





Position statement summary
Open access CC BY NC ND
Volume 220 - Issue 1
Cough in Children and Adults: Diagnosis, Assessment and Management (CICADA). Summary of an updated position statement on chronic cough in Australia
Authors: Julie M Marchant, Anne B Chang, Emma Kennedy, David King, Jennifer L Perret, Andre Schultz, Maree R Toombs, Lesley Versteegh, Shyamali C Dharmage, Rebecca Dingle, Naomi Fitzerlakey, Johnson George, Anne Holland, Debbie Rigby, Jennifer Mann, Stuart Mazzone, Mearon O'Brien, Kerry‐Ann O'Grady, Helen L Petsky, Jonathan Pham, Sheree MS Smith, Danielle F Wurzel, Anne E Vertigan and Peter Wark
Med J Aust 2024 || doi: 10.5694/mja2.52157
Published online: 20 November 2023
Published online: 20 November 2023
Correction(s) for this article:
Erratum | Published online: 26 June 2024
Updated recommendations from the Thoracic Society of Australia and New Zealand and Lung Foundation Australia for managing chronic cough in children and adults
Abstract
Introduction: Cough is the most common symptom leading to medical consultation. Chronic cough results in significant health care costs, impairs quality of life, and may indicate the presence of a serious underlying condition. Here, we present a summary of an updated position statement on cough management in the clinical consultation.
Main recommendations: Assessment of children and adults requires a focused history of chronic cough to identify any red flag cough pointers that may indicate an underlying disease. Further assessment with examination should include a chest x‐ray and spirometry (when age>6years). Separate paediatric and adult diagnostic management algorithms should be followed. Management of the underlying condition(s) should follow specific disease guidelines, as well as address adverse environmental exposures and patient/carer concerns. First Nations adults and children should be considered a high risk group. The full statement from the Thoracic Society of Australia and New Zealand and Lung Foundation Australia for managing chronic cough is available at https://lungfoundation.com.au/resources/cicada‐full‐position‐statement.
Changes in management as a result of this statement:
- Algorithms for assessment and diagnosis of adult and paediatric chronic cough are recommended.
- High quality evidence supports the use of child‐specific chronic cough management algorithms to improve clinical outcomes, but none exist in adults.
- Red flags that indicate serious underlying conditions requiring investigation or referral should be identified.
- Early and effective treatment of chronic wet/productive cough in children is critical.
- Culturally specific strategies for facilitating the management of chronic cough in First Nations populations should be adopted.
- If the chronic cough does not resolve or is unexplained, the patient should be referred to a respiratory specialist or cough clinic.
Cough is a common condition leading to clinical consultation and results in significant health care costs. Guidelines seek to standardise and assist in diagnosis, investigation and management of cough.1,2 Cough in Children and Adults: Diagnosis, Assessment and Management (CICADA) is an updated Australian position statement on the clinical assessment and management of chronic cough that highlights the burden of chronic cough, including the disproportionate burden in our First Nations population. We provide recommendations for initial assessment of chronic cough in clinical practice, including red flags in history and examination, and CICADA diagnostic management algorithms for use in paediatrics (Box 1) and adults (Box 2). As there is high quality evidence that the common aetiologies of chronic cough in children and adults are not the same, we discuss the management of paediatric and adult chronic cough separately.3
Method
CICADA was developed by a multidisciplinary expert committee that convened to undertake a systematic literature review and discuss updated recommendations. A total of 6395 articles were screened and 277 new studies since 2010 (the previous CICADA update)4 were included in the updated full statement (Box 3 provides details of the guideline development process). Throughout the position statement (in the main text and in the box summarising the recommendations and their level of evidence and strength), the GRADE of evidence6 refers to evidence of the efficacy of treatment recommendations for cough in association with the respective conditions. The full statement can be found at https://lungfoundation.com.au/resources/cicada‐full‐position‐statement. We plan to update the statement every 2 years.
Burden of chronic cough
In 2015, the prevalence of chronic cough in adults was estimated to be 9.6% (95% CI, 7.6–11.7%) globally,7 and 8.8% in Australia.8 The prevalence of chronic cough gradually increases to peak in the sixth decade9 and has been estimated to occur in 3% of never smokers, 4% of former smokers and 8% of current smokers.10 Overall, chronic cough presents more commonly in middle‐aged women.2
There are limited Australian studies on population prevalence of chronic cough in children.11 In a recent study of Australian children presenting to emergency departments, 7.5% had chronic cough, and 20–23% had persistent cough at day 28 irrespective of duration of cough on presentation.12 The prevalence of chronic wet cough in children living in Indigenous communities is higher (around 13%).13
First Nations Australians are disproportionately affected by conditions that present with chronic wet cough, such as protracted bacterial bronchitis and bronchiectasis. The mortality difference between First Nations and non‐First Nations Australians with bronchiectasis is about 22 years.14 In 180 First Nations children aged <5 years presenting to primary care in urban Queensland for any reason, 24% had a history of chronic cough in the previous 12 months, and at 12‐month follow‐up 26% had a further episode of chronic wet cough.15 Owing to multiple factors, chronic wet cough in First Nations children is often incorrectly considered a normal feature by both families and doctors.16,17 First Nations Australians who have been symptomatic since childhood are more likely to have considerably poorer clinical outcomes in adulthood than those who had onset symptoms in adulthood.18 Box 4 lists potential strategies in combatting chronic wet cough in First Nations patients.
Chronic cough: initial assessment of both children and adults
In both adults and children, estimating duration of cough is critical in assessment.3,22 A chronic cough is defined as a daily cough for >4weeks in children,3 and>8weeks in adults (Box 5).22 The initial assessment for chronic cough relies on history and examination to identify any red flags — indicators that may signal an underlying disease or systemic exposure (Box 6). Probability‐based algorithms are an important clinical decision tool and are presented for both children (Box 1) and adults (Box 2) separately. Initial assessment should always include a chest x‐ray and spirometry (age, >6years).2,3,22 Although a primary diagnosis may be made, it should be remembered that many common conditions co‐exist.
An assessment of risk factors and modification of such exposures is essential to the optimal management of chronic cough (Box 7). These risk factors are mostly common to both children and adults.
Diagnosis and management in children
In children, “specific cough” refers to a cough that occurs with a condition known to be associated with or cause a chronic cough. Identification of the conditions associated with chronic cough forms the basis of specific treatment and investigation. These conditions can usually be identified by cough characteristics and reviewing red flags (Box 6), a probability‐based diagnostic approach (Box 8), and consideration of important conditions not to be missed (Box 9). This approach has been validated in children.3
There is high quality evidence that using children‐specific cough management algorithms improves clinical outcomes, as shown in a systematic review that focused on chronic cough managed by specialists.26 This approach was supported by a randomised controlled trial (RCT) applying the cough management algorithm in community‐based children.12 Box 1 shows the paediatric algorithm, adapted from international ones.3,27,28
Causes of paediatric specific cough
Protracted bacterial bronchitis. This condition is considered in children with a chronic wet cough in the absence of other specific cough diagnoses or red flags.24 Chest x‐ray and spirometry are usually normal. Two to four weeks of antibiotic treatment (typically amoxicillin–clavulanate if no history of allergy) should lead to complete cough resolution29,30 [GRADE: Strong]. The diagnosis can only be definitive when patients become asymptomatic with treatment.24,31 A significant proportion of children with protracted bacterial bronchitis have ongoing symptoms at 5‐year follow‐up, including bronchiectasis in 9.6%; these children therefore require careful follow‐up and specialist referral if episodes recur more than three times per year or treatment fails (Box 1).32
Asthma. Asthma may cause a cough that is episodic and associated with other features such as expiratory wheeze and/or exertional dyspnoea. The diagnosis and management of asthma should be undertaken in accordance with paediatric asthma management guidelines. Treatment is expected to reduce symptoms within 2–4 weeks [GRADE: Strong]. In children, chronic cough in the absence of other symptoms/signs is seldom due to asthma, and inhaled corticosteroids are not indicated unless there are specific features to suggest asthma. When used, the trial period should be of a defined duration (eg, one month) to confirm or refute the provisional diagnosis.27
Allergic rhinitis. The evidence that postnasal drip is a significant cause of cough in children is not fully established, and when present, likely reflects co‐existing upper airway disease. Some paediatric studies reported upper airways cough syndrome as the aetiology of chronic cough,33 but we did not find high quality RCTs on therapies for upper airway disorders in children with cough, and in children, antihistamines have not been shown to be efficacious for the treatment of chronic cough.3 Allergic rhinitis can be diagnosed by symptoms of nasal itching, nasal blockage, or nasal discharge. Management should follow current guidelines [GRADE: Weak].34
Chronic rhinosinusitis. Chronic cough may occur concurrently in children with chronic rhinosinusitis.25 However, any association between rhinosinusitis and cough does not necessarily indicate causality. Notably, the bacterial pathogens associated with chronic rhinosinusitis are the same as those of protracted bacterial bronchitis, hence treatment recommendations for prolonged antibiotics (~2–4 weeks of amoxicillin–clavulanate) are similar.24,35 While there are currently insufficient data, this raises the question of whether the chronic wet cough in children with chronic rhinosinusitis is related to protracted bacterial bronchitis [GRADE: Weak].
