




Knee pain and functional impairment, frequently related to osteoarthritis (OA) of the knee, is increasing in prevalence and severity in association with the ageing of our population.1,2 For milder OA, the mainstay of therapy is conservative, with physical therapy, simple analgesia and self-management strategies.3 The appropriate use of surgical interventions, such as arthroscopy, has been debated.4
In 2002, Moseley and colleagues conducted a randomised placebo-controlled trial (RCT) comparing arthroscopic debridement and arthroscopic lavage with placebo surgery in 180 patients with OA of the knee. They found no difference in self-reported pain and function over a 24-month follow-up period.5 Similarly, in 2008, Kirkley and colleagues found no significant benefit for arthroscopy in measures of pain, stiffness or physical function in their RCT. It compared arthroscopic debridement and lavage combined with medical and physical therapy, with medical and physical therapy alone, in 92 patients with moderate to severe knee pain from OA.6
The most recent systematic review on this topic identified 18 studies examining the effectiveness of arthroscopy, and reported limited evidence for the use of arthroscopy as a treatment for OA of the knee.7 However, only one study had evidence rated as level I. A 2008 Cochrane systematic review identified three studies and concluded that arthroscopy provided no benefit for patients with undiscriminated OA.8 The findings refuting the effectiveness of arthroscopy in patients with OA have been questioned, as the studies tend to be small, lack generalisability and have other methodological limitations.9,10
Despite the evidence questioning the use of arthroscopies in the absence of major mechanical derangement, reports suggest that use of these procedures may be increasing over time in the United Kingdom and United States.11,12 No studies have been published that have examined the usage patterns of knee arthroscopy in Australia.
A retrospective, longitudinal cohort study was conducted, using routinely collected hospital admissions data in Victoria.13
The Victorian Admitted Episodes Dataset (VAED) is maintained by the Victorian Government Department of Health and includes all hospital episode data compiled by public and private hospitals, including day procedure units.14
We obtained data on all patients aged 20 years and older with a hospital discharge during the study period, for whom the episode included the clinical specialty codes for orthopaedics and rheumatology (Box 1). Patients were excluded if their hospital admission was categorised as an emergency admission (2.2%).
The patient characteristics of age, sex, marital status, country of birth, duration of stay and hospital type were generated from VAED variables. Patient comorbidities were defined using the published algorithms for the Charlson comorbidity index groups.15,16 They incorporated a look-back period through any admission 1 year before the admission involving the arthroscopy.17
Each patient’s statistical local area of residence at their time of admission was linked to Socio-Economic Indexes for Areas (SEIFA) data. Tertiles of the economic resource index and the education and occupation index (two of four area-based measures of socioeconomic status) were used. The education and occupation index includes measures such as the proportion of people with a higher qualification or those employed in a skilled occupation. The economic resources index includes measures of income, housing expenditure and household assets.18 The statistical local areas that could not be linked to the SEIFA datasets due to missing values (17.7% of cases) were imputed to the median value. In sensitivity analyses, we imputed the lowest value, and this did not alter our estimates of the effect.
Our outcome of interest was change in the rate of arthroscopies across the study period, defined as the number of arthroscopies by financial year, offset by the volume of patients receiving any elective orthopaedic procedure identified from the VAED in the same financial year. We determined that elective orthopaedic volume would be a more accurate offset variable than the Victorian population, based on exploratory analysis of the data. Exploratory analysis confirmed that elective orthopaedic procedure volume for other orthopaedic procedures (eg, arthroplasty) greatly exceeded population growth when adjusted for age, sex and financial year. Thus, we concluded that the increase in orthopaedic procedure volume over the past decade is likely to be driven by other increasing pressures beyond population growth, such as an increasing burden of disease, changing referral patterns and patient preferences.19
We chose the 2000–01 financial year as our reference value for assessing changes during the study period. We also examined changes in relation to the period July 2002 – June 2004, after publication of the Moseley study demonstrating a lack of benefit for knee arthroscopies in patients with OA of the knee.5
Due to overdispersion of the data,20 negative binomial regression was used to analyse the number of arthroscopic procedures occurring in each financial year, adjusted for factors identified as potential confounders. Confounders were identified through clinical opinion and bivariate analysis (assessed for a significant relationship with the outcome [P < 0.05]).
