





There is broad recognition of the under‐representation of women in health care and medical leadership.1,2,3,4 The World Health Organization landmark report Delivered by women, led by men5 showed women make up 70% of the global health workforce but only 25% of the leadership. Decades of parity in men and women graduating from medical schools have not translated to gender equality in medical leadership,6 with variable gender participation in medical and surgical specialties and exacerbated by the “leaky” pipeline into medical leadership.2,3,7,8,9,10 Despite improvement, the disparity in Australian medical leadership remains, with only 33% of private hospital Chief Executive Officers and 30% of heads of Australian medical schools being women.11,12,13
Advancing women into health care leadership is an issue of equity and social justice. Furthermore, diversity, including more women into leadership, is likely to improve health system performance and health of the workforce and community.14 Women leaders are more likely to support equitable health policy and delivery, including immunisation, antenatal care, and community health practices, and have improved outcomes, including decreasing neonatal mortality.15,16 Women have been shown generally to display transformational democratic leadership, being team‐focused, motivating and empowering, with benefits of leadership diversity well demonstrated.17,18
The burden of addressing barriers on a woman's path to leadership16 should not sit with individuals but rather with changing the culture, organisations and systems where women work.17 The Advancing Women in Healthcare Leadership (AWHL) initiative focuses on this system‐level change. Funded by the National Health and Medical Research Council (NHMRC) and partner contributions, AWHL integrates health services, policy makers, professional colleges and member organisations with cross‐sector academic expertise. It aims to deliver coproduced, evidence‐based organisational and systems change to have an impact on the workplaces and systems where women work, enabling career goal attainment (Box 1).
Five AWHL research streams have emerged through coproduction with partners: organisational change management; leadership development; exploring intersectionality across race, ethnicity and gender diversity; nursing leadership; and collective action by member organisations. Here, we focus on this last stream, recognising the important role member organisations (including professional associations and colleges), play in medical careers. We aim to (i) explore