





Research letter
Open access CC BY NC
Volume 220 - Issue 2
Steatotic liver disease in rural and regional Victoria, according to the NAFLD and newer diagnostic criteria: retrospective cohort analyses of 2001–03 and 2016–18 data
Authors: Karl Vaz, William W Kemp, Ammar Majeed, John Lubel, Dianna Magliano, Kristen Glenister, Lisa Bourke, David Simmons and Stuart K Roberts
Med J Aust 2024; 220 (2): 97-99. || doi: 10.5694/mja2.52189
Published online: 5 February 2024
Published online: 5 February 2024
The rising prevalence of steatotic liver disease parallels that of obesity in regional and rural Victoria
The global prevalence of non‐alcoholic fatty liver disease (NAFLD) among adults is 25–30%,1 and it is fast becoming the most frequent indication for liver transplantation.2 Its increasing prevalence is linked with the rise in that of obesity.3
The suggestion by an international expert panel that NAFLD be re‐termed “metabolic dysfunction‐associated fatty liver disease” (MAFLD)4 has been widely endorsed, including by the foremost Asia–Pacific hepatology society (Asian Pacific Association for the Study of the Liver).5 A multi‐society Delphi process (predominantly involving European and North and South American experts) reached consensus on changing the name to “metabolic dysfunction‐associated steatotic liver disease” (MASLD).6 The change was motivated by the recognition that “NAFLD” has trivialising, pejorative, and stigmatising connotations, and does not highlight the disease pathophysiology, including dysmetabolism.
As the prevalence of disease according to the criteria for the three diagnoses has not been compared, we evaluated their prevalence in regional Victoria. We analysed data collected during two longitudinal, cross‐sectional studies of health, disease, and access to health care in the Goulburn Valley in rural Victoria: CrossRoads I (CR‐I; June 2001 – February 2003) and CrossRoads II (CR‐II; October 2016 – August 2018)7 (further details: Supporting Information, section 1). The CrossRoads studies were approved by the Goulburn Valley Health Human Research Ethics Committee (GCH‐3/99, GVH‐20/16) and the Alfred Health Ethics Committee (project 310/22).
Steatotic liver disease was defined by a fatty liver index value of 60 or more,8 NAFLD as steatotic liver disease in people for whom excessive alcohol consumption (men: ≥30g/day; women: ≥20 g/day) and viral hepatitis (CR‐I: self‐report; CR‐II: serological evidence) were not recorded.9 MAFLD and MASLD were diagnosed according to the published criteria.4,6 Each diagnosis requires evidence of both steatotic liver disease and metabolic derangement, with minor differences in the threshold applied. MAFLD permits any degree of concurrent alcohol consumption or liver disease; MASLD is more restrictive, excluding people who report excessive alcohol consumption (Box 1).
Categorical data are summarised as frequencies and proportions; differences were assessed in χ2 or Fisher exact tests. Continuous data are summarised as means with standard deviations (SDs); the statistical significance of differences was assessed in Student t tests. Age‐ and gender‐standardised prevalence was calculated using direct standardisation and Australian 2022 population data.10 P<0.05 (two‐tailed) was deemed statistically significant. All statistical analyses were conducted in SPSS 28.0 (IBM); graphs were produced in Prism GraphPad 9.4.1.
Evaluable data (including weight and waist circumference for calculating the fatty liver index) were available for 1040 of 1048 CR‐I participants (99.2%) and 721 of 747 CR‐II participants (96.5%). Compared with CR‐I participants, the mean age of CR‐II participants was higher (59.9 [SD, 16.1] v 52.8 [SD, 15.6] years); larger proportions lived in rural areas (53.4% v 33.5%), were overweight or obese (73.0% v 68.4%), had an elevated waist circumference (80.0% v 72.0%), or consumed take‐away food at least once a week (213 of 695 [30.6%] v 271 of 1037 [26.1%]), while a smaller proportion currently smoked (67 of 695 [9.6%] v 179 of 1037 [17.3%]) (Supporting Information, table 1).
The crude prevalence of NAFLD was higher among CR‐II than CR‐I participants (38.6% v 32.7%), as was that of MAFLD (46.9% v 40.3%) and MASLD (39.1% v 34.6%). After standardisation for age and gender, no differences in prevalence between CR‐I and CR‐II participants were statistically significant (Box 2).
In total, 758 participants across the two studies satisfied the criteria for at least one of the three diagnoses. All CrossRoads participants who satisfied the NAFLD diagnostic criteria also met those for MASLD; all but one also met the diagnostic criteria for MAFLD (one person had steatotic liver disease without metabolic derangement of the degree required for MAFLD). However, 138 participants who satisfied the MAFLD criteria (CR‐I, 80; CR‐II, 58 participants) and 23 who satisfied the MASLD criteria (CR‐I, twenty; CR‐II, three participants) did not meet the NAFLD criteria because of alcohol‐related liver disease or viral hepatitis. Finally, 123 participants who satisfied the MAFLD criteria (CR‐I, 60; CR‐II, 63 participants) did not meet the MASLD criteria (excessive alcohol consumption, 116; alcohol use unknown, seven). Overall, 611 of 758 people with steatotic liver disease satisfied the criteria for all three diagnoses (80.6%; Supporting Information, figure 1).
