





Volume 168 - Issue 8
Panic disorder: coronary spasm as a basis for cardiac risk?
Authors: Virginia M Mansour, Garry L Jennings, Rosemary G Schwarz, Jane M Thompson and Murray D Esler
Med J Aust 1998; 168 (8): 390-392.
Published online: 20 April 1998
Published online: 20 April 1998
Panic disorder: coronary spasm as a basis for cardiac risk?
Virginia M Mansour, Dominic J C Wilkinson, Garry L Jennings,
Rosemary
G Schwarz, Jane M Thompson and Murray D Esler
For editorial comment see Freedman & Tennant
Patients with panic disorder often complain of angina-like chest
pain during panic attacks, but this is not usually considered
life-threatening. We describe three patients with panic disorder
and documented cardiac ischaemia during episodes of chest pain. In
two, it progressed to myocardial infarction. As none had
atherosclerosis evident at coronary angiography, the mechanism was
presumed to be coronary artery spasm. These cases illustrate that
pain typical of angina during panic attacks may have an organic cause.
(MJA 1998: 168; 390-392)
Introduction -
Case records -
Discussion -
Acknowledgement -
References -
Authors' details
-
-
©MJA1998
Introduction |
Panic disorder is characterised by unpredictable and overwhelming
feelings of fear accompanied by various symptoms of sympathetic
nervous system arousal, such as sweating, palpitations, diarrhoea,
and tremor.1 Often,
angina-like chest pain is also present, but detailed cardiac
"workup" in patients with panic disorder typically shows no
abnormalities.
Thus, although panic disorder is distressing and disabling, it has not been thought life-threatening. However, recent well conducted, prospective epidemiological studies show substantially increased risk of myocardial infarction and sudden death in patients with panic disorder (three- to six-fold increase).2,3 These patients sit at the crossroads of cardiology and neuropsychiatry, and provide a clinical model for investigation of the relationship between stress and heart disease. The mechanism by which cardiac risk is increased in panic disorder is not known, but has been thought to involve activation of the sympathetic nerves of the heart, predisposing to ventricular arrhythmias. We present three patients with panic disorder and chest pain whose cases suggest coronary artery spasm as a pos sible mechanism. |
Case records | All three patients met the diagnostic criteria for panic disorder of the Diagnostic and statistical manual of mental disorders (4th edition),4 and all were non-smokers. |
Patient 1 |
A 34-year-old woman presented to a hospital casualty department in
November 1996 with severe chest pain radiating to her left arm and
shortness of breath after having taken cocaine. She also complained
of palpitations, dizziness, tremor, and an overwhelming sense of
doom and fear. She had taken cocaine occasionally over the previous
two years without panic symptoms. An electrocardiogram (ECG) showed
inferolateral ST-segment depression suggesting ischaemia. The
pain eased with sublingual nitroglycerine and intramuscular
morphine. A thallium exercise stress test two weeks later gave normal
results.
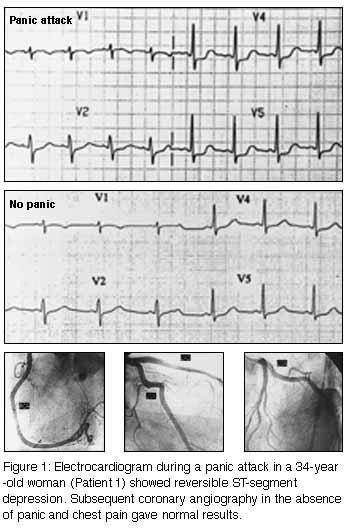
The patient presented again a month later with recurrent episodes of severe chest pain accompanying panic attack symptoms. She had stopped using cocaine after the first panic attack. An ECG taken during persisting pain again showed inferolateral ST-segment depression (Figure 1, below). Serum creatine kinase (CK) levels were normal. Coronary angiography during subsequent hospital admission (when the patient was free of pain) showed a normal coronary arterial tree (Figure 1). The patient was prescribed the selective serotonin reuptake inhibitor paroxetine (20 mg, increasing to 40 mg, daily), low dose aspirin (100 mg daily) and alprazolam (0.5 mg daily). Over two months' follow-up, panic attacks were less frequent, but chest pain recurred with each. After the addition of the slow calcium-channel blocker amlodipine (5 mg daily), her infrequent panic attacks were pain-free. |
Patient 2 |
A 42-year-old woman suffered anteroseptal infarction in November
1996 after exercise. Although she had no antecedent panic attack, she
had a nine-year history of panic disorder, with panic attacks
commonly associated with chest pain. She had been jogging as usual
that morning without any symptoms, and presented later in the day with
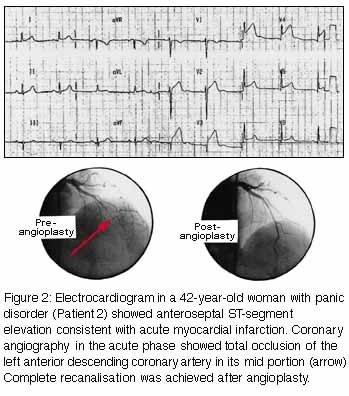
chest tightness and left-arm pain. A 12-lead ECG (Figure 2, below) showed anteroseptal ST-segment
elevation consistent with acute myocardial infarction. Acute
coronary angiography (Figure 2) showed
total occlusion of the left anterior descending coronary artery in
its mid portion.