There was a total of 807 030 elective orthopaedic admissions in 256 hospitals during the study period. This included 159 528 patients having 190 881 admissions identified as involving a knee arthroscopic procedure in 123 hospitals (low orthopaedic volume, 44.5%; medium, 32.5%; high, 23.0%) (Box 2). Most arthroscopies occurred in private hospitals (73.6%) among patients aged 40–59 years (44.1%). Most patients had few comorbidities recorded, with diabetes (3.3%), cancer (1.2%) and chronic lung disease (1.2%) the most common. Most admissions were same-day patients (78.7% in public hospitals and 74.6% in private hospitals). Limb laterality of procedure is not documented in the VAED; however, 3.3% of patients received three or more arthroscopies during the study period.
The negative binomial regression results show a decrease in the incident rate ratios (IRRs) of arthroscopies by financial year, with 2000–01 as the reference (Box 3). The largest decrease was in the 2003–04 year (P < 0.001). The trend appears to increase in subsequent years until 2008–09, although rates are still significantly lower when compared with 2000–01 (P < 0.001).
Other significant factors in the model are also shown in Box 3. The tertile of economic resources was dropped due to collinearity with the tertile of education and occupation (Pearson correlation coefficient = 0.78), which showed a stronger relationship to the outcome in bivariate analysis. Charlson comorbidity was not found to be significant in bivariate analysis so was not included in multivariate analysis. Although we identified a significant reduction in the IRR of arthroscopies around the time of the 2002 Moseley publication (IRR = 0.89; P < 0.01, for 2002–04 compared with 2000–02), the reduction was not sustained in more recent years (IRR = 1.05; P < 0.01, for 2004–09 compared with 2002–04).
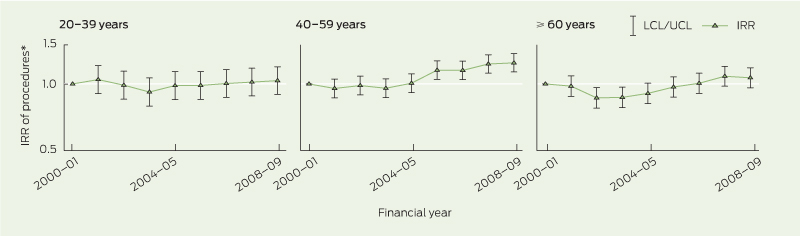
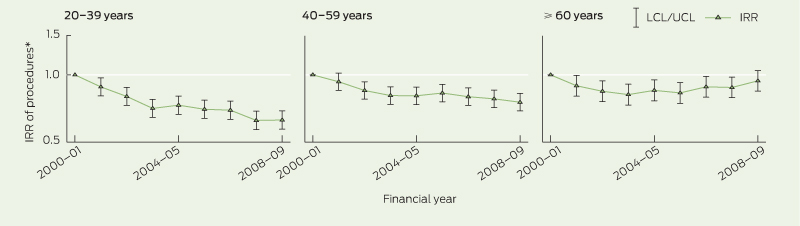
The graphs for the patient subgroup analyses (Box 4, Box 5) show an initial decrease among the youngest and oldest age groups with OA, but this did not persist to 2008–09. Conversely, there was an overall significant increase in arthroscopies for middle-aged patients with a diagnosis of OA (P < 0.001 in 2008–09). There were significant decreasing trends for younger and middle-aged patients without an OA diagnosis, but this was not maintained in the oldest age group in 2008–09 (P = 0.19).
A major strength of our study is that it included all public and private hospital episode data for the whole of Victoria over a 9-year period. We identified an overall decrease in arthroscopy trends from 2000–01, after adjusting for the volume of elective orthopaedic surgery and other confounding factors. However, this trend was not sustained for patients with OA. A potential reason for the observed overall decrease in arthroscopies may be the shift to diagnostic magnetic resonance imaging for younger people who are likely to have had an episode of trauma.21 Our findings show that the largest increase in the IRR of procedures is among same-day admissions within medium orthopaedic volume, private hospitals. These trends suggest a changing model of care for use of elective knee arthroscopy.
The limitations of our study relate to the use of existing data, which are collected for a broad range of reasons, including administrative purposes. However, these methods are in keeping with those used in international studies.11,12 Because we derived the diagnosis of knee OA from coded data taken from patient medical records, there is potential for errors in coding or inaccurate recording in the notes, especially in data from private hospitals where there is not the same rigour of data quality auditing as there is in public hospitals. We conducted sensitivity analysis using data from public hospitals only, and this did not alter the trends.
The downward trend that was noted initially after the Moseley publication was not sustained in patients with OA, suggesting that there was no widespread uptake of the published evidence into practice. There are several explanations for why we did not identify a sustained decrease in arthroscopic procedures among this subgroup. One is that, despite the published evidence, the personal clinical experience of orthopaedic surgeons in the effectiveness of arthroscopic procedures may encourage them to continue using them. The Moseley publication has received criticisms for having methodological flaws9,10 and the Cochrane systematic review in the area included only three studies.8 The article by Kirkley and colleagues6 addressed some of the methodological concerns, but additional evidence may be warranted before changes to practice occur.