In each CrossRoads study, the age‐ and gender‐standardised prevalence of each diagnosis was generally slightly higher in rural than regional areas (exception: MAFLD in CR‐II); the inter‐study differences in standardised prevalence were small for both regional and rural areas (Supporting Information, table 2).
The proportions of participants with steatotic liver disease with indeterminate or high fibrosis‐4 index values were larger in CR‐II than in CR‐I: NAFLD: 106 of 242 (43.8%) v 108 of 340 (31.8%; P = 0.003); MAFLD: 135 of 301 (44.9%) v 144 of 419 (34.4%; P = 0.005); MASLD: 109 of 245 (44.5%) v 121 of 360 (33.6%; P = 0.009). Across the two trials, the proportions of participants with indeterminate or high NAFLD fibrosis scores were similar for those who satisfied the criteria for NAFLD (333 of 575, 57.9%), MAFLD (413 of 704, 58.7%), or MASLD (349 of 597, 58.5%) (Box 3).
Limitations of our study include the uncertain generalisability across Australia of our study undertaken in regional and remote Victoria, the lack of ultrasound facilities for assessing steatotic liver disease, and missing data for certain covariates (eg, recording of physical activity).
We found that 43% (MAFLD) or 35% (MASLD) of regional and rural Victorian participants in the 2016–18 CR‐II study satisfied the diagnostic criteria for the newer steatotic liver disease diagnoses. Further, the concordance of these diagnoses with NAFLD across the two CrossRoads studies was good. The possibility of other liver disease allowed by the MAFLD criteria was not associated with greater fibrosis risk; the proportions of indeterminate or high fibrosis scores were similar for all three diagnoses. Information about long term clinical outcomes is still needed, but the proportion of participants with steatotic liver disease at indeterminate or high risk of fibrosis and who therefore required second line tests (eg, transient elastography) and referral to tertiary care was larger in the second than in the first CrossRoads study. The rising prevalence of steatotic liver disease, parallel to that of obesity, could place a significant burden on health care in regional and rural Victoria.
Box 1 – Diagnostic criteria for steatotic liver disease in adults
|
Diagnosis |
Required criteria |
Other criteria |
|||||||||||||
|
|
|||||||||||||||
|
Non‐alcoholic fatty liver disease (NAFLD)9 |
≥5% hepatic steatosis |
|
|||||||||||||
|
Metabolic dysfunction‐associated fatty liver disease (MAFLD)5 |
≥5% hepatic steatosis |
|
|||||||||||||
|
Metabolic dysfunction‐associated steatotic liver disease (MASLD)6 |
≥5% hepatic steatosis |
|
|||||||||||||
|
|
|||||||||||||||
|
BMI = body mass index; HbA1c = glycated haemoglobin; HDL = high‐density lipoprotein. * Parameters for which data were not available in the two CrossRoads datasets, and were therefore not used for defining MAFLD definition in our study. |
|||||||||||||||
Box 2 – Crude and age‐ and gender‐standardised prevalence (with 95% confidence intervals) of steatotic liver disease among participants in the two CrossRoads studies, by diagnosis
|
Characteristic |
Non‐alcoholic fatty liver disease (NAFLD) |
Metabolic dysfunction‐associated fatty liver disease (MAFLD) |
Metabolic dysfunction‐associated steatotic liver disease (MASLD) |
||||||||||||
|
|
|||||||||||||||
|
Participants meeting diagnosis |
|
|
|
||||||||||||
|
CrossRoads I |
340/1040 |
419/1040 |
360/1040 |
||||||||||||
|
CrossRoads II |
272/704 |
338/721 |