Treatment with balloon angioplasty and abciximab (an inhibitor of platelet aggregation) achieved complete recanalisation, and the pain resolved. No atherosclerosis was evident in the coronary arterial tree. Although a vasodilator was not given during angiography, the treating cardiologist described the angiogram as indicating development of fresh thrombus at a site of spasm in an otherwise normal coronary artery. Low dose aspirin and amlodipine (5 mg daily) were prescribed. The patient had further panic attacks (without chest pain) until paroxetine (20 mg daily) was also prescribed. |
Patient 3 |
A 46-year-old man presented to a casualty department in October 1996
with severe chest pain during a panic attack. He had long-standing
panic disorder and a 15-year history of mild essential hypertension
treated by propranolol (40 mg daily). His ECG was normal in the
casualty department, and he was not admitted. The chest pain failed to
resolve over the next 10 hours and he attended his family doctor, who
found a raised serum CK level and arranged urgent hospital admission.
His serum CK level rose progressively in hospital, peaking at 518 U/L
(normal range [NR], 0-130 U/L), with CK MB isoenzyme level 66 U/L (NR,
0-10 U/L), leading to a diagnosis of myocardial infarction. Coronary
angiography 14 days later, when the patient was free of pain, gave
normal results, with no evidence of atherosclerosis.
Over the ensuing eight months, the patient had increasingly frequent panic attacks accompanied by angina-like pain. He was prescribed paroxetine (20 mg, increasing to 40 mg, daily) and alprazolam (0.5 mg daily). Although the panic attacks became less frequent when the daily paroxetine dose was increased to 40 mg, chest pain persisted until amlodipine (5 mg daily) and aspirin (100 mg daily) were added to the regimen. |
Discussion |
These three patients with panic disorder had otherwise inexplicable
episodes of cardiac ischaemia. In all three, the panic attacks were
typically accompanied by chest pain. In two, the documented
ischaemic events (angina with ST-segment depression in one and
myocardial infarction in the other) occurred during a panic attack.
In the third, while myocardial infarction was associated with
exercise rather than a panic attack, there was a long prior history of
panic attacks with chest pain. None of the three had atherosclerosis
evident on coronary angiography, and two were women with no classical
cardiac risk factors. Coronary artery spasm was thought to be the
underlying mechanism of the ischaemia in all three cases.