Further, the implementation of evidence into practice can be delayed for many years, and health system factors may also contribute to this delay. Patients in Victoria may preferentially seek surgical intervention before trying more conservative therapies, as found in the study examining arthroscopy rates by Kim and colleagues in the US.12 In a national health survey, 6% of Australian patients with OA reported trying to lose weight to manage their condition.22 However, surgical options may be preferred by some patients. This presents a dilemma for surgeons: they do not wish to limit patient choice, but there is uncertain clinical evidence of the benefit of arthroscopy for knee OA.
Total knee arthroplasty is a proven treatment for end-stage knee OA in older patients, but the results are not as good among younger patients.23 Total knee replacement is not always accepted by patients who may prefer minor surgical intervention. Further research in this area, linking previous arthroscopy to subsequent total knee replacement, may be important.
Because arthroscopic procedures can be associated with complications,24,25 it is important that they are used only when they are likely to have measurable positive outcomes. Given the uncertain evidence of effectiveness, general practitioners should encourage patients with OA of the knee who have no evidence of major mechanical derangement to try non-surgical treatments in the first instance.
1 Arthroscopic procedure codes
2 Descriptive characteristics of patients having elective knee arthroscopy
SEIFA = Socio-Economic Indexes for Areas. * Some percentages do not add to 100% due to rounding. |
|||||||||||||||
Received 23 December 2011, accepted 28 June 2012
- Megan A Bohensky1
- Vijaya Sundararajan2
- Nick Andrianopoulos1
- Richard N de Steiger3,4
- Andrew Bucknill5
- Christos M Kondogiannis5
- Geoffrey McColl4
- Caroline A Brand1,5
- 1 Centre of Research Excellence in Patient Safety, Monash University, Melbourne, VIC.
- 2 Monash University, Melbourne, VIC.
- 3 Epworth HealthCare, Melbourne, VIC.
- 4 University of Melbourne, Melbourne, VIC.
- 5 Melbourne Health, Melbourne, VIC.
This study was funded by a grant from Arthritis Australia, who had no other role in it.
- 1. Felson DT, Zhang Y. An update on the epidemiology of knee and hip osteoarthritis with a view to prevention. Arthritis Rheum 1998; 41: 1343-1355.
- 2. Laxafoss E, Jacobsen S, Gosvig KK, Sonne-Holm S. Case definitions of knee osteoarthritis in 4,151 unselected subjects: relevance for epidemiological studies: the Copenhagen Osteoarthritis Study. Skeletal Radiol 2010; 39: 859-866.
- 3. The Royal Australian College of General Practitioners. Guideline for the non-surgical management of hip and knee osteoarthritis. South Melbourne: RACGP, 2009. http://www. racgp.org.au/guidelines/osteoarthritis (accessed Jul 2012).
- 4. Jackson RW. Debate on the use of arthroscopic surgery for osteoarthritis of the knee. Proc (Bayl Univ Med Cent) 2003; 16: 27, discussion 28-29.
- 5. Moseley JB, O’Malley K, Petersen NJ, et al. A controlled trial of arthroscopic surgery for osteoarthritis of the knee. N Engl J Med 2002; 347: 81-88.
- 6. Kirkley A, Birmingham TB, Litchfield RB, et al. A randomized trial of arthroscopic surgery for osteoarthritis of the knee. N Engl J Med 2008; 359: 1097-1107.
- 7. Siparsky P, Ryzewicz M, Peterson B, Bartz R. Arthroscopic treatment of osteoarthritis of the knee: are there any evidence-based indications? Clin Orthop Relat Res 2007; 455: 107-112.
- 8. Laupattarakasem W, Laopaiboon M, Laupattarakasem P, Sumananont C. Arthroscopic debridement for knee osteoarthritis. Cochrane Database Syst Rev 2008; (1): CD005118.
- 9. Chambers K, Schulzer M, Sobolev B. A controlled trial of arthroscopic surgery for osteoarthritis of the knee. Arthroscopy 2002; 18: 683-687.
- 10. Ilahi OA. Selection bias results in misinterpretation of randomized controlled trials on arthroscopic treatment of patients with knee osteoarthritis. Arthroscopy 2010; 26: 144-146.
- 11. Hawker G, Guan J, Judge A, Dieppe P. Knee arthroscopy in England and Ontario: patterns of use, changes over time, and relationship to total knee replacement. J Bone Joint Surg Am 2008; 90: 2337-2345.