the current and potential roles of partner professional colleges and member organisations, reaching within, across and beyond these entities to the broader health care sector; (ii) map organisational activity against evidenced‐based interventions; and (iii) identify opportunities and priorities for interventions moving forward. We apply the Consolidated Framework for Implementation Research (CFIR)19,20 for insights into (i) broad societal norms, expectations and culture where implementation occurs (outer setting); (ii) internal organisational culture and prioritisation of gender equity (inner setting); (iii) evidence base and quality of interventions already underway to address gender equity (intervention characteristics); (iv) the appetite and readiness of people within organisations to engage in implementation (individuals involved); and (v) the process of implementation19,20 (Supporting Information, figure 1).
Coproduction
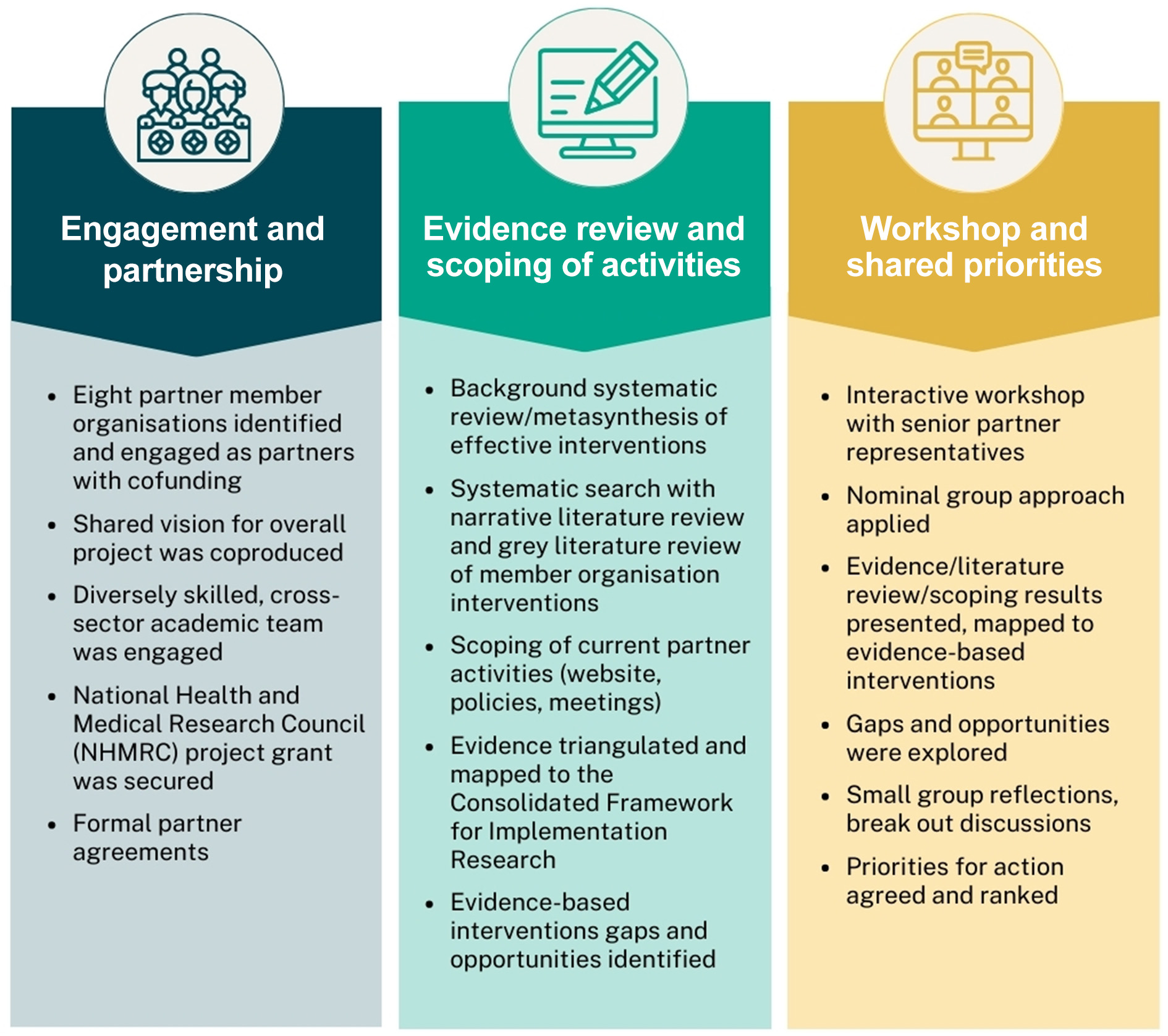
The phases of formative research for this national initiative are outlined in Box 2. The cross‐sector academic team engaged multiple stakeholders, including medical member organisations and colleges, with partnership involving cash and in‐kind contributions, matched in a nationally competitive grant by the NHMRC. Coproduction approaches were applied to explore, map, identify and prioritise the roles of partners within their organisations and across the broader health care sector. These relied on close collaboration with partner organisations, building trust and mutual respect across all stages, in their role as both knowledge generators and end users.
We performed a systematic search with a narrative literature review including grey literature and organisational website search (Supporting Information, table 1). We interrogated publicly available information and field notes from meetings with partners to gain insight into the roles and activities of member organisations in gender equity. We captured strategic plans, policies, reports, regulations, training accreditation standards and guidelines of member organisations. These included, but were not limited to, flexible and interrupted training, parental leave, diversity, inclusion and gender equity. We then mapped these against five categories of evidence‐based organisational strategies shown to advance women in leadership21 (Supporting Information, table 2). We applied the CFIR to examine the “outer” broader social, political and “inner” organisational contexts in which the work of promoting gender equity was occurring.
