





Volume 176 - Issue 3
Emergency endovascular stent-graft repair for thoracic aortic injury
Authors: Julian A Hanson, D Mark Brooks and Jai S Raman
Med J Aust 2002; 176 (3): 111-112. || doi: 10.5694/j.1326-5377.2002.tb04316.x
Published online: 4 February 2002
Published online: 4 February 2002
Thoracic aorta injury secondary to blunt chest trauma accounts for 10% to 20% of fatalities from high-velocity accidents, and the subsequent mortality rate in untreated survivors is high.1 Standard management is based on prompt radiological diagnosis and surgical repair by thoracotomy, usually with partial left heart bypass. Despite technical advances, these procedures carry significant mortality and postoperative paraplegia rates (up to 30% and 10%, respectively),2 and severe traumatic comorbidity or coincidental chest disease in many patients makes their aortic injury inoperable.
Endovascular stent-graft repair is emerging as an alternative for treating thoracic aortic injury, with a number of potential advantages.3,4 These include the ability to treat patients with contraindications to thoracotomy, and the potential to reduce neurological complications. However, clinical experience with this procedure is limited.
The procedure involves deploying a self-expanding, fabric-covered metal stent from within the diseased vessel to exclude an aneurysmal segment, and is performed by means of a dedicated delivery system retrogradely inserted through the femoral artery. We report a case of immediate stent-graft repair of a traumatic false aneurysm of the thoracic aorta in a patient for whom thoracotomy was relatively contraindicated. We also review the published data and discuss technical issues.
Clinical record
A 47-year-old professional motorcyclist was thrown from his bike against a rubber tyre wall at high speed. He did not lose consciousness, but immediately noticed low back pain and lower-limb tingling. His vital signs were stable, and he was transferred to the trauma unit with full spinal precautions. Subsequent evaluation showed a pulse rate of 65 beats per minute, blood pressure of 150/65 mmHg, 30 respirations per minute, and a Glasgow Coma Score of 15. He had absent left knee and ankle jerks, reduced light touch sensation in L2–S1 dermatomes on the left and L2–L3 on the right, with normal power and anal tone. Chest and spine radiographs showed an abnormal mediastinal contour consistent with haemorrhage, and a fracture-dislocation of the lumbar spine at the L2–L3 level. Computed tomography (CT) angiography showed thoracic aortic injury with intimal flap and false aneurysm of the proximal descending aorta.
We felt that turning the patient to the lateral thoracotomy position for conventional surgical repair would risk further neurological deficit. Therefore, after discussing therapeutic options with the patient and his family, emergency endovascular stent-graft repair of the thoracic aortic injury was performed (see Box for technical details). CT angiography confirmed absence of extraluminal flow after the procedure. The patient subsequently underwent fixation of the lumbar spine injury using posterior rods, pedicle screws and bone graft. He made a complete neurological recovery. Three days after stent-graft insertion, he underwent video-assisted thoracoscopic evaluation of the left side of the chest for drainage of a large haemoserous pleural effusion. The thoracic aortic contour was normal, with minimal peri-aortic haematoma. Repeat CT angiography at six and 12 months confirmed thrombosis of the false aneurysm, with no complication related to the stent-graft repair, and the patient remains well 18 months after the injury.
Discussion
A number of centres have published encouraging initial results for elective endovascular stent-graft repair of chronic thoracic aortic aneurysms, usually related to atherosclerosis or chronic dissection.4-7 The largest study, of more than 100 patients, reported an initial technical success rate (aneurysm thrombosis) of 85%, one-month mortality of 10% and morbidity of 30%, and two-year actuarial survival of 70%.4 Stent-graft repair has been used to treat established traumatic thoracic aortic aneurysms,8,9 but there are few reports of immediate stent-graft repair of thoracic aortic injury.10-12
This case demonstrates the feasibility of emergency endovascular stent-graft repair for thoracic aortic injury. Stent-graft repair is an option for patients who are unable to undergo thoracotomy because of associated injuries or pre-existing chest disease. The endovascular strategy may reduce early surgical morbidity. In particular, the minimal requirement for anticoagulation and avoiding aortic cross-clamping may lower the risks of cerebral haemorrhage and paraplegia.2 For our patient with coincidental spinal injury, stent-graft repair minimised the chance of neurological deterioration secondary to lateral positioning for thoracotomy.
Continuing improvements in devices and delivery systems are likely to increase the familiarity, ease of use and availability of "off-the-shelf" thoracic aortic stent-graft systems. However, the role of emergency endovascular repair of thoracic aortic injuries requires further clarification. Medium-term follow-up data for endovascular repair of chronic thoracic aortic aneurysms suggest a small incidence of endoleak, delayed rupture and paraplegia,4,13 but very limited information is available for traumatic false aneurysms. In particular, the role of stent-graft repair in the context of intensive medical management of thoracic aortic injury needs to be defined.14
Stent-graft deployment technique
The diameter of the isthmic (26 mm) and descending (24 mm) thoracic aorta and the longitudinal extent of intimal injury were determined from computed tomography, and an appropriately sized "off-the-shelf" stent-graft (Zenith, 28 mm diameter, 120 mm length, Cook Australia) was obtained.