Obstructive sleep apnoea. Obstructive sleep apnoea (OSA) is suggested by a history of snoring associated with witnessed apnoeas, sleep disturbance or sweating at night, excessive daytime sleepiness, failure to thrive (in infants), obesity, large tonsils, or nasal blockage. The association between cough and OSA is very weak.36 Hence, in children with OSA and cough, the OSA and cough should be evaluated and treated independently [GRADE: Weak].
Gastro‐oesophageal reflux disease. In children, gastro‐oesophageal reflux disease (GORD) is not commonly identified as a cause of chronic cough.25 There is little current convincing evidence that GORD is a common cause of isolated chronic cough (ie, without gastrointestinal‐related GORD symptoms) and proving causality is difficult.37 Thus, in line with international guidelines,3,33,38 CICADA recommends against empirical treatment for GORD in children with chronic cough and against fundoplication for the treatment of isolated cough in children (Box 10). When symptoms of GORD are present, paediatric GORD guidelines42 should be followed.
Tic and somatic cough syndrome. Tic (habit cough) and somatic cough syndrome (psychogenic cough) are characterised by a continuous, excessive dry barking/honking cough in a child with no red flags in their history or examination. The key indicator is that cough is absent in sleep. Treatment involves suggestion therapy without further investigation [GRADE: Weak].43,44
Non‐specific cough in children
Non‐specific cough is chronic dry cough without any cough pointers or cough‐associated diagnoses, and normal chest x‐ray and spirometry. Most children with non‐specific cough undergo spontaneous resolution or improvement,25 but they need to be reviewed to ensure that no new cough pointers emerge. The management of non‐specific cough adopts the approach of counsel, watch, wait and review [GRADE: Strong], and addresses parental stress and concerns [GRADE: Strong]. At each review, look out for specific pointers (Box 1). CICADA recommends against use of narcotic cough suppressants45 in children [GRADE: Strong].
Diagnosis and management in adults
The assessment of chronic cough in adults includes a history2,22 to define the duration and characteristics of the cough (sputum production, cough hypersensitivity, triggers), to elicit any red flags that suggest underlying disease (Box 6, Box 11)2,46 We recommend a chest x‐ray and spirometry followed by use of a probability‐based algorithm (Box 2) to identify whether these triggers are present and then to manage them to reduce chronic cough (Box 10, Box 12).
Causes of adult chronic cough
Asthma/eosinophilic bronchitis/cough variant asthma. Eosinophilic airway inflammation is found in 30–50% of adults with chronic cough47,48,49 and may reflect asthma, cough variant asthma, and eosinophilic bronchitis. Asthma is diagnosed in 24–32% of adults with chronic cough,48 and is associated with episodic chest tightness, wheeze and dyspnoea.41 Asthma diagnosis relies upon the presence of variable airflow obstruction (as measured by spirometry, peak flow monitoring) or bronchial hyperresponsiveness.39,41,50 Cough variant asthma, a subtype of asthma, is less common and presents solely with cough (without dyspnoea or wheeze), normal spirometry, and a positive bronchial provocation challenge.51 As asthma is commonly associated with chronic cough,19 we recommend spirometry, including post bronchodilator, be considered in the initial assessment of all patients with chronic cough. Eosinophilic bronchitis is characterised by an increase in lower airway eosinophils, normal spirometry, and negative bronchial provocation challenge.48,49 Fractional exhaled nitric oxide (FeNO) has been proposed as a surrogate marker of eosinophilic airway inflammation.2,52 FeNO has good diagnostic accuracy in predicting cough variant asthma, but was less sensitive in predicting eosinophilic bronchitis.53 Treatment of asthma, according to current management guidelines, has been shown to improve chronic cough [GRADE: Strong].
Chronic bronchitis/chronic obstructive pulmonary disease/bronchiectasis. In adults, chronic bronchitis is defined by recurring chronic cough with sputum production54 and has been described with and without chronic obstructive pulmonary disease, bronchiectasis, or a smoking history.55,56 Chronic bronchitis associated with chronic obstructive pulmonary disease and asthma is linked to more frequent exacerbations and worse outcomes.57 It is recommended to treat these underlying disorders [GRADE: Strong]. Non‐smoking adults with chronic bronchitis without airflow obstruction should be investigated for underlying lung disease such as bronchiectasis. Treatments trialled have included mucolytics and/or macrolide antibiotics, but the evidence for their use is scarce [GRADE: Weak].
Interstitial lung disease. Chronic cough that has been reported in up to 80% of people with interstitial lung disease58 is often severe, leads to a significantly impaired quality of life, and is associated with worse clinical outcomes.59
Laryngeal hypersensitivity/intermittent laryngeal obstruction/vocal cord dysfunction. Several well defined clinical syndromes comprise laryngeal dysfunction and often have overlapping symptoms.60 They can also be associated with intermittent laryngeal obstruction, which describes an inappropriate, transient, reversible narrowing of the larynx in response to external triggers. Intermittent laryngeal obstruction is an important cause of chronic cough and dyspnoea and can mimic asthma.61 Speech pathology management including education, vocal hygiene training, breathing techniques, and psycho‐educational counselling are effective in reducing symptoms [GRADE: Strong].
Gastro‐oesophageal reflux disease/airway reflux. The prevalence of chronic cough associated with GORD in adults varies depending on the definition. When this requires the demonstration of acid reflux the prevalence is low;62 however, definitions based on symptoms or oesophageal dysmotility are more frequently associated with chronic cough. A systematic review identified nine RCTs that treated patients with acid suppression and no symptomatic GORD. Only two trials reported a reduction in cough frequency or severity, limited to those with abnormal 24‐hour pH monitoring.63 CICADA recommends against acid suppressive therapy without a history of reflux, or evidence of reflux on objective testing [GRADE: Strong].40
Chronic rhinosinusitis. Chronic rhinosinusitis (allergic or non‐allergic) is found in 12% of people from the United Kingdom presenting with chronic cough,64,65 and treatment follows current evidence‐based guidelines.39 Intranasal corticosteroids are the first line therapy, although evidence they improve chronic cough is weak [GRADE: Weak]. A systematic review of antihistamines66 (ten placebo‐controlled trials in chronic rhinitis, asthma or cough associated with allergy) found treatment led to improved cough symptom scores, although the effect appeared greatest in those with allergy [GRADE: Weak].
Cough hypersensitivity syndrome. Cough hypersensitivity syndrome describes excessive coughing triggered by low levels of thermal, mechanical or chemical stimuli, and can be the result of multiple triggers (Box 11).2,46 Where cough persists beyond management of triggers, it is called unexplained chronic cough.
Adult unexplained chronic cough
Where cough persists despite optimal treatment of diagnosed conditions, it is termed refractory chronic cough (RCC). If no identifiable cause for the cough can be determined, it is termed unexplained chronic cough (UCC), estimated to occur in 10% of adult chronic cough,2,67 and is clinically important.64 We recommend referral for all adults with RCC or UCC to a specialist respiratory clinic.