Individual partner meetings were held to ensure relevant data from their organisations were captured. An interactive online workshop was held, which included 20 senior representatives from partner organisations and academics, including senior management staff and gender equity or diversity and inclusion leads. The workshop applied nominal group approaches as a structured method to gain contributions and consensus from the range of partner representatives present. This methodology included structured presentations, individual and small‐group discussions capturing reflections and ideas, and then discussions to capture consensus and priorities. Objectives included:
- exploring roles and responsibilities;
- interactively reviewing and reflecting on the de‐identified evidence of gender equity activities;
- identifying gaps and opportunities for implementation of organisational interventions; and
- exploring opportunities for collective action.
Ethics approval was provided by the Monash University Human Research Ethics Committee (Project ID 25097).
Activities of member organisations
Eight colleges and membership organisations partnered initially in AWHL: the Royal Australasian College of Medical Administrators, the Royal Australasian College of Physicians, the Royal Australasian College of Surgeons, the Royal Australian and New Zealand College of Obstetricians and Gynaecologists, the Australian College of Nursing, the Australasian College of Dermatologists, the Royal Australian College of General Practitioners and the Australian Medical Association.
The literature review and engagement with partners identified multiple roles of these organisations in medical careers, despite not being significant employers of the medical workforce (Box 3). Partners’ roles included career development, overseeing postgraduate medical training and continuing professional development. These organisations provide leadership opportunities and skills through participation in internal organisational education, policy, and governance committees and promote academic engagement and networking. They assign membership based on criteria and remove membership privileges if professional standards and codes of conduct are breached. Externally, these organisations are a respected voice for the health care industry, are key public and political advocacy stakeholders, and negotiate industrial agreements for medical staff.
Mapping of current activity against evidence‐based interventions21 (Box 4) showed that most partner organisations had gender equity or diversity and inclusion working groups, and all recognised the importance of preventing harassment and discrimination. Two had leadership and board approval for gender equity plans and gender targets for representation on leadership committees, examinations and conference panels. Two had established targets for gender representation in training programs, yet only one had formally reported on progress on these. Two had committed to collecting data on participation of women within subspecialties and investigating barriers to subspecialty entry. Only one had reported on progress and had committed to regular review and reporting. No evidence of collective action was identified.
Most partner organisations had policies for bullying, harassment and discrimination, flexible training, interrupted training, and principles for parental leave. Many policies were contingent on flexible training positions availability at health service level, which is left to arguably disempowered early career doctors to negotiate in the absence of workplace system‐level solutions. One college reported flexible training positions online. There was no available evidence of implementation or enforcement of relevant policies, standards or regulations.
Accreditation of training standards for health services included availability of flexible training and a culture of respect. These were not linked to gender equity and no public record of implementation was found. Although all organisations provided networking opportunities such as annual academic meetings, only one had public evidence of a mentoring program for women. One organisation had established leadership training for its leaders and another focused on training medical leaders across all disciplines.
Coproduction workshop, priorities and community of practice
Relevant literature, and mapping of organisational activities compared with the evidence and to an implementation framework, showed that most partners had positive intent, yet they did not fully grasp potential opportunities and roles, and were early in their implementation journeys.
During the workshop, it was acknowledged that publicly available information did not reflect the activities within many organisations, only reflected a single time point on an evolving issue, and collaboration was extended to collect further data. Workshop participants shared their motivations, updates on their organisation's progress, achievements to date and challenges they were facing.
Member organisations unanimously agreed that collective action was a priority to increase the reach and impact of organisational interventions to advance women in leadership. They explored the opportunities, identified and prioritised strategies to deliver organisational and systems‐level change. Partners were highly invested and engaged, and this was reflected in a commitment to improving organisational policies and practices, and to collectively developing gender equity‐focused training accreditation standards. They recognised the importance of reducing gender bias within training programs by implementing flexible training options and parental leave, as well as their vital role in providing broader advocacy within, across and beyond their own organisations to the broader health care sector.
The partner organisations enthusiastically agreed to establish and participate in a Community of Practice as a priority, to share experiences and learnings and more effectively influence the settings where women work. Further priorities of the Community of Practice include: developing aligned principles for flexible training and parental leave policies, considering the development of a shared accreditation standard focused on gender equitable practices, and engaging in broader advocacy (Supporting Information, table 3).