- 12. Kim S, Bosque J, Meehan JP, et al. Increase in outpatient knee arthroscopy in the United States: a comparison of National Surveys of Ambulatory Surgery, 1996 and 2006. J Bone Joint Surg Am 2011; 93: 994-1000.
- 13. Australian Bureau of Statistics. Population growth: past, present and future. Canberra: ABS, 2011. (ABS Cat. No. 4102.0.) http://www.abs.gov. au/AUSSTATS/abs@.nsf/Lookup/4102.0Main+ Features10Jun+2010 (accessed Jul 2012).
- 14. Acute Health Division, Victorian Government Department of Human Services. The Victorian Admitted Episodes Dataset: an overview. Melbourne: Victorian DHS, 2001. http://www.health.vic.gov.au/hdss/archive/vaed/vaedover.pdf (accessed Jul 2012).
- 15. Charlson ME, Sax FL, MacKenzie CR, et al. Morbidity during hospitalization: can we predict it? J Chronic Dis 1987; 40: 705-712.
- 16. Quan H, Sundararajan V, Halfon P, et al. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med Care 2005; 43: 1130-1139.
- 17. Zhang JX, Iwashyna TJ, Christakis NA. The performance of different lookback periods and sources of information for Charlson comorbidity adjustment in Medicare claims. Med Care 1999; 37: 1128-1139.
- 18. Australian Bureau of Statistics. Census of population and housing: Socio-Economic Indexes for Areas (SEIFA), Australia – Technical paper, 2001. Canberra: ABS, 2004. (ABS Cat. No. 2039.0.55.001.) http://www.abs.gov.au/AUSSTATS/abs@.nsf/DetailsPage/2039.0.55. 0012001?OpenDocument (accessed Jul 2012).
- 19. Wells VM, Hearn TC, McCaul KA, et al. Changing incidence of primary total hip arthroplasty and total knee arthroplasty for primary osteoarthritis. J Arthroplasty 2002; 17: 267-273.
- 20. Gardner W, Mulvey EP, Shaw EC. Regression analyses of counts and rates: Poisson, overdispersed Poisson, and negative binomial models. Psychol Bull 1995; 118: 392-404.
- 21. Tsai KJ, Chiang H, Jiang CC. Magnetic resonance imaging of anterior cruciate ligament rupture. BMC Musculoskelet Disord 2004; 5: 21.
- 22. Australian Institute of Health and Welfare. A picture of osteoarthritis in Australia. Canberra: AIHW, 2007. (AIHW Cat. No. PHE 93; Arthritis Series No. 5.) http://www.aihw.gov.au/publication-detail/?id=6442468033 (accessed Jul 2012).
- 23. Australian Orthopaedic Association. National Joint Replacement Registry. Annual report. Adelaide: AOA, 2011. http://www.dmac.adelaide. edu.au/aoanjrr/documents/AnnualReports2011/AnnualReport_2011_WebVersion.pdf (accessed Jul 2012).
- 24. Allum R. Complications of arthroscopy of the knee. J Bone Joint Surg Br 2002; 84: 937-945.
- 25. Jameson SS, Dowen D, James P, et al. The burden of arthroscopy of the knee: a contemporary analysis of data from the English NHS. J Bone Joint Surg Br 2011; 93: 1327-1333.
Abstract
Objective: To assess the use of elective knee arthroscopy procedures for all adults 20 years and older, and for adults with a concomitant diagnosis of osteoarthritis (OA) in Victoria.
Design, setting and patients: Retrospective, longitudinal cohort study of 807 030 elective orthopaedic admissions using routinely collected public and private hospital data from 1 July 2000 to 30 June 2009.
Main outcome measure: Trends in rates of elective knee arthroscopy in the time period (defined as a statistically significant change in the incident rate ratio for each financial year with respect to the reference year). Subgroup analyses were undertaken for patients with an associated diagnosis of OA.
Results: There were 190 881 admissions for 159 528 patients having an elective knee arthroscopic procedure. There was a significant decrease in arthroscopic procedures from the 2000–01 financial year, after adjusting for growth in elective orthopaedic volume and relevant patient and hospital characteristics. The trend did not apply to patients with osteoarthritis of the knee. A significant shift in the use of multiday procedures undertaken in high volume, public hospital settings to same-day admissions in the private sector was also identified.
Conclusions: The overall rate of elective knee arthroscopy in Victorian hospitals has decreased. There has been no sustained reduction in arthroscopy use for people with a concomitant diagnosis of OA, despite published evidence questioning the effectiveness of the procedures.