Therapies for RCC/UCC in adults. Specialists use several options to treat RCC and UCC, including speech therapy and/or antitussive therapies. Two RCTs of speech therapy in adults with RCC or UCC found benefits.68,69 We recommend speech pathology for RCC and UCC [GRADE: Strong], following assessment by respiratory/otolaryngology clinics.
The evidence‐base for antitussive therapies in RCC/UCC is not strong, and a trial of treatment under the supervision of specialist is recommended. The trial should be of sufficient duration to establish efficacy using objective measures of cough severity.70
Inhaled corticosteroids. Inhaled corticosteroids (ICSs) are often trialled in RCC/UCC empirically. A response to treatment should be seen within 4 weeks, and if not evident, ICSs should be ceased. Every effort should be made to diagnose asthma and demonstrate variable airflow obstruction, as this predicts response to ICSs.2 In RCC/UCC, the evidence for empirical ICS use is weak, and there are greater odds of cough improvement with an elevated FeNO (>50ppB) [GRADE: Weak].71
The use of leukotriene receptor antagonists is limited to small open label trials.72 The evidence for their use is weak and may be independent of FeNO [GRADE: Weak].
Antibiotics. A small trial of azithromycin in RCC/UCC found no improvement in cough scores, except for a subgroup with asthma where a significant improvement was seen.73 There is no evidence for other antibiotic regimens. We recommend against the use of empirical antibiotic trials [GRADE: Weak].
Neuromodulators. Two systematic reviews investigating neuromodulators including amitriptyline, gabapentin, pregabalin and baclofen consistently found improvements in cough symptoms and quality of life in RCC/UCC.74,75 A trial of neuromodulators could be considered in RCC/UCC [GRADE: Weak].
Opioids. There are short term trials76 showing that low dose morphine reduces RCC/UCC; however, CICADA recommends against its use in chronic cough given concerns and limitations regarding long term use of opioids [GRADE: Weak].
Specific antitussive therapies. Although the detailed neurophysiology of cough is beyond the scope of this statement, changes in the activity and sensitivity of peripheral and central cough neural circuits are critical to chronic cough pathology and a targetable mechanism. There is emerging evidence for the use of specific antitussive agents for RCC/UCC, but none are yet approved for use in Australia.
Conclusion
Cough is the most common symptom leading to medical consultation. Chronic cough results in significant health care costs, impairs quality of life, and may indicate the presence of a serious underlying condition. We have presented an updated Australian position statement on cough management in the clinical consultation.
The main recommendations are:- Assessment of children and adults requires a focused history of the chronic cough to elicit any red flag cough pointers that may indicate an underlying disease.
- Further assessment with examination should include a chest x‐ray and spirometry (age, >6 years).
- Separate paediatric and adult diagnostic management algorithms should be followed.
- Management of the underlying condition(s) should follow specific disease guidelines, as well as address adverse environmental exposures and patient/carer concerns.
- Aboriginal and Torres Strait Islander adults and children should be considered high risk groups.
Full details of the position statement update, complete reference list, and chronic cough health professional and consumer resources developed in conjunction are available from Lung Foundation Australia at https://lungfoundation.com.au/resources/cicada‐full‐position‐statement.
Box 1 – Algorithm for diagnosis and assessment of a child with chronic cough
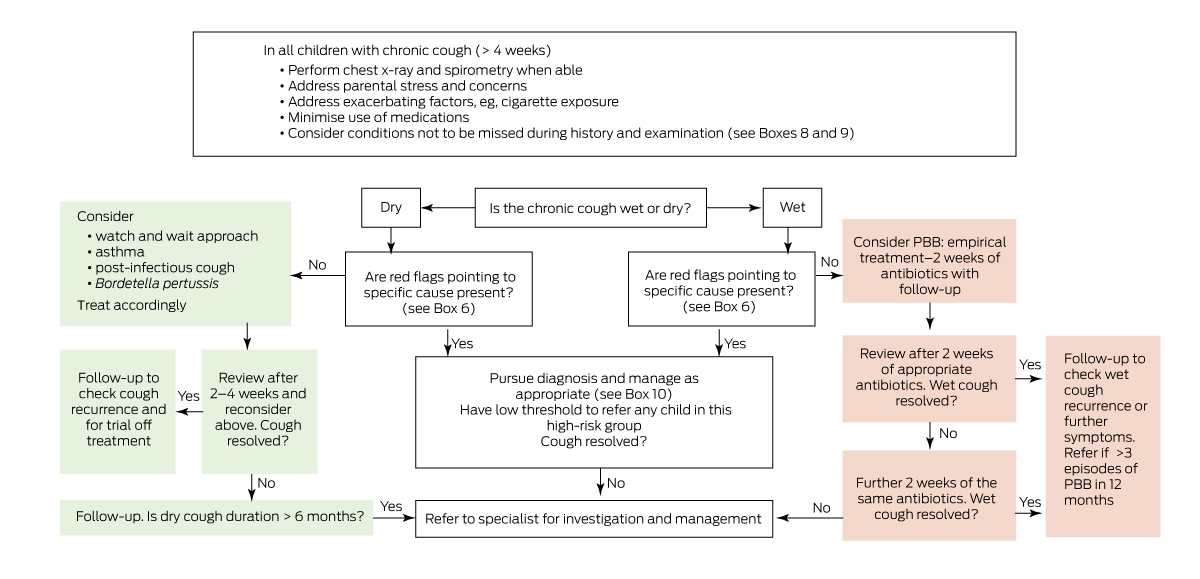
PBB = protracted bacterial bronchitis
Box 2 – Algorithm for diagnosis and assessment of an adult with chronic cough
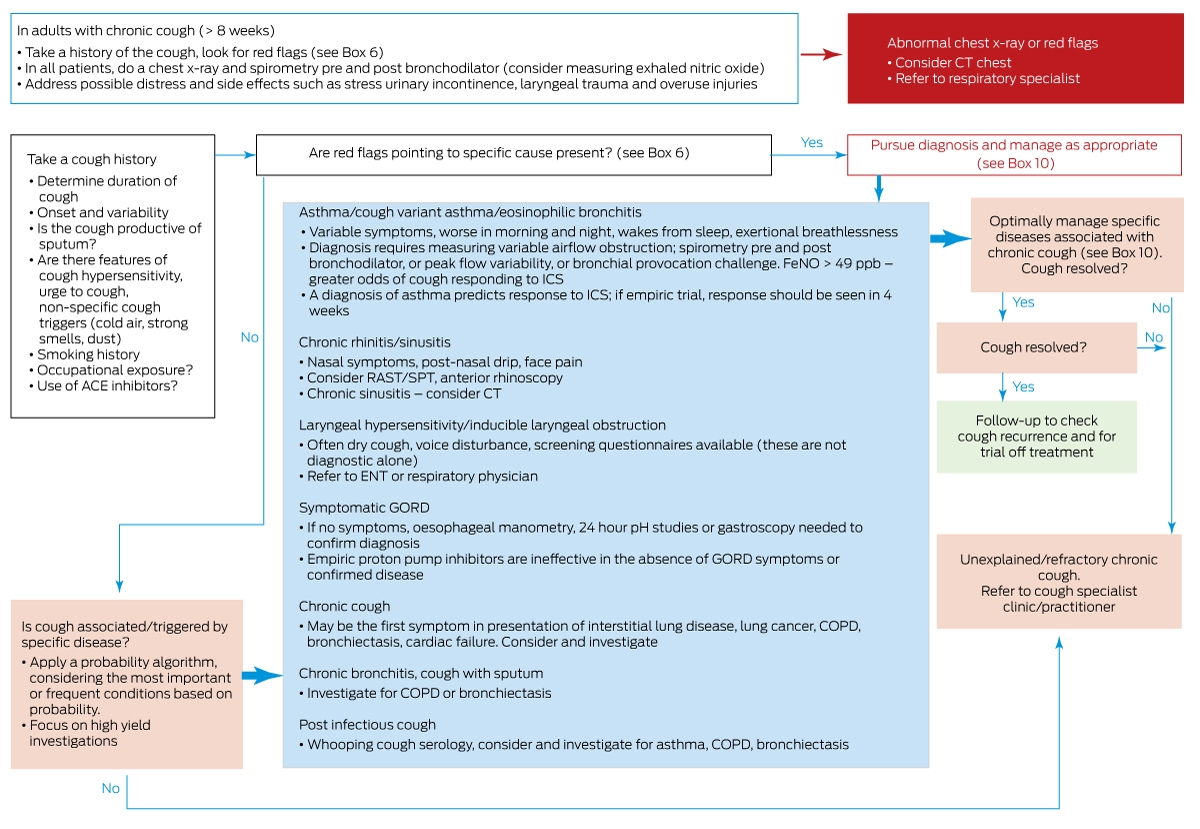
ACE = angiotensin‐converting enzyme; COPD = chronic obstructive pulmonary disease; CT = computed tomography; ENT = ear, nose and throat; ICS = inhaled corticosteroids; FeNO = fractional exhaled nitric oxide; GORD = gastro‐oesophageal reflux disease; ppb = parts per billion; RAST = radioallergosorbent test; SPT = skin prick test.