Implementation context
Using the CFIR to frame implementation efforts, the “outer setting” context in Australia includes the establishment of the national Workplace Gender Equality Agency (WGEA)22 and, in Victoria, the Gender Equality Act 2020,23 both requiring mandatory collection and reporting of gender equity indicators. This has enhanced interest and commitment of member organisations and health services to advance women in health care leadership. Despite not being direct employers of the medical workforce, they recognise their ability to advance gender equality. Understanding and actioning their potential roles to drive policy‐mandated change is key to progress.
Evidence‐based interventions to advance women in health care leadership are now established,21 and here the literature and publicly available data24,25,26,27 on member organisation activities were mapped against the evidence, showing gaps and opportunities. We contextualised these findings in terms of understanding the internal organisational commitment to implementing evidence‐based change, aligned to the CFIR. Partner member organisations’ “inner” context shows general awareness of the importance of gender equity, and increasing organisational engagement and commitment, reflected by strong engagement in the AWHL initiative. However, organisations varied considerably in maturity, readiness, and actions to implement change, with most early in the journey. Only three organisations had published a strategy to manage issues of women in leadership, including implementation of gender targets, with only two reporting on progress. Nevertheless, they all enthusiastically agreed to continue shared communication and collaboration through a Community of Practice, and the coproduction of collective evidence‐based interventions that can be applied in their own contexts.
Next steps
Interest in this national initiative has resulted in substantial expansion to include multiple additional medical colleges, and a second successful NHMRC partnership grant has now been obtained to fund and deliver this work.
Extensive engagement and in‐depth qualitative research and surveys are now underway to further understand the “inner” partner context, such as attitudes, knowledge, policies, and behaviours of the leadership, members, trainees and early career professionals. Data will be triangulated with available public information, such as that reported here, to inform further implementation research and activities.
Ongoing coproduction with the partner organisations continues, using the newly established Community of Practice as the platform to bring to life these next phases of collective knowledge generation, intervention development, implementation and evaluation. These efforts aim beyond the problem and barriers to evidence‐based solutions to advance women into health care leadership for equity.
