





Research letter
Open access CC BY NC ND
Volume 218 - Issue 7
Different estimates of the prevalence of dementia in Australia, 2021
Authors: Annette J Dobson, Leon Flicker, Osvaldo P Almeida, Michael Waller and Kaarin Anstey
Med J Aust 2023 || doi: 10.5694/mja2.51838
Published online: 13 March 2023
Published online: 13 March 2023
The range of prevalence estimates suggests that re-assessing future demand may be appropriate
Estimates of the number of Australians living with dementia vary from fewer than 200000 to more than 450000. To understand these differences, we assessed the sources of the estimates. The 2021 Australian census, which collected data on the entire population (including people in hospitals and residential aged care), included a question on whether each person had been told by a doctor or nurse they had “dementia (including Alzheimer's)”.1 For the 2018–19 NPS MedicineWise national survey of general practice, data were extracted from the electronic records of a sample of 569 practices (7% of all general practices) that included 9% of general practitioners and 13% of people who had consulted GPs in Australia during the survey period.2 The Australian Institute of Health and Welfare (AIHW) derived its 2021 estimate3 from the 2015 Alzheimer's Disease International (ADI) report,4 an analysis of studies applying standardised diagnostic criteria in high income countries, most undertaken before 2000. The National Centre for Social and Economic Modelling (NATSEM) used standard demographic modelling to estimate the number of people in Australia living with dementia in 2022 for Dementia Australia5 (further details: Supporting Information).
We calculated age‐and sex‐specific prevalence rates for Australians aged 60 years or more in 2021 from the 2021 census,1 the 2018–19 NPS MedicineWise report,2 and the 2021 AIHW report,3 using estimated population numbers by sex and 5‐year age group for June 2021.6 Summary prevalence rates were estimated using direct sex and age standardisation based on the estimated 2021 Australian population. We did not seek ethics approval for our analysis of publicly available data.
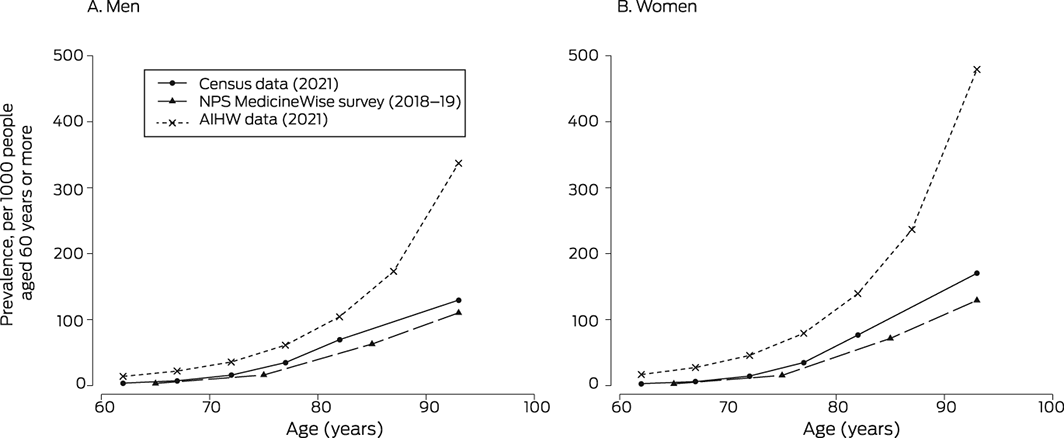
The estimated prevalence of dementia among people aged 60 years or more based on 2021 census1 or 2018–19 NPS MedicineWise data2 was lower for men and women of all ages than that based on 2021 AIHW data3 (Box). The estimated age‐ and sex‐standardised prevalence was 31.4 per 1000 people (2021 census), 21.4 per 1000 people (2018–19 NPS MedicineWise survey), and 65.9 per 1000 people (2021 AIHW data). The estimated number of people aged 60 years or more living with dementia were 181580 (2021 census), 123818 (2018–19 NPS MedicineWise), and 380768 (2021 AIHW). In 2022, NATSEM estimated that 487500 people (all ages) had dementia.5
All methods for estimating national dementia prevalence have strengths and weaknesses.7 One meta‐analysis found that about half of all people living with dementia are undiagnosed or their condition is unreported.8 Dementia can be underreported because of the time lag between initial symptoms and clinical diagnosis, infrequent contact with diagnostic services, and fear of stigmatisation. National and local health surveys often do not include clinical diagnosis information, have low response rates, and do not include people in residential care, where a large proportion of people have dementia.9 Community studies are similarly affected by low response rates and socio‐demographic biases, compounded by difficulties in recruiting and retaining participants.7 People from lower socio‐economic status or rural or remote areas, with multiple health conditions, or from culturally or linguistically diverse backgrounds may be underrepresented in data sources such as clinical registries.7 General practitioners are more likely to see people not included in community studies or clinical registries, particularly older people with chronic conditions, but they may not record dementia if cognitive impairment is not the main reason for a consultation. The population coverage of the Australian census is near complete, and the concordance of self‐reports and proxy measures of dementia with clinical diagnoses is reasonable.10
The lower estimates of dementia prevalence based on the 2021 census and the NPS MedicineWise survey are plausible. The age‐standardised dementia incidence among people aged 65 years or more estimated by the Sax Institute 45 and Up study (2020), based on linked survey and administrative health records data, was 27% lower than the global estimate for high income countries.11 Further, the prevalence in Australia of other conditions that share risk factors with dementia, such as cardiovascular diseases, have been falling for decades.12 As dementia incidence is also declining in some high income countries,13 older data may not be useful for estimating its more recent prevalence.