Box 3 – Guideline development process
- From Jan 2021 to December 2022, members of the CICADA committee regularly convened (email, face‐to‐face, virtual meetings) to undertake an extensive literature review and discuss recommendations.
- The committee included several working groups (children, adult, epidemiology and prevention, overall approach) who undertook systematic searches for relevant literature published since 2010 (the previous CICADA update),4 including but not limited to “all RCTs, systematic reviews, guidelines, position statements in any setting”.
- Databases searched included OVID MEDLINE, PubMed, the Cochrane Library, and Embase. Search results were then screened (total 6395 abstracts); a total of 277 new studies were included in this statement. The search strategies, PRISMA diagrams, full reference list of included evidence, and complete guideline document are available on the Australian Lung Foundation website at https://lungfoundation.com.au/resources/cicada‐full‐position‐statement/.
- The recommendations use the principles of evidence‐based medicine5 and the GRADE approach to guide recommendations to inform the strength of the evidence: strong, weak, or no specific recommendation.6
-
The implications of strong recommendation are:
- ‣ for patients — most people in your situation would want the recommended course of action and only a small proportion would not; suggest request discussion if the intervention is not offered
- ‣ for clinicians — most patients should receive this recommended course of action
- ‣ for policy makers — the recommendation can be adopted as a policy in most situations.
-
The implications of a weak recommendation are:
- ‣ for patients — some people in your situation would want the recommended course of action, but many would not
- ‣ for clinicians — you should recognise that different choices will be appropriate for different patients and that you must help each patient to arrive at a management decision consistent with their values and preferences
- ‣ for policy makers — policy making will require substantial debate.
Box 4 – Specific recommendations for addressing chronic cough in First Nations people
Recommendations |
Level of evidence* |
Strength of recommendation† | |||||||||||||
Address environmental factors: air quality (airborne particulate matter), cigarette smoke exposure (patient, parental, household)19 |
Good |
Strong |
|||||||||||||
Provide culturally secure health information to facilitate detection of chronic wet cough: accurate history taking in First Nations settings, provision of appropriate health information in a culturally secure way, community engagement at a local level20 |
Satisfactory |
Strong |
|||||||||||||
Implement strategies in health systems that include targeted training of clinicians; implementation programs that include targeted training of clinicians, health system changes and the provision of culturally secure health information tools have been shown to improve physician assessment of chronic cough and appropriate antibiotic prescription20 |
Satisfactory |
Strong |
|||||||||||||
Utilise chronic cough management algorithms; randomised controlled trials including First Nations children have shown the effectiveness of management algorithms for chronic cough, usual care12,21 |
Excellent |
Strong |
|||||||||||||
* NHMRC additional levels of evidence and grades for recommendations for developers of guidelines.5 † The GRADE (Grading of Recommendations Assessment, Development and Evaluation) system was used to grade the strength of recommendations.6 | |||||||||||||||
Box 5 – Definitions of cough3,22
- Cough: protective respiratory behaviour of forced expulsion of air against a closed glottis
- Acute cough: cough lasting up to 2 weeks
-
Protracted acute cough:
- ‣ in children — cough lasting 2 to 4 weeks
- ‣ in adults — cough lasting 2 to 8 weeks
-
Chronic cough:
- ‣ in children — cough lasting more than 4 weeks
- ‣ in adults — cough lasting more than 8 weeks
Box 6 – Red flags and cough pointers (indicators of serious pathology)
Children 23- Dyspnoea (at rest or exertional)
- Recurrent episodes of chronic or wet or productive cough
- Recurrent pneumonia
- Chest pain
- Haemoptysis
- Systemic symptoms: fever, weight loss, growth failure
- Neurodevelopmental abnormality
- Feeding difficulties (including choking/vomiting)
- Stridor and other respiratory noises
- Abnormal clinical respiratory examination (eg, crackles, digital clubbing)
- Abnormal systemic examination (eg, growth failure)
- Abnormal chest x‐ray
- Abnormal lung function
- Co‐existing chronic diseases (eg, immunodeficiency, syndromes)
- Haemoptysis
- Smoking/vaping (especially new/altered cough, cough with voice disturbance)
- Prominent dyspnoea (especially at rest or at night)
- Chronic productive cough with substantial sputum production
- Hoarseness
- Recurrent pneumonia
- Systemic symptoms: fever, weight loss
- Swallowing difficulties (including choking/vomiting)
- Abnormal clinical respiratory examination (eg, crackles, wheeze, digital clubbing)
- Abnormal chest radiograph
Box 7 – Preventive strategies for chronic cough
- Immunisations: pneumococcus, Haemophilus influenzae, Bordetella pertussis, influenza
-
Avoidance of airway pollutants, irritants and triggers:
- ‣ cigarette smoke, wood‐fire smoke, e‐cigarettes
- ‣ fumes, strong odours, subfreezing air
- ‣ for those susceptible, animals, pollens, and other allergens
-
Health education:
- ‣ early clinical review and adequate treatment of a chronic wet cough including post‐acute respiratory infection (>4 weeks in children, >8 weeks in adults)
- ‣ workplace education about hazard minimisation for workers in high risk occupations
Box 8 – Probability‐based diagnosis of chronic cough in children
If the examination, chest x‐ray and spirometry are normal, the most common diagnoses and exposures associated with chronic cough in children are:- Diagnoses:
- Exposures:21
- ‣ Respiratory infection (post‐infectious cough, including pertussis)
- ‣ Tobacco smoke or e‐cigarettes/vaping and other pollutants (active, environmental) can exacerbate chronic cough but are rarely the cause
Box 9 – Significant conditions in children with chronic cough3,25
Condition |
Typical symptoms | ||||||||||||||
Diagnoses with specific removable causes or usually good treatment response |
|||||||||||||||
Protracted bacterial bronchitis |
Wet/productive cough and no other systemic symptoms or signs24 |
||||||||||||||
Asthma |
Recurrent wheeze and/or dyspnoea responsive to β2 agonists |