Box 1 – Advancing Women in Healthcare Leadership (AWHL) initiative structure
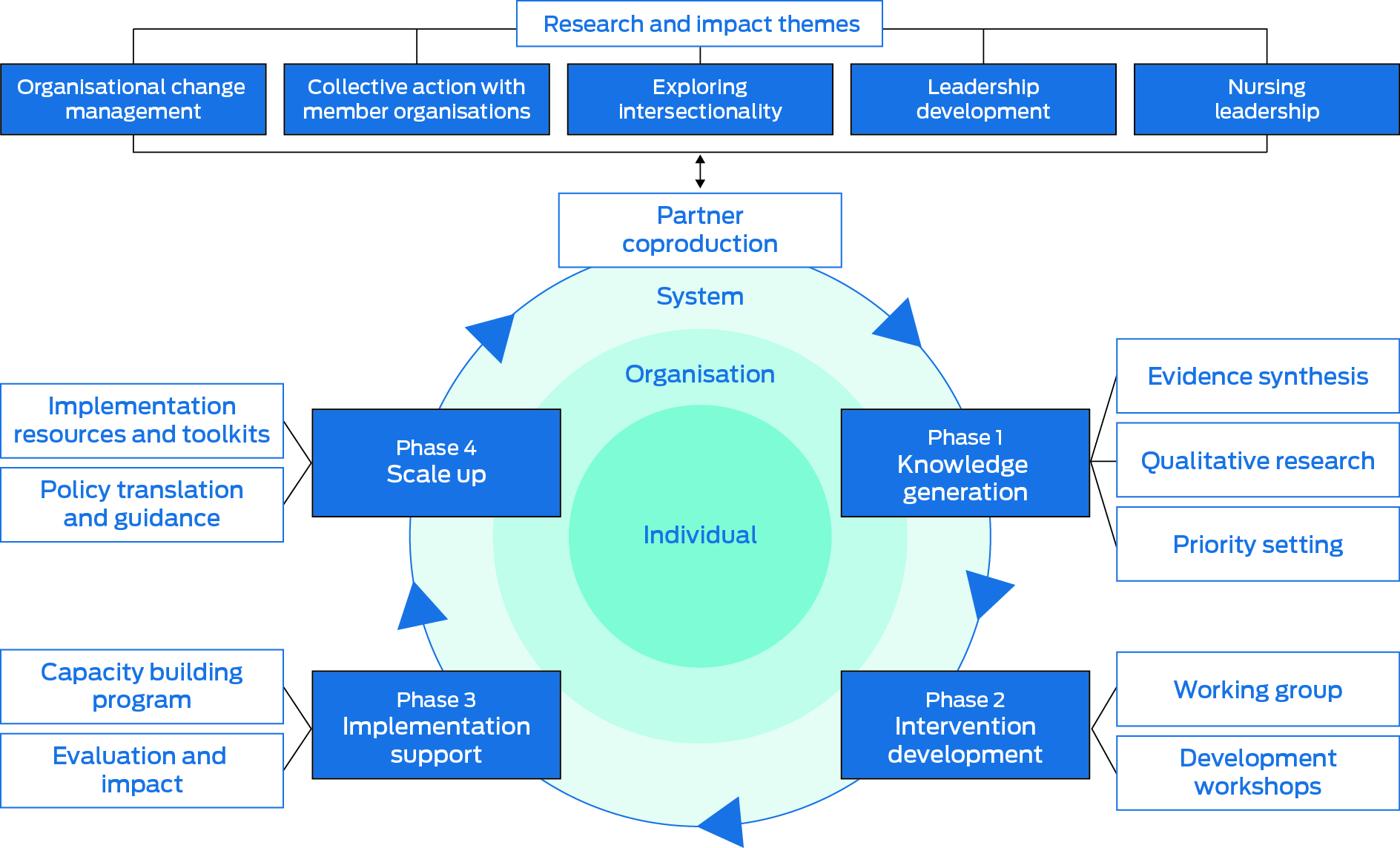
This figure was originally created by the AWHL team, chaired by Helena Teede, and is copyrighted to Monash University (2022). There are no patents or royalties, but we reserve the right to use the diagram again in other publications.
Box 3 – Roles and responsibilities of professional medical membership organisations
|
Roles and responsibilities |
Organisations |
||||||||||||||
|
|
|||||||||||||||
|
Training |
|
|
|||||||||||||
|
Accreditation of training |
|
|
|||||||||||||
|
Training programs |
|
|
|||||||||||||
|
Continuing professional development |
|
|
|||||||||||||
|
Leadership |
|
|
|||||||||||||
|
Governance |
|
|
|||||||||||||
|
Networking and mentoring |
|
|
|||||||||||||
|
Research |
|
|
|||||||||||||
|
Policy and advocacy |
|
|
|||||||||||||
|
Industrial |
|
|
|||||||||||||
|
|
|||||||||||||||
|
AMA = Australian Medical Association. |
|||||||||||||||
Box 4 – Publicly available activities promoting the advancement of women in member organisations
|
Category |
Level of implementation |
||||||||||||||
|
|
|||||||||||||||
|
Organisational processes |
|
||||||||||||||
|
Policies |
|
||||||||||||||
|
Flexible training |
All |
||||||||||||||
|
Parental leave |
None (but mentioned in flexible training policy) |
||||||||||||||
|
Interruption to training |
All |
||||||||||||||
|
Accreditation of training positions |
|
||||||||||||||
|
All posts operate within a culture of respect |
All subject to service availability of flexible training positions |
||||||||||||||
|
Flexible training positions allowed |
|||||||||||||||
|
Family friendly events, conferences |
Three |
||||||||||||||
|
Gender representation at conferences |
Three set targets |
||||||||||||||
|
Awareness and engagement |
|
||||||||||||||
|
Collection of data on gender participation in subspecialties |
One reports publicly |
||||||||||||||
|
Investigate barriers to entry to training programs |
Two reported on barriers to entry |
||||||||||||||
|
Standards for education leadership (free from discrimination, bullying and harassment) |
All |
||||||||||||||
|
Mentoring and networking |
|
||||||||||||||
|
Early to mid‐career mentoring for women specialists |
One |
||||||||||||||
|
Leader training and development |
|
||||||||||||||
|
Formal leadership training programs |
One |
||||||||||||||
|
Organisational support tools |
|
||||||||||||||
|
Transparent data on gender composition of committees |
One |
||||||||||||||
|
Selection in training programs |
Two had specific criteria |
||||||||||||||
|
Training standards |
|
||||||||||||||
|
Flexible training |
All |