Information regarding dementia should continue to be collected in future censuses and its validity assessed. Planning services for people living with dementia is important because of our ageing population, but the range of prevalence estimates for 2021 suggests that re‐assessing future demand may be appropriate.
Competing interests
No relevant disclosures.
Received 20 October 2022, accepted 22 December 2022
Acknowledgements
This analysis was supported by the National Health and Medical Research Council Boosting Dementia Research Grant (APP1171319). We acknowledge the assistance of Paul McElwee (School of Public Health, University of Queensland) for coordinating the project; he also contributed to discussions and helped develop the final manuscript.
References
- Australian Bureau of Statistics. Census of Population and Housing: health data summary, 2021; table 1. 12 Oct 2022. https://www.abs.gov.au/statistics/health/health‐conditions‐and‐risks/health‐census/2021/Health%20data%20summary%20‐%20first%20and%20second%20release.xlsx (viewed Dec 2022).
- NPS MedicineWise. General practice insights report, July 2018 – June 2019. Sydney: NPS MedicineWise, 2020. www.nps.org.au/assets/Report‐2018‐19‐GPIR.pdf (viewed Dec 2022).
- Australian Institute of Health and Welfare. Dementia in Australia 2021: data (Cat. no. DEM 2). Updated 16 Sept 2022. https://www.aihw.gov.au/reports/dementia/dementia‐in‐aus/data (viewed Dec 2022).
- Alzheimer's Disease International. World Alzheimer report 2015. The global impact of dementia: an analysis of prevalence, incidence, cost and trends. 21 Sept 2015. www.alzint.org/resource/world‐alzheimer‐report‐2015 (viewed Dec 2022).
- Dementia Australia. Dementia prevalence data. 2022. www.dementia.org.au/information/statistics/prevalence‐data (viewed Oct 2022).
- Australian Bureau of Statistics. National, state and territory population. Reference period December 2021. 28 June 2022. www.abs.gov.au/statistics/people/population/national‐state‐and‐territory‐population/dec‐2021 (viewed Oct 2022).
- Flicker L, Anstey KJ, Almeida OP, et al. Differing methodologies are required to estimate prevalence of dementia: Single study types are no longer reliable. J Alzheimers Dis 2022; 88: 943‐948.
- Lang L, Clifford A, Wei L, et al. Prevalence and determinants of undetected dementia in the community: a systematic literature review and a meta‐analysis. BMJ Open 2017; 7: e011146.
- Gamble LD, Matthews FE, Jones IR, et al. Characteristics of people living with undiagnosed dementia: findings from the CFAS Wales study. BMC Geriatr 2022; 22: 409.
- Hendry K, Quinn TJ, Evans JJ, Stott DJ. Informant single screening questions for delirium and dementia in acute care: a cross‐sectional test accuracy pilot study. BMC Geriatr 2015; 15: 17.
- Welberry HJ, Brodaty H, Hsu B, et al. Measuring dementia incidence within a cohort of 267153 older Australians using routinely collected linked administrative data. Sci Rep 2020; 10: 8781.
- Australian Institute of Health and Welfare. Heart, stroke and vascular disease: Australian facts. 29 Sept 2021. www.aihw.gov.au/reports/heart‐stroke‐vascular‐diseases/hsvd‐facts/contents/heart‐stroke‐and‐vascular‐disease‐and‐subtypes/what‐is‐coronary‐heart‐disease (viewed Jan 2023).
- Stephan BCM, Birdi R, Tang EYH, et al. Secular trends in dementia prevalence and incidence worldwide: a systematic review. J Alzheimers Dis 2018; 66: 653‐680.