||||||||||||||
Tic (habit cough) and somatic cough syndrome (psychogenic cough) |
Continuous, excessive dry cough with no sign of physical disease; stops when asleep or distracted |
||||||||||||||
Significant conditions not to be missed |
|||||||||||||||
Congenital airway abnormalities |
Symptoms commencing in infancy/early childhood |
||||||||||||||
Recurrent aspiration |
Cough or choking with feeds |
||||||||||||||
Foreign body inhalation |
Symptoms commenced after choking episode |
||||||||||||||
Chronic infection |
|||||||||||||||
Tuberculosis |
Focal signs, weight loss lymphadenopathy, contact history |
||||||||||||||
Lung abscess |
Fever and local signs |
||||||||||||||
Pertussis |
Dry cough, contact history; paroxysms in unvaccinated children |
||||||||||||||
Bronchiectasis/chronic suppurative lung disease/cystic fibrosis |
Wet cough not responding to 4 weeks of antibiotics or recurring |
||||||||||||||
Chronic atelectasis |
Focal signs on auscultation |
||||||||||||||
Interstitial lung disease |
Diffuse inspiratory crepitations growth failure with or without hypoxia |
||||||||||||||
Box 10 – Strength of recommendations for the efficacy of treatment of cough in association with the conditions
Recommendations |
Level of evidence* |
Strength of recommendation† | |||||||||||||
Children |
|||||||||||||||
Cessation of parental smoking to reduce cough |
Good |
Strong |
|||||||||||||
Cough with allergic rhinitis |
|||||||||||||||
Treatment according to current rhinitis management guidelines involving topical nasal corticosteroid, antihistamines, and allergen management |
Poor |
Weak |
|||||||||||||
Cough with obstructive sleep apnoea |
|||||||||||||||
Tonsillectomy and adenoidectomy |
Poor |
Weak |
|||||||||||||
Cough with asthma |
|||||||||||||||
Treatment according to current asthma management guidelines involving education and self‐management, inhaled bronchodilators, and inhaled corticosteroids; if empirical treatment is used, review in 2–4 weeks |
Good |
Strong |
|||||||||||||
Cough with protracted bacterial bronchitis |
|||||||||||||||
Medium term (2–4 weeks) antibiotics for protracted bacterial bronchitis |
Excellent |
Strong |
|||||||||||||
Cough with GORD |
|||||||||||||||
Treatment(s) for GORD should not be used when there are no gastro‐intestinal clinical features of GORD; paediatric GORD guidelines should be used to guide treatment and investigations |
Good |
Weak |
|||||||||||||
Treatment with laparoscopic fundoplication |
Poor |
Strong recommendation against |
|||||||||||||
Non‐specific or refractory cough |
|||||||||||||||
Address patient/parental stress and concerns |
Poor |
Strong |
|||||||||||||
Address exacerbating factors, such as tobacco smoke exposure |
Good |
Strong |
|||||||||||||
Minimise use of medications other than demulcents (eg, honey) if no contraindications (young age) exist |
Good |
Strong |
|||||||||||||
Adopt counsel, watch, wait and review approach |
Excellent |
Strong |
|||||||||||||
Empirical trial of inhaled corticosteroid therapy |
Poor |
No recommendation |
|||||||||||||
Empirical trial of proton pump inhibitors |
Good |
Strong recommendation against |
|||||||||||||
Speech pathology techniques designed to relieve glottal constriction during inspiration and to recognise and alter response to precipitants |
Poor |
No recommendation |
|||||||||||||
Antitussive therapy with narcotic |
Good |
Strong recommendation against |
|||||||||||||
Adults |
|||||||||||||||
Cough with allergic rhinitis |
|||||||||||||||
Treatment according to current rhinitis management guidelines39 involving nasal corticosteroid spray, nasal antihistamine spray, combination corticosteroid/antihistamine nasal spray |
Good |
Weak |
|||||||||||||
Cough with chronic rhinosinusitis |
|||||||||||||||
Treatment according to current chronic sinusitis management guidelines39 involving nasal corticosteroid spray, large volume saline irrigation, long term antibiotic therapy (macrolide, 3 months) |
Poor |
Weak |
|||||||||||||
Cough with laryngeal hypersensitivity |
|||||||||||||||
Treatment with speech pathology management |
Good |
Strong |
|||||||||||||
Cough with vocal cord dysfunction/intermittent laryngeal obstruction |
|||||||||||||||
Treatment with speech pathology management |
Good |
Strong |
|||||||||||||
Cough with GORD/dysmotility |
|||||||||||||||
Treatment(s) for GORD in adults with cough alone and no other symptoms of GORD with PPI therapy; when other symptoms of GORD occur, use appropriate clinical guidelines40 |
Good |
Strong recommendation against use of PPI for cough alone |
|||||||||||||
Cough with asthma |
|||||||||||||||
Treatment according to current asthma management guidelines41 involving education, inhaled bronchodilators, inhaled corticosteroids |
Excellent |
Strong |
|||||||||||||
Leukotriene receptor antagonists, alone or with inhaled corticosteroids |
Good |
Weak |
|||||||||||||
Cough with eosinophilic bronchitis |
|||||||||||||||
Treatment with inhaled corticosteroids |
Satisfactory |
Strong |
|||||||||||||
Leukotriene receptor antagonists, alone or with inhaled corticosteroids |
Satisfactory |
Weak |
|||||||||||||
Cough with chronic bronchitis without airflow obstruction |
|||||||||||||||
Mucolytic therapy and/or macrolide antibiotic therapy |
Poor |
Weak |
|||||||||||||
Cough with ILD |
|||||||||||||||
Treatment according to current ILD guidelines |
Poor |
Weak |
|||||||||||||
Cough with COPD |
|||||||||||||||
Treatment according to current COPD management guidelines involving education and self‐management, smoking cessation, pulmonary rehabilitation and treatment of exacerbations |
Excellent |
Strong |
|||||||||||||
Addition of combination inhaled long‐acting bronchodilators and corticosteroids may reduce cough severity |
Good |
Weak |
|||||||||||||
Cough with bronchiectasis |
|||||||||||||||
Treatment according to current bronchiectasis management guidelines involving treatment of exacerbations with 14 days antibiotics, regular airway clearance and pulmonary rehabilitation |
Good |
Weak |
|||||||||||||
Unexplained chronic cough |
|||||||||||||||
An empirical treatment trial supervised by a specialist cough clinic using validated, objective measures of cough severity (cough severity scales, the cough severity diary, quality‐of‐life measures [Leicester cough questionnaire, cough specific quality of life questionnaire], objective cough recording devices and cough reflex sensitivity challenges) |
Satisfactory |
Weak |
|||||||||||||
Cessation of smoking, nicotine containing cigarettes or e‐cigarettes |
Excellent |
