, et al. Bleeding patterns and clinical performance of the levonorgestrel-releasing intrauterine system (Mirena) up to two years. Contraception 2002; 65: 129-132. i1082636
- Monteiro I, Bahamondes L, Diaz J, et al. Therapeutic use of levonorgestrel-releasing intrauterine system in women with menorrhagia: a pilot study (1). Contraception 2002; 65: 325-328. i1082638
- Hurskainen R, Teperi J, Rissanen P, et al. Quality of life and cost-effectiveness of levonorgestrel-releasing intrauterine system versus hysterectomy for treatment of menorrhagia: a randomised trial. Lancet 2001; 357: 273-277. i1082640
- O'Connor H, Magos A. Long-term results of endometrial resection. J Am Assoc Gynecol Laparosc 1996; 3 (4 Suppl): S35. i1082642
- Sowter MC, Lethaby A, Singla AA. Pre-operative endometrial thinning agents before endometrial destruction for heavy menstrual bleeding. Cochrane Database Syst Rev 2002; 3: CD001124. i1082644
- Lethaby A, Hickey M. Endometrial destruction techniques for heavy menstrual bleeding: a Cochrane review. Hum Reprod 2002; 17: 2795. i1082646
- Nanda S, Chadha N, Sen J, Sangwan K. Transvaginal sonography and saline infusion sonohysterography in the evaluation of abnormal uterine bleeding. Aust N Z J Obstet Gynaecol 2002; 42: 530-534. i1082648
- De Vries L, Dijkhuizen FP, Mol BW, et al. Comparison of transvaginal sonography, saline infusion sonography, and hysteroscopy in premenopausal women with abnormal uterine bleeding. J Clin Ultrasound 2000; 28: 217-223. i1082650
- Vercellini P, Zaina B, Yaylayan L, et al. Hysteroscopic myomectomy: long-term effects on menstrual pattern and fertility. Obstet Gynecol 1999; 94: 341-347. i1082652
- Cooper KG, Bain C, Parkin DE. Comparison of microwave endometrial ablation and transcervical resection of the endometrium for treatment of heavy menstrual loss: a randomised trial. Lancet 1999; 354: 1859-1863. i1082654
- Pron G, Bennett J, Common A, et al. Ontario Uterine Fibroid Embolization Collaboration Group.The Ontario Uterine Fibroid Embolization Trial. Part 2. Uterine fibroid reduction and symptom relief after uterine artery embolization for fibroids. Fertil Steril 2003; 79: 120-127. i1082656
- Pinto I, Chimeno P, Romo A, et al. Uterine fibroids: uterine artery embolization versus abdominal hysterectomy for treatment — a prospective, randomized, and controlled clinical trial. Radiology 2003; 226: 425-431. i1082658
- Payne JF, Haney AF. Serious complications of uterine artery embolization for conservative treatment of fibroids. Fertil Steril 2003; 79: 128-131. i1082660
- Ikomi A, Pepra EF. Efficacy of the levonorgestrel intrauterine system in treating menorrhagia: actualities and ambiguities. J Fam Plann Reprod Health Care 2002; 28: 99-100. i1082662
- Lethaby A, Farquhar C, Cooke I. Antifibrinolytics for heavy menstrual bleeding. Cochrane Database Syst Rev 2000; 4: CD000249. i1082664
- Bonnar J, Sheppard BL. Treatment of menorrhagia during menstruation: randomised controlled trial of ethamsylate, mefenamic acid, and tranexamic acid. BMJ 1996; 313: 579-582. i1082666
- Lindoff C, Rybo G, Astedt B. Treatment with tranexamic acid during pregnancy, and the risk of thrombo-embolic complications. Thromb Haemost 1993; 70: 238-240. i1082668
- Fraser IS, Pearce C, Shearman RP, et al. Efficacy of mefanamic acid in patients with a complaint of menorrhagia. Obstet Gynecol 1981; 58: 543-551. i1082670
- Farquhar CM. Extracts from the "clinical evidence". Endometriosis. BMJ 2000; 320: 1449-1452. i1082672
- Donnez J, Squifflet J, Pirard C, et al. The efficacy of medical and surgical treatment of endometriosis-related infertility and pelvic pain. Gynecol Obstet Invest 2002; 54 Suppl 1: 2-10. i1082674
- Jacobson TZ, Barlow DH, Garry R, Koninckx PR. Laparoscopic surgery for pelvic pain associated with endometriosis. Cochrane Database Syst Rev 2001; 4: CD001300. i1082676
- Jacobson TZ, Barlow DH, Koninckx PR, et al. Laparoscopic surgery for subfertility associated with endometriosis (Cochrane review). The Cochrane Library, Issue 1, 2003. Oxford: Update Software. i1082678
- Ghezzi F, Beretta P, Franchi M, et al. Recurrence of ovarian endometriosis and anatomical location of the primary lesion. Fertil Steril 2001; 75: 136-140. i1082680
- Jones KD, Sutton CJ. Recurrence of chocolate cysts after laparoscopic ablation. J Am Assoc Gynecol Laparosc 2002; 9: 315-320. i1082682
- Tokushige M, Suginami H, Taniguchi F, Kitaoka Y. Laparoscopic surgery for endometriosis: a long-term follow-up. J Obstet Gynaecol Res 2000; 26: 409-416. i1082684
- Surrey ES, Hornstein MD. Prolonged GnRH agonist and add-back therapy for symptomatic endometriosis: long-term follow-up. Obstet Gynecol 2002; 99 (5 Pt 1): 709-719. i1082686
- Farquhar C, Sutton C. The evidence for the management of endometriosis. Curr Opin Obstet Gynecol 1998; 10: 321-332. i1082688