275/704 |
||||||||||||
|
Crude prevalence |
|
|
|
||||||||||||
|
CrossRoads I |
32.7% (29.8–35.6%) |
40.3% (37.3–43.3%) |
34.6% (31.7–37.6%) |
||||||||||||
|
CrossRoads II |
38.6% (35.0–42.3%) |
46.9% (43.2–50.6%) |
39.1% (35.4–42.8%) |
||||||||||||
|
Difference |
5.9 percentage points (5.7–6.1 percentage points) |
6.6 percentage points (4.4–8.8 percentage points) |
4.5 percentage points (2.3–6.9 percentage points) |
||||||||||||
|
Standardised prevalence |
|
|
|
||||||||||||
|
CrossRoads I |
32.0% (28.9–35.2%) |
38.5% (35.2–41.7%) |
33.6% (30.4–36.7%) |
||||||||||||
|
CrossRoads II |
34.7% (30.2–39.1%) |
42.6% (38.1–47.2%) |
35.0% (30.5–39.5%) |
||||||||||||
|
Difference |
2.7 percentage points (–2.9% to 8.2 percentage points) |
4.1 percentage points (–1.4 to 9.8 percentage points) |
1.4 percentage points (–4.1% to 6.9 percentage points) |
||||||||||||
|
|
|||||||||||||||
|
|
|||||||||||||||
Box 3 – Distribution of fibrosis‐4 index and NAFLD fibrosis scores (NFS) for participants in the two CrossRoads studies who satisfied the diagnostic criteria for steatotic liver disease, by diagnosis*
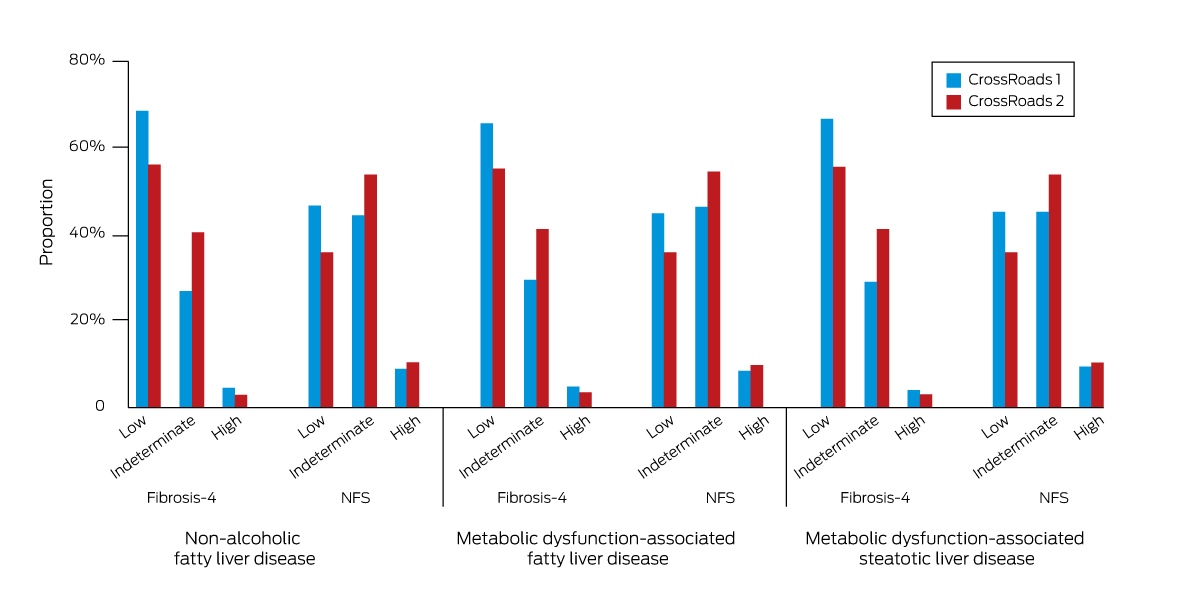
NAFLD = non‐alcoholic fatty liver disease.* Fibrosis‐4 index: low risk, <1.30; indeterminate risk, 1.30–2.67; high risk, >2.67. NAFLD fibrosis score: low risk, <–1.455; indeterminate risk, –1.455 to 0.676; high risk, >0.676.
Competing interests
No relevant disclosures.
Acknowledgements
This study was supported by a National Health and Medical Research Council partnership grant (APP 1113850).
References
- Le MH, Yeo YH, Li X, et al. 2019 Global NAFLD prevalence: a systematic review and meta‐analysis. Clin Gastroenterol Hepatol 2022; 20: 2809‐2817.
- Wong RJ, Singal, AK. Trends in liver disease etiology among adults awaiting liver transplantation in the United States, 2014–2019. JAMA Netw Open 2020; 3: e1920294.
- Ng M, Fleming T, Robinson M, et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014; 384: 766‐781.
- Eslam M, Newsome PN, Sarin SK, et al. A new definition for metabolic dysfunction‐associated fatty liver disease: an international expert consensus statement. J Hepatol 2020; 73: 202‐209.
- Eslam M, Sarin SK, Wong VWS, et al. The Asian Pacific Association for the Study of the Liver clinical practice guidelines for the diagnosis and management of metabolic associated fatty liver disease. Hepatol Int 2020; 14: 888‐919.
- Rinella ME, Lazarus JV, Ratziu V, et al; NAFLD Nomenclature consensus group. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. J Hepatol 2023; 79: 1554‐1556.
- Glenister KM, Bourke L, Bolitho L, et al. Longitudinal study of health, disease and access to care in rural Victoria: the Crossroads‐II study: methods. BMC Public Health 2018; 18: 670.
- Bedogni G, Bellentani S, Miglioli L, et al. The Fatty Liver Index: a simple and accurate predictor of hepatic steatosis in the general population. BMC Gastroenterol 2006; 6: 33.
- European Association for the Study of the Liver (EASL); European Association for the Study of Diabetes (EASD); European Association for the Study of Obesity (EASO). EASL‐EASD‐EASO clinical practice guidelines for the management of non‐alcoholic fatty liver disease. J Hepatol 2016; 64: 1388‐1402.
- Australian Bureau of Statistics. National, state and territory population. Reference period: December 2022. 15 June 2023. https://www.abs.gov.au/statistics/people/population/national‐state‐and‐territory‐population/dec‐2022 (viewed July 2023).