Strong |
|||||||||||||
Identify and minimise environmental/occupational exposures |
Satisfactory |
Weak |
|||||||||||||
Cessation of angiotensin‐converting enzyme inhibitors |
Satisfactory |
Strong |
|||||||||||||
Speech and language therapy |
Excellent |
Strong |
|||||||||||||
Inhaled corticosteroids or leukotriene antagonist empirical treatment trial |
Poor |
Weak |
|||||||||||||
Macrolide antibiotics |
Satisfactory |
Weak recommendation against |
|||||||||||||
Acid suppressive therapy, proton pump inhibitors, or H2 antagonist empirical treatment trial |
Excellent |
Strong recommendation against |
|||||||||||||
Neuromodulators (amitriptyline, gabapentin, pregabalin) treatment trial |
Satisfactory |
Weak |
|||||||||||||
Opioids empirical treatment trial |
Satisfactory |
Weak recommendation against |
|||||||||||||
COPD = chronic obstructive pulmonary disease; GORD = gastro‐oesophageal reflux disease; H2 = histamine type 2; ILD = interstitial lung disease; PPI = proton pump inhibitor. * NHMRC additional levels of evidence and grades for recommendations for developers of guidelines.5 † GRADE (Grading of Recommendations Assessment, Development and Evaluation) system.6 | |||||||||||||||
Box 11 – Conditions associated with chronic cough in adults
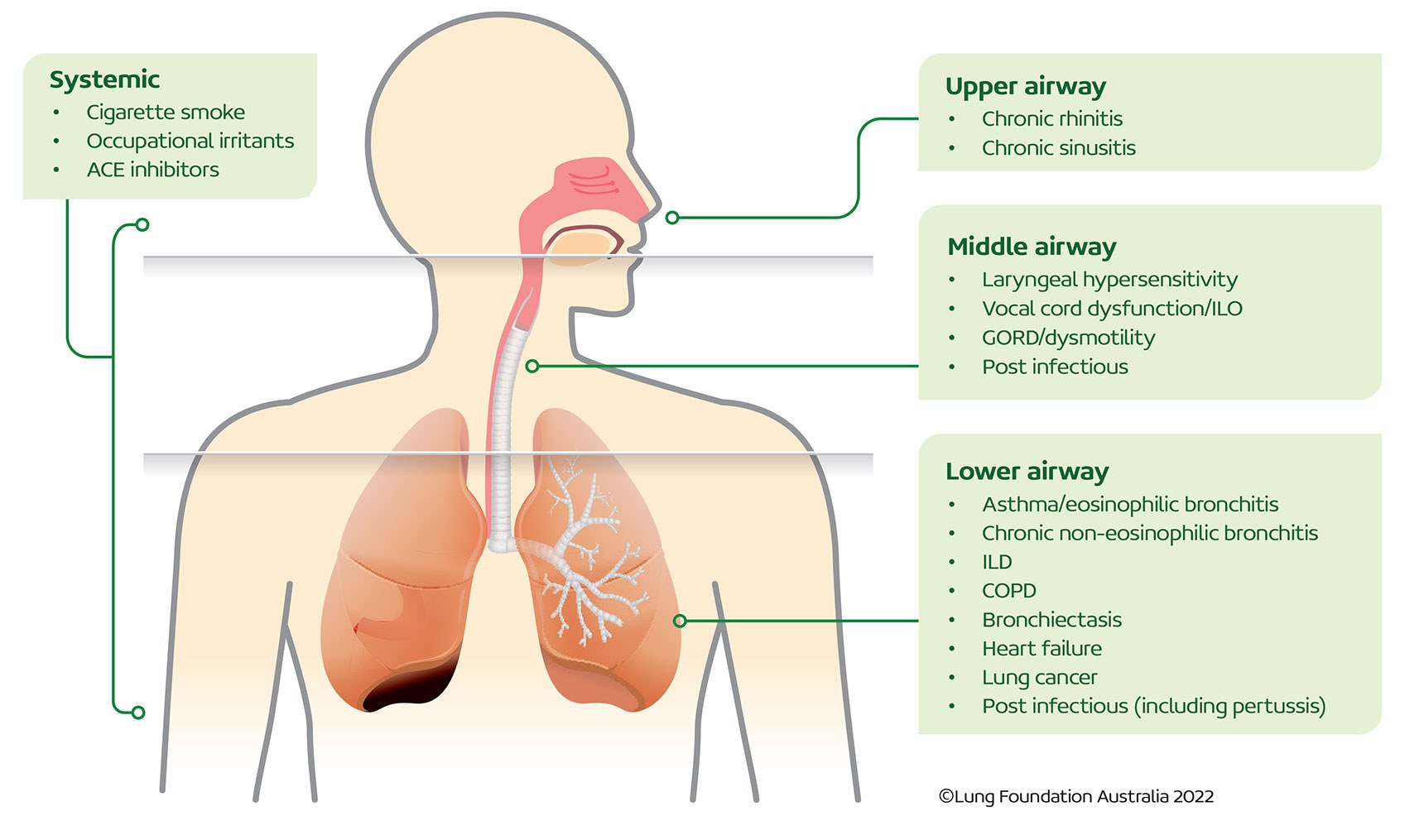
ACE = angiotensin‐converting enzyme; COPD = chronic obstructive pulmonary disease; GORD = gastro‐oesophageal reflux disease; ILD = interstitial lung disease; ILO = intermittent laryngeal obstruction. Reproduced with permission from Lung Foundation Australia.
Box 12 – Conditions associated with chronic cough in adults
Condition |
Key features |
Investigations | |||||||||||||
Chronic rhinitis |
Nasal obstruction (variable or persistent), loss of smell, nasal discharge |
RAST/SPT
|
|||||||||||||
Chronic sinusitis |
Nasal obstruction, and at least one other of nasal discharge, postnasal drip, reduction/loss of sense of smell, facial pain |
RAST/SPT
|
|||||||||||||
Laryngeal hypersensitivity |
Hypersensitive cough reflex, allotussia |
Laryngeal Hypersensitivity Questionnaire |
|||||||||||||
Vocal cord dysfunction/inspiratory laryngeal obstruction |
|
Functional laryngoscopy
|
|||||||||||||
GORD/dysmotility |
Heartburn, reflux symptoms
|
Oesophageal manometry
|
|||||||||||||
Post infectious |
Post acute respiratory illness |
Bordetella pertussis serology
|
|||||||||||||
Asthma/cough variant asthma/eosinophilic bronchitis without asthma |
Wheeze, dyspnoea
|
Spirometry (bronchodilator reversibility)
|
|||||||||||||
Chronic non‐eosinophilic bronchitis |
Sputum production without airflow obstruction |
Spirometry: pre/post bronchodilator to exclude asthma and COPD
|
|||||||||||||
Interstitial lung disease |
Presence of dyspnoea |
HRCT chest, history (exposures, serology) |
|||||||||||||
COPD |
Exertional dyspnoea, sputum production, history of smoking/exposure to noxious agents |
Spirometry (post bronchodilator FEV1/FVC<0.7) |
|||||||||||||
Bronchiectasis |
Sputum production, chronic bronchial infection |
HRCT chest |
|||||||||||||
Congestive cardiac failure |
Dyspnoea, peripheral oedema, crackles +/‐wheeze on auscultation |
ECG, CXR, BNP or
|
|||||||||||||
Lung cancer |
Haemoptysis, dyspnoea, chest pain, history of smoking, constitutional symptoms |
CT scan of the chest, bronchoscopy, PET scan |
|||||||||||||
BNP = B‐type natriuretic peptide; COPD = chronic obstructive pulmonary disease; CT = computed tomography; CXR = chest x‐ray; ECG = electrocardiogram; FeNO = fractional exhaled nitric oxide; FEV1 = forced expiratory volume; FVC = forced vital capacity; GORD = gastro‐oesophageal reflux disease; HRCT = high resolution computed tomography; NT‐BNP = N‐terminal pro hormone BNP; PET = positron emission tomography; RAST = radioallergosorbent test; SPT = skin prick test. | |||||||||||||||
Competing interests
The authors received no specific funding for this work. Julie Marchant is supported by the Lung Foundation Australia Hope Research Fund Andrew Harrison Fellowship in Bronchiectasis Research 2021 and receives personal fees from being an author of two UpToDate chapters, outside of the submitted work. Anne Chang reports multiple grants from the National Health and Medical Research Council (NHMRC) during the conduct of this work; is an independent data monitoring committee member for an unlicensed vaccine (GSK) and an unlicensed monoclonal antibody (AstraZeneca); is an advisory member on the study design for an unlicensed molecule for chronic cough (Merck); and has received personal fees from being an author of two UpToDate chapters, outside the submitted work. Andre Schultz receives salary support from a Medical Research Future Fund Investigator Grant (APP1193796). Danielle Wurzel has received research grants from the NHMRC and GSK, and honoraria from Merck and MSD. Stuart Mazzone has received honoraria from Merck, NeRRe Therapeutics, Reckitt Benckiser and Bellus Health for consultancy on their antitussive programs, and antitussive‐related grant support from Merck, Bellus Health and Reckitt Benckiser, as well as multiple grants from the NHMRC and the Australian Research Council. Shyamali Dharmage has received multiple grants from the NHMRC and the Australian Research Council, including the NHMRC Investigator Grant (APP1193993) that currently supports her. Additionally, Shyamali Dharmage and Jennifer Perret have received independent investigator‐initiated grants from AstraZeneca and GSK for unrelated research. Jennifer Perret is supported by an NHMRC Early Career Fellowship (APP1159090). Johnson George has received honoraria through consultations for AstraZeneca, GSK and Pfizer which have been paid to his employer, and has held research grants from Boehringer Ingelheim, GSK and Pfizer through investigator‐initiated research schemes. All other authors have no conflicts of interest to declare in relation to this work.
Acknowledgements
We thank Lung Foundation Australia and the Thoracic Society of Australia and New Zealand for their support in the preparation of these guidelines.
References
- Gibson P, Wang G, McGarvey L, et al. Treatment of unexplained chronic cough: CHEST guideline and expert panel report. Chest 2016; 149: 27‐44.
- Morice AH, Millqvist E, Bieksiene K, et al. ERS guidelines on the diagnosis and treatment of chronic cough in adults and children. Eur Respir J 2020; 55: 1901136.
- Chang AB, Oppenheimer JJ, Irwin RS. Managing chronic cough as a symptom in children and management algorithms: CHEST guideline and expert panel report. Chest 2020; 158: 303‐329.