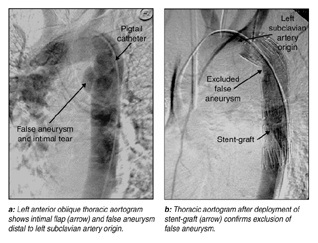
The procedure was performed with the patient in the supine position in the angiography suite under general anaesthesia, commencing eight hours after the accident. Diagnostic aortography via the right common femoral artery confirmed a transverse intimal tear 2 cm distal and opposite to the left subclavian artery origin (Figure a). Formal left common femoral arteriotomy was performed, followed by placement of the stent-graft device within its 24 F delivery system to the aortic arch over a stiff Lunderquist guide wire (Cook Australia).
Precise proximal positioning of the device was aided by intermittent angiography of the left subclavian artery origin using a 4 F Omni-flush catheter (Angiodynamics, USA) inserted via the left brachial artery. (In this case there was sufficient length of normal isthmic aorta to achieve a seal with the proximal stent-graft without compromising the left subclavian artery origin. Where there is insufficient distance it may be necessary to position the stent-graft across the subclavian artery origin, and to perform left carotid to distal subclavian bypass at a later stage should ischaemic symptoms ensue.) The self-expanding stent-graft was deployed in stages to allow recoil of the Z-stent sections to accommodate the inner radius of curvature of the aortic arch.
Optimal apposition of the proximal stent-graft was achieved with secondary dilatation ("moulding") using a compliant latex balloon (Cook Australia), resulting in successful exclusion of the false aneurysm, and patency of the subclavian artery (Figure b).
Competing interests
None declared.
References
- Patel NH, Stephens KE, Mirvis SE, et al. Imaging of acute thoracic aortic injury due to blunt trauma: A review. Radiology 1998; 209: 335-348. CACIJAEI
- Fabian TC, Richardson JD, Croce MA, et al. Prospective study of blunt aortic injury: Multicenter trial of the American Association for the Surgery of Trauma. J Trauma 1997; 42: 374-380. i1064030
- Reidy JF, Taylor P. The use of stent-grafts in thoracic aortic disease. Cardiovasc Intervent Radiol 2000; 23: 249-251. i1064032
- Mitchell RS, Miller DC, Dake MD, et al. Thoracic aortic aneurysm repair with an endovascular stent graft: the "first generation". Ann Thorac Surg 1999; 67: 1971-1974. i1064034
- Kawaguchi S, Ishimaru S, Shimazaki T, et al. Clinical results of endovascular stent graft repair for fifty cases of thoracic aortic aneurysms. Jap J Thoracic Cardiovasc Surg 1998; 46: 971-975. pgfId-1064036
- Nienaber CA, Fattori R, Lund G, et al. Nonsurgical reconstruction of thoracic aortic dissection by stent-graft placement. N Engl J Med 1999; 340: 1539-1545. pgfId-1064037
- Grabenwoger M, Hutschala D, Ehrlich MP, et al. Thoracic aortic aneurysms: treatment with endovascular self-expandable stent grafts. Ann Thoracic Surg 2000; 69: 441-445. i1064038
- Kato N, Dake MD, Miller DC, et al. Traumatic thoracic aortic aneurysm: treatment with endovascular stent-grafts. Radiology 1997; 205: 657-662. i1064040
- Rousseau H, Soula P, Perreault P, et al. Delayed treatment of traumatic rupture of the thoracic aorta with endoluminal covered stent. Circulation 1999; 99: 498-504. i1064042
- Fujikawa T, Yukioka T, Ishimaru S, et al. Endovascular stent grafting for the treatment of blunt thoracic aortic injury. J Trauma 2001; 50: 223-229. i1064044
- Bruninx G, Wery D, Dubois E, et al. Emergency endovascular treatment of an acute traumatic rupture of the thoracic aorta complicated by a distal low-flow syndrome. Cardiovasc Intervent Radiol 1999; 22: 515-518. pgfId-1064046
- Lagattolla N, Matson M, Self G, et al. Traumatic rupture of the aortic arch treated by stent grafting. Eur J Vasc Endovasc Surg 1999; 17: 84-86. i1064047
- Kasirajan K, Dolmatch B, Ouriel K, Clair D. Delayed onset of ascending paralysis after thoracic aortic stent graft deployment. J Vasc Surg 2000; 31: 196-199. i1064049
- Galli R, Pacini D, Di Bartolomeo R, et al. Surgical indications and timing of repair of traumatic ruptures of the thoracic aorta. Ann Thorac Surg 1998; 65: 461-464. i1064051