||||||||||||||
|
Safe workloads that do not lead to burnout |
All |
||||||||||||||
|
Trainee work–life balance |
All |
||||||||||||||
|
Leadership commitment and accountability |
|
||||||||||||||
|
Gender equity or diversity and inclusion working groups or committees |
Five |
||||||||||||||
|
Gender quality/diversity and inclusion plans |
Four |
||||||||||||||
|
Gender targets |
|
||||||||||||||
|
Representation on board, councils, committees |
Three |
||||||||||||||
|
Representation in training programs |
Two |
||||||||||||||
|
Representation at events and conferences |
Three |
||||||||||||||
|
Formal reporting on targets |
Two |
||||||||||||||
|
|
|||||||||||||||
|
|
|||||||||||||||
Provenance: Not commissioned; externally peer reviewed.
- 1. Bickel J, Wara D, Atkinson B, et al. Increasing women's leadership in academic medicine: report of the AAMC Project Implementation Committee. Acad Med 2002; 77: 1043‐1061.
- 2. Brown MA, Erdman MK, Munger AM, Miller AN. Despite growing number of women surgeons, authorship gender disparity in orthopaedic literature persists over 30 years. Clin Orthop Relat Res 2020; 478: 1542‐1552.
- 3. Burgess S, Shaw E, Ellenberger KA, et al. Gender equity within medical specialties of Australia and New Zealand: cardiology's outlier status. Intern Med J 2020; 50: 412.
- 4. Jagsi R, Means O, Lautenberger D, et al. Women's representation among members and leaders of national medical specialty societies. Acad Med 2020; 95: 1043‐1049.
- 5. World Health Organization. Delivered by women, led by men: a gender and equity analysis of the global health and social workforce. Geneva: WHO, 2019. https://www.who.int/publications/i/item/9789241515467 (viewed Sept 2022).
- 6. Medical Deans Australia and New Zealand. Medical Schools Outcomes Database reports. Sydney: Medical Deans, 2022. https://medicaldeans.org.au/data/medical‐schools‐outcomes‐database‐reports/ (viewed Oct 2022).
- 7. Danko D, Cheng A, Losken A. Gender diversity in plastic surgery: Is the pipeline leaky or plugged? Plast Reconstr Surg 2021; 147: 1480‐1485.
- 8. Carnes M, Bairey Merz C. Women are less likely than men to be full professors in cardiology: why does this happen and how can we fix it? Circulation 2017; 135: 518‐520.
- 9. Liang R, Dornan T, Nestel D. Why do women leave surgical training? A qualitative and feminist study. Lancet 2019; 393: 541‐549.
- 10. Angstmann M, Woods C, de Costa CM. Gender equity in obstetrics and gynaecology — where are we heading? Aust N Z J Obstet Gynaecol 2019; 59: 177‐180.
- 11. Cohn A, Cubitt M, Goh A, et al. Gender equity in Australian health leadership. Asia Pacific Journal of Health Management 2021; 16: i519.
- 12. Workplace Gender Equality Agency. WGEA Data Explorer 2021. https://data.wgea.gov.au/ (viewed Aug 2022).