In some circumstances, patients with primary cardiac arrhythmias can be misdiagnosed as having panic disorder.5 Similarly, it might perhaps be argued that our patients had variant angina, with the anxiety disorder developing after a period of misdiagnosis of the cause of the chest pain, so that the myocardial ischaemia was a cause rather than a consequence of the panic disorder. However, in Patients 2 and 3 the diagnosis of panic disorder antedated the development of chest pain during panic attacks, while in Patient 1 angina-like pain was a feature of the first and of most subsequent panic attacks. The mechanism by which coronary spasm develops in panic disorder is not clear. Cigarette smoking can underlie coronary spasm, but our three patients were non-smokers. Hyperventilation, often a concomitant of a panic attack, can precipitate coronary spasm in the presence of atheroma6 and even in coronary arteries free of atherosclerosis.7 Patients who had spontaneous panic attacks in the research laboratory have shown a substantial increase in adrenaline secretion and sympathetic nervous system activity. 8 However, adrenaline typically increases, rather than decreases, coronary blood flow by means of b -adrenergic coronary vasodilatation.9 Similarly, sympathetic nervous system stimulation usually causes coronary vasodilatation and increases flow, partly through the attendant metabolic myocardial stimulation, but also through direct effects on the vasculature.9 In some circumstances, disorders of coronary vasomotion have been linked to dysfunction of the vascular endothelium. Endothelial function was not assessed in our patients, but such tests would be relevant for future prospective studies given that the mechanism of presumed spasm remains elusive. We suspect that coronary spasm is not uncommon during panic attacks, particularly in patients with typical angina-like pain, and that panic disorder may be an undetected cause of otherwise inexplicable coronary heart disease, especially in premenopausal women, who are otherwise at low cardiac risk. It may possibly overlap clinically with "Syndrome X", a poorly understood condition in which recurrent myocardial ischaemia occurs despite the presence of structurally normal coronary arteries. This condition, not to be confused with the endocrinological Syndrome X (insulin metabolic resistance syndrome),11 seems to result, not from coronary spasm, but from reduced myocardial flow reserve caused by a functional abnormality in the cardiac microcirculation.10 Formal testing involving measurements of coronary blood flow under conditions which increase it reflexly, such as exercise, would be needed to exclude this syndrome. An understanding of the mechanism of coronary spasm in panic disorder would facilitate therapeutic intervention. At present, we treat patients with panic disorder and clinical evidence of coronary spasm with drugs and other measures aimed at preventing or minimising their panic attacks,1 a slow calcium-channel blocker as a non-specific antispasm measure, and low dose aspirin as prophylaxis against coronary thrombosis during spasm. It is difficult to know how far to pursue cardiac testing in patients with panic disorder. As we believe their level of cardiac risk is low overall, we recommend selective investigation of those with typical angina-like pain during panic attacks. Capturing ECG evidence of myocardial ischaemia during a panic attack, either during clinic or emergency department attendance or on Holter monitoring, is of central clinical relevance. While it is important to exclude the presence of fixed coronary artery stenosis (which may coexist, particularly in older patients), standard provocative ischaemia testing is not entirely satisfactory; exercise or vasodilator pharmacological challenges are inappropriate for behaviourally induced ischaemia. Panic attacks can be induced in some patients by breathing a mixture of carbon dioxide (10%-15%) and oxygen.12 ECG or thallium stress testing using this stimulus as a challenge is worth future research evaluation. Panic disorder may provide a useful clinical model for studying the possible link between stress and heart disease. A direct relationship between mental stress and sudden death has been seen in special circumstances, such as inherited long-QT-interval syndromes, in which there is electrical instability of the heart muscle.13 In addition, rates of non-traumatic sudden death were markedly increased in people with underlying coronary disease during the 1994 Los Angeles earthquake.14 However, research on stress and heart disease has been hampered by disagreement over what constitutes stress and how to measure it. In panic disorder, the episodes of recurring, often inexplicable, anxiety can be regarded as repeated mental stress reactions. The study of cardiac risk during panic attacks may be a valid method for testing the general proposition that the clinical endpoints of ischaemic heart disease can be "triggered" by stressful events. |
Acknowledgement | This work was supported by a Project Grant from the National Heart Foundation of Australia and an Institute Grant to the Baker Medical Research Institute from the National Health and Medical Research Council of Australia. The contributions of Dr David Prior and Sister Leonie Johnston in the research cardiac catheter laboratory are gratefully acknowledged. The authors also wish to thank Dr Emmanuel G Manolas for provision, through the Epworth Hospital, of clinical and angiographic findings on his patient. |
References |
(Received 28 Aug 1997, accepted 21 Jan 1998) |
Authors' details
Baker Medical Research Institute, Melbourne, VIC.Virginia M Mansour, MB BS, Clinical Research Associate;
Jane M Thompson, MB BS, Clinical Research Associate;
Murray D Esler, PhD, FRACP, Associate Director.
Melbourne University, Melbourne, VIC.
Dominic J C Wilkinson, BMedSci, Medical Student.
Alfred Hospital Heart Centre, Melbourne, VIC.
Garry L Jennings, MD, FRACP, Director.
Medical Advisory Committee, The Melbourne Clinic, Melbourne, VIC.
Rosemary G Schwarz, FRANZCP, Chair.
Reprints: Professor M D Esler, Human Neurotransmitter Research
Laboratory, Baker Medical Research Institute, PO Box 348, Prahran,
VIC 3181.
E-mail: Esler AT Baker.edu.au
Readers may print a single copy for personal use. No further
reproduction or distribution of the articles
should proceed without the permission of the publisher. For
permission, contact the
Australasian Medical Publishing Company
Journalists are welcome to write news stories based on what they read here, but should acknowledge their source as "an article published on the Internet by The Medical Journal of Australia <http://www.mja.com.au>".
<URL: http://www.mja.com.au/>