- Gibson PG, Chang AB, Glasgow NJ, et al. CICADA: Cough in Children and Adults: Diagnosis and Assessment. Australian cough guidelines summary statement. Med J Aust 2010; 192: 265‐271. https://www.mja.com.au/journal/2010/192/5/cicada‐cough‐children‐and‐adults‐diagnosis‐and‐assessment‐australian‐cough
- National Health and Medical Research Council. NHMRC levels of evidence and grades for recommendations for developers of guidelines. 2009. https://www.mja.com.au/sites/default/files/NHMRC.levels.of.evidence.2008‐09.pdf (viewed Oct 2023).
- Andrews J, Guyatt G, Oxman AD, et al. GRADE guidelines: 14. Going from evidence to recommendations: the significance and presentation of recommendations. J Clin Epidemiol 2013; 66: 719‐725.
- Song WJ, Chang YS, Faruqi S, et al. The global epidemiology of chronic cough in adults: a systematic review and meta‐analysis. Eur Respir J 2015; 45: 1479‐1481.
- Alif SM, Dharmage SC, Benke G, et al. Occupational exposure to pesticides are associated with fixed airflow obstruction in middle‐age. Thorax 2017; 72: 990‐997.
- Morice AH, Jakes AD, Faruqi S, et al. A worldwide survey of chronic cough: a manifestation of enhanced somatosensory response. Eur Respir J 2014; 44: 1149‐1155.
- Colak Y, Nordestgaard BG, Laursen LC, et al. Risk factors for chronic cough among 14,669 individuals from the general population. Chest 2017; 152: 563‐573.
- Chung KF, McGarvey L, Song WJ, et al. Cough hypersensitivity and chronic cough. Nat Rev Dis Primers 2022; 8: 45.
- O'Grady KF, Grimwood K, Torzillo PJ, et al. Effectiveness of a chronic cough management algorithm at the transitional stage from acute to chronic cough in children: a multicenter, nested, single‐blind, randomised controlled trial. Lancet Child Adolesc Health 2019; 3: 889‐898.
- Laird P, Totterdell J, Walker R, et al. Prevalence of chronic wet cough and protracted bacterial bronchitis in Aboriginal children. ERJ Open Res 2019; 5: 00248‐2019.
- McCallum GB, Chang AB. ‘Good enough’ is ‘not enough’ when managing indigenous adults with bronchiectasis in Australia and New Zealand. Respirology 2018; 23: 725‐726.
- Hall KK, Chang AB, Anderson J, et al. Characteristics and respiratory risk profile of children aged less than 5 years presenting to an urban, Aboriginal‐friendly, comprehensive primary health practice in Australia. J Paediatr Child Health 2017; 53: 636‐643.
- Laird P, Walker R, Lane M, et al. We won't find what we don't look for: Identifying barriers and enablers of chronic wet cough in Aboriginal children. Respirology 2020; 25: 383‐392.
- D'Sylva P, Walker R, Lane M, et al. Chronic wet cough in Aboriginal children: it's not just a cough. J Paediatr Child Health 2019; 55: 833‐843.
- King PT, Holdsworth SR, Farmer M, et al. Phenotypes of adult bronchiectasis: onset of productive cough in childhood and adulthood. COPD 2009; 6: 130‐136.
- Zhang J, Perret JL, Chang AB, et al. Risk factors for chronic cough in adults: a systematic review and meta‐analysis. Respirology 2022; 27: 36‐47.
- Laird P, Walker R, Lane M, et al. Recognition and management of protracted bacterial bronchitis in Australian Aboriginal children: a knowledge translation approach. Chest 2021; 159: 249‐258.
- Chang AB, Robertson CF, Van Asperen PP, et al. A multicenter study on chronic cough in children: burden and etiologies based on a standardized management pathway. Chest 2012; 142: 943‐950.
- Irwin RS, French CL, Chang AB, Altman KW. Classification of cough as a symptom in adults and management algorithms: CHEST guideline and expert panel report. Chest 2018; 153: 196‐209.
- Chang AB, Van Asperen PP, et al. Children with chronic cough: when is watchful waiting appropriate? Development of likelihood ratios for assessing children with chronic cough. Chest 2015; 147: 745‐753.
- Chang AB, Oppenheimer JJ, Weinberger MM, et al. Management of children with chronic wet cough and protracted bacterial bronchitis: CHEST guideline and expert panel report. Chest 2017; 151: 884‐890.
- Chang AB, Oppenheimer JJ, Weinberger M, et al. Etiologies of chronic cough in pediatric cohorts: CHEST guideline and expert panel report. Chest 2017; 152: 607‐617.
- Chang AB, Oppenheimer JJ, Weinberger M, et al. Use of management pathways or algorithms in children with chronic cough: systematic reviews. Chest 2016; 149: 106‐119.
- Chang AB, Oppenheimer JJ, Weinberger MM, et al. Use of management pathways or algorithms in children with chronic cough: CHEST guideline and expert panel report. Chest 2017; 151: 875‐883.
- Alsubaie H, Al‐Shamrani A, Alharbi AS, Alhaider S. Clinical practice guidelines: approach to cough in children: the official statement endorsed by the Saudi Pediatric Pulmonology Association (SPPA). Int J Pediatr Adolesc Med 2015; 2: 38‐43.
- Marchant JM, Petsky HL, Morris PS, Chang AB. Antibiotics for prolonged wet cough in children. Cochrane Database Syst Rev 2018; (7): CD004822.
- Ruffles TJC, Goyal V, Marchant JM, et al. Duration of amoxicillin‐clavulanate for protracted bacterial bronchitis in children (DACS): a multi‐centre, double blind, randomised controlled trial. Lancet Respir Med 2021; 9: 1121‐1129.
- Kantar A, Chang AB, Shields MD, et al. ERS statement on protracted bacterial bronchitis in children. Eur Respir J 2017; 50: 1602139.
- Ruffles TJC, Marchant JM, Masters IB, et al. Outcomes of protracted bacterial bronchitis in children: a 5‐year prospective cohort study. Respirology 2021; 26: 241‐248.
- Marseglia GL, Manti S, Chiappini E, et al. Chronic cough in childhood: a systematic review for practical guidance by the Italian Society of Pediatric Allergy and Immunology. Allergol Immunopathol (Madr) 2021; 49: 133‐154.
- Dykewicz MS, Wallace DV, Baroody F, et al. Treatment of seasonal allergic rhinitis: an evidence‐based focused 2017 guideline update. Ann Allergy Asthma Immunol 2017; 119: 489‐511.e41.
- Brietzke SE, Shin JJ, Choi S, et al. Clinical consensus statement: pediatric chronic rhinosinusitis. Otolaryngol Head Neck Surg 2014; 151: 542‐553.
- Teoh L, Hurwitz M, Acworth JP, et al. Treatment of obstructive sleep apnoea for chronic cough in children. Cochrane Database Syst Rev 2011; (4): CD008182.
- de Benedictis FM, Bush A. Respiratory manifestations of gastro‐oesophageal reflux in children. Arch Dis Child 2018; 103: 292‐296.
- Chang AB, Oppenheimer JJ, Kahrilas PJ, et al. Chronic cough and gastroesophageal reflux in children: CHEST guideline and expert panel report. Chest 2019; 156: 131‐40.
- Australasian Society of Clinical Immunology and Allergy. ASCIA Information for Health Professionals: Chronic rhinosinusitis with nasal polyps (CRSwNP) position paper. 2021. https://www.allergy.org.au/images/stories/pospapers/ASCIA_HP_Position_Paper_CRSwNP_2021.pdf (viewed Oct 2023).
- Kahrilas PJ, Altman KW, Chang AB, et al. Chronic cough due to gastroesophageal reflux in adults: CHEST guideline and expert panel report. Chest 2016; 150: 1341‐1360.
- National Asthma Council. Australian Asthma Handbook: Making a diagnosis of asthma in adults. https://www.asthmahandbook.org.au/diagnosis/adults/making‐a‐diagnosis (viewed Oct 2023).
- National Institute for Health and Care Excellence. Gastro‐oesophageal reflux disease in children and young people. NICE Guideline [NG1]. Published 14 Jan 2015; last updated 9 Oct 2019. https://www.nice.org.uk/guidance/ng1 (viewed Oct 2023).
- Weinberger M. The habit cough: diagnosis and treatment. Pediatr Pulmonol 2018; 53: 535‐537.