- 13. Australian Medical Council. Heads of Australian Medical Council accredited medical school websites [website]. 2022. https://www.amc.org.au/accredited‐organisations/medical‐schools/accredited‐medical‐schools/ (viewed Sept 2022).
- 14. Heymann J, Levy JK, Bose B, et al. Improving health with programmatic, legal, and policy approaches to reduce gender inequality and change restrictive gender norms. Lancet 2019; 393: 2522‐2534.
- 15. Downs JA, Reif LK, Hokororo A, Fitzgerald DW. Increasing women in leadership in global health. Acad Med 2014; 89: 1103‐1107.
- 16. King TL, Kavanagh A, Scovelle AJ, Milner A. Associations between gender equality and health: a systematic review. Health Promot Int 2018; 35: 27‐41.
- 17. Fontenot T. Leading ladies: women in healthcare leadership. Front Health Serv Manage 2012; 28: 11‐21.
- 18. Eagly AH, Johannesen‐Schmidt MC. The leadership styles of women and men. J Soc Issues 2001; 57: 781‐797.
- 19. Damschroder LJ, Aron DC, Keith RE, et al. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sci 2009; 4: 50.
- 20. Damschroder LJ, Reardon CM, Widerquist MAO, Lowery J. The updated Consolidated Framework for Implementation Research based on user feedback. Implement Sci 2022; 17: 75.
- 21. Mousa M, Boyle J, Skouteris H, et al. Advancing women in healthcare leadership: a systematic review and meta‐synthesis of multi‐sector evidence on organisational interventions. EClinicalMedicine 2021; 39: 101084.
- 22. Workplace Gender Equality Agency. What we do [website]. https://www.wgea.gov.au/what‐we‐do (viewed Sept 2022).
- 23. Commission for Gender Equality in the Public Sector. About the Gender Equality Act 2020. Melbourne: Victoria State Government, 2020. https://www.genderequalitycommission.vic.gov.au/about‐gender‐equality‐act‐2020 (viewed Sept 2022).
- 24. Australian Medical Association. AMA Gender Equity Summit report 2019. Canberra: AMA, 2019. https://www.ama.com.au/articles/ama‐gender‐equity‐summit‐report‐2019 (viewed Apr 2023).
- 25. Royal Australasian College of Surgeons. Diversity and Inclusion Plan: 2019 progress update. Melbourne: RACS, 2019. https://www.surgeons.org/‐/media/Project/RACS/surgeons‐org/files/operating‐with‐respectcomplaints/building‐respect/diversity‐and‐inclusion‐plan‐2019.pdf (viewed Sept 2022).
- 26. Royal Australian and New Zealand College of Obstetricians and Gynaecologists. Gender Equity and Diversity Policy. Melbourne: RANZCOG, 2021. https://ranzcog.edu.au/wp‐content/uploads/2022/04/Gender‐Equity‐and‐Diversity‐Policy.pdf (viewed Sept 2022).
- 27. Royal Australasian College of Physicians. Flexible training options [website]. Sydney: RACP, 2021. https://www.racp.edu.au/trainees/flexible‐training‐options (viewed Apr 2023).
Open access:
Open access publishing facilitated by Monash University, as part of the Wiley – Monash University agreement via the Council of Australian University Librarians.
Jenny Proimos is supported by an Australian Government Research Training Program (RTP) stipend. We acknowledge the contribution of the partner organisations: the Australian Medical Association, the Australian College of Nursing, the Australasian College of Dermatologists, the Royal Australian College of General Practitioners; the Royal Australasian College of Medical Administrators, the Royal Australasian College of Physicians, the Royal Australasian College of Surgeons, and the Royal Australian and New Zealand College of Obstetricians and Gynaecologists. We also acknowledge Mariam Mousa, author of the systematic review of evidence‐informed organisational interventions to advance women in leadership, on which the mapping exercise in this article is based.
No relevant disclosures.