- Vertigan AE, Murad MH, Pringsheim T, et al. Somatic cough syndrome (previously referred to as psychogenic cough) and tic cough (previously referred to as habit cough) in adults and children: CHEST guideline and expert panel report. Chest 2015; 148: 24‐31.
- Gardiner SJ, Chang AB, Marchant JM, Petsky HL. Codeine versus placebo for chronic cough in children. Cochrane Database Syst Rev 2016; (7): CD011914.
- McGarvey L, Gibson PG. What is chronic cough? terminology. J Allergy Clin Immunol Pract 2019; 7: 1711‐1714.
- Gibson PG, Dolovich J, Denburg J, et al. Chronic cough: eosinophilic bronchitis without asthma. Lancet 1989; 1: 1346‐1348.
- Carney IK, Gibson PG, Murree‐Allen K, et al. A systematic evaluation of mechanisms in chronic cough. Am J Respir Crit Care Med 1997; 156: 211‐216.
- Brightling CE. Chronic cough due to nonasthmatic eosinophilic bronchitis: ACCP evidence‐based clinical practice guidelines. Chest 2006; 129 (1 Suppl): 116S‐121S.
- Australian Medicines Handbook. Last modified: July 2023. https://amhonline.amh.net.au/ (viewed Oct 2023).
- Corrao WM, Braman SS, Irwin RS. Chronic cough as the sole presenting manifestation of bronchial asthma. N Engl J Med 1979; 300: 633‐637.
- Chen LC, Zeng GS, Wu LL, et al. Diagnostic value of FeNO and MMEF for predicting cough variant asthma in chronic cough patients with or without allergic rhinitis. J Asthma 2021; 58: 326‐333.
- Song WJ, Kim HJ, Shim JS, et al. Diagnostic accuracy of fractional exhaled nitric oxide measurement in predicting cough‐variant asthma and eosinophilic bronchitis in adults with chronic cough: a systematic review and meta‐analysis. J Allergy Clin Immunol 2017; 140: 701‐709.
- Kim V, Crapo J, Zhao H, et al. Comparison between an alternative and the classic definition of chronic bronchitis in COPDGene. Ann Am Thorac Soc 2015; 12: 332‐339.
- Balte PP, Chaves PHM, Couper DJ, et al. Association of nonobstructive chronic bronchitis with respiratory health outcomes in adults. JAMA Intern Med 2020; 180: 676‐686.
- Çolak Y, Nordestgaard BG, Vestbo J, et al. Prognostic significance of chronic respiratory symptoms in individuals with normal spirometry. Eur Respir J 2019; 54: 1900734.
- Hughes R, Rapsomaniki E, Janson C, et al. Frequent productive cough: symptom burden and future exacerbation risk among patients with asthma and/or COPD in the NOVELTY study. Respir Med 2022; 200: 106921.
- Ryerson CJ, Abbritti M, Ley B, et al. Cough predicts prognosis in idiopathic pulmonary fibrosis. Respirology 2011; 16: 969‐975.
- Lee J, White E, Freiheit E, et al. Cough‐specific quality of life predicts disease progression among patients with interstitial lung disease: data from the Pulmonary Fibrosis Foundation Patient Registry. Chest 2022; 162: 603‐613.
- Vertigan AE, Bone SL, Gibson PG. Laryngeal sensory dysfunction in laryngeal hypersensitivity syndrome. Respirology 2013; 18: 948‐956.
- Halvorsen T, Walsted ES, Bucca C, et al. Inducible laryngeal obstruction: an official joint European Respiratory Society and European Laryngological Society statement. Eur Respir J 2017; 50: 1602221.
- Irwin RS, French CL, Curley FJ, et al. Chronic cough due to gastroesophageal reflux. Clinical, diagnostic, and pathogenetic aspects. Chest 1993; 104: 1511‐1517.
- Kahrilas PJ, Howden CW, Hughes N, Molloy‐Bland M. Response of chronic cough to acid‐suppressive therapy in patients with gastroesophageal reflux disease. Chest 2013; 143: 605‐612.
- Hull JH, Langerman H, Ul‐Haq Z, et al. Burden and impact of chronic cough in UK primary care: a dataset analysis. BMJ Open 2021; 11: e054832.
- Dietz de Loos DA, Hopkins C, Fokkens WJ. Symptoms in chronic rhinosinusitis with and without nasal polyps. Laryngoscope 2013; 123: 57‐63.
- Lee JH, Lee JW, An J, et al. Efficacy of non‐sedating H1‐receptor antihistamines in adults and adolescents with chronic cough: a systematic review. World Allergy Organ J 2021; 14: 100568.
- Usta Guc B, Asilsoy S, Durmaz C. The assessment and management of chronic cough in children according to the British Thoracic Society guidelines: descriptive, prospective, clinical trial. Clin Respir J 2014; 8: 330‐337.
- Vertigan AE, Theodoros DG, Gibson PG, Winkworth AL. Efficacy of speech pathology management for chronic cough: a randomised placebo controlled trial of treatment efficacy. Thorax 2006; 61: 1065‐1069.
- Chamberlain Mitchell SA, Garrod R, Clark L, et al. Physiotherapy, and speech and language therapy intervention for patients with refractory chronic cough: a multicentre randomised control trial. Thorax 2017; 72: 129‐136.
- Birring SS, Spinou A. How best to measure cough clinically. Curr Opin Pharmacol 2015; 22: 37‐40.
- Price DB, Buhl R, Chan A, et al. Fractional exhaled nitric oxide as a predictor of response to inhaled corticosteroids in patients with non‐specific respiratory symptoms and insignificant bronchodilator reversibility: a randomised controlled trial. Lancet Respir Med 2018; 6: 29‐39.
- Sadeghi MH, Wright CE, Hart S, et al. Phenotyping patients with chronic cough: evaluating the ability to predict the response to anti‐inflammatory therapy. Ann Allergy Asthma Immunol 2018; 120: 285‐291.
- Hodgson D, Anderson J, Reynolds C, et al. The effects of azithromycin in treatment‐resistant cough: a randomized, double‐blind, placebo‐controlled trial. Chest 2016; 149: 1052‐1060.
- Cohen SM, Misono S. Use of specific neuromodulators in the treatment of chronic, idiopathic cough: a systematic review. Otolaryngol Head Neck Surg 2013; 148: 374‐382.
- Wei W, Liu R, ZhangTong Y, Qiu Z. The efficacy of specific neuromodulators on human refractory chronic cough: a systematic review and meta‐analysis. J Thorac Dis 2016; 8: 2942‐2951.
- Morice AH, Menon MS, Mulrennan SA, et al. Opiate therapy in chronic cough. Am J Respir Crit Care Med 2007; 175: 312‐315.
Provenance: Not commissioned; externally peer reviewed.
Interpreting Australian Stillbirth Rate Trends: Implications for Surveillance and Continuous Quality Improvement
Aleena M. Wojcieszek, Kirstine Sketcher-Baker, Christine Andrews, Michael Coory, Imogen Kettle, Melissa Malivoire, David Ellwood, Vicki Flenady
Paracetamol in Pregnancy: Uncertain Evidence, Certain Consequences
David J. Tunnicliffe, Miranda Cumpston, Debra Kennedy, Margie Danchin, Armando Teixeira-Pinto
Fatty Liver Disease in Australia: A Narrative Review on the Epidemiology, Natural History, Prognostication and Management in People With Metabolic Dysfunction
Karl Vaz, Daniel Clayton-Chubb, William W. Kemp, Stuart K. Roberts, Ammar Majeed
Birth prevalence, clinical sequelae, and management of congenital cytomegalovirus infections in Australia, 1999–2023: a national prospective study
Ece Egilmezer, Suzy M Teutsch, Carlos Nunez, Stuart T Hamilton, Adam W Bartlett, Pamela Palasanthiran, Elizabeth J Elliott, William D Rawlinson
The number of cancer‐related deaths that could be attributable to spatial disparities in survival in Australia, 2010–2019: a retrospective population‐based cohort study
Charlotte K Bainomugisa, Jessica Cameron, Paramita Dasgupta, Peter Baade
Mandatory research projects during medical specialist training in Australia and New Zealand
Paulina Stehlik, Caitlin Brandenburg, David A Henry