





Open access CC BY NC ND
Volume 217 - Issue 11
“Harry Potter and the Multitudinous Maladies”: a retrospective population‐based observational study of morbidity and mortality among witches and wizards
Authors: Vincent D Gaertner, Elia D Helwig, Brett J Manley, Omar F Kamlin, Andrea Kraus and Christoph M Rüegger
Med J Aust 2022; 217 (11): 592-597. || doi: 10.5694/mja2.51784
Published online: 12 December 2022
Published online: 12 December 2022
Magical remedies should be incorporated into Muggle medicine to improve patient outcomes and to reduce burdens on healthcare systems
Abstract
Objectives: To describe the prevalence of maladies and deaths among witches and wizards in the Harry Potter world, their causes, and associated therapies.
Design: Retrospective population‐based observational study (report analysis) undertaken 10 February – 19 March 2022.
Setting: All locations described in the Harry Potter books, predominantly Hogwarts School of Witchcraft and Wizardry, but also selected locations, including Privet Drive No 4, Diagon Alley, the Ministry of Magic, and The Burrow.
Participants: All witches and wizards mentioned at least once in any of the seven Harry Potter books.
Main outcome measures: Overall numbers of maladies and deaths. Secondary outcomes were changes in morbidity and mortality over time, causes of morbidity and mortality, and treatments.
Results: A total of 603 wizards or witches named in the Potter books experienced 1541 maladies and injuries (1410 non‐fatal) and 131 deaths. Overall morbidity incidence was 471 events per 1000 individuals, and mortality, after adjustment for Lord Voldemort's multi‐mortality, was 20.6%. The most frequent causes of morbidity were traumatic injuries during duels or fights (553 cases, 39.2%), magical objects, potions, plants, or creatures (345, 24.5%), and non‐combative trauma (221, 15.7%). Most deaths were related to wizarding duels (101 of 131, 77.1%). Treatments were rarely described; the most frequent were jinxes (274, 19.4%) and potions (136, 9.6%). Hospital stays were shorter than a week for almost all non‐fatal maladies (1397 of 1410, 99.1%).
Conclusions: Morbidity and, in particular, mortality were very high and predominantly caused by magical means. Further investigation into the safety at Hogwarts School of Witchcraft and Wizardry is warranted. The few treatments used had high success rates; rapid recovery was the rule, and hospital stays generally brief. Efforts should be undertaken to identify the magical therapies and interventions used and to introduce these novel remedies into Muggle medicine.
The known: The first Harry Potter report was published 25years ago, and the book series sparked overwhelming public interest. However, morbidity and mortality among wizards and witches has not been examined in the medical literature.
The new: Morbidity and mortality in the wizarding population were high, and the safety standards at the Hogwarts School of Witchcraft and Wizardry are clearly questionable. However, the few treatments used were highly effective, hospital stays were brief, and chronic illness was rare.
The implications: Magical remedies should be incorporated into Muggle medicine to improve patient outcomes and to reduce burdens on healthcare systems.
The first report on the world of wizards in the United Kingdom, published 25years ago this year, focused mainly on a young boy named Harry Potter, attending Hogwarts School of Witchcraft and Wizardry.1 Six further detailed accounts of the primary subject's life during his schooldays have since been published,2,3,4,5,6,7 sparking major interest in his world, with more than half a billion books sold and translations into 80 languages.8,9 Despite increasing evidence for the presence of wizards and witches, medical knowledge about this population is limited. While the original accounts of Harry Potter's life have sparked analogies for medical and educational purposes,10,11,12 no publication has focused on medical entities in this parallel wizarding world.
If the original account can be believed, wizards have the ability to hide from us “Muggles” (non‐magical people) using advanced spells (eg, Repello Muggletum),4,7 possibly explaining the lack of medical literature on wizards. Still, as physicians in the Muggle world may need to treat witches and wizards, understanding the epidemiological characteristics of magical maladies is important. Further, studying effective alternative treatment methods may be important, even for non‐magical populations.
The primary aim of our study was therefore to describe morbidity and mortality among witches and wizards across a seven‐year observational period corresponding with the school years of Harry Potter at Hogwarts. Secondly, we describe causes of morbidity and mortality, as well as the associated therapies.
Methods
We undertook a retrospective analysis of written accounts about a boy named Harry Potter, his peers, and the staff at the only known wizarding school in the United Kingdom, Hogwarts.1,2,3,4,5,6,7 As neither the subjects of the original reports nor their parents or guardians could be reached by reasonable (non‐magical) means, no written informed consent could be obtained. However, all reported patient data are publicly available in most libraries and households around the world. Similarly, de‐identification and maintaining confidentiality were neither possible nor desirable and the real names of all persons are used throughout our report. This improves readability and allows the passionate community of readers around the world to challenge our dataset. Our reporting follows the STROBE guideline.13
Data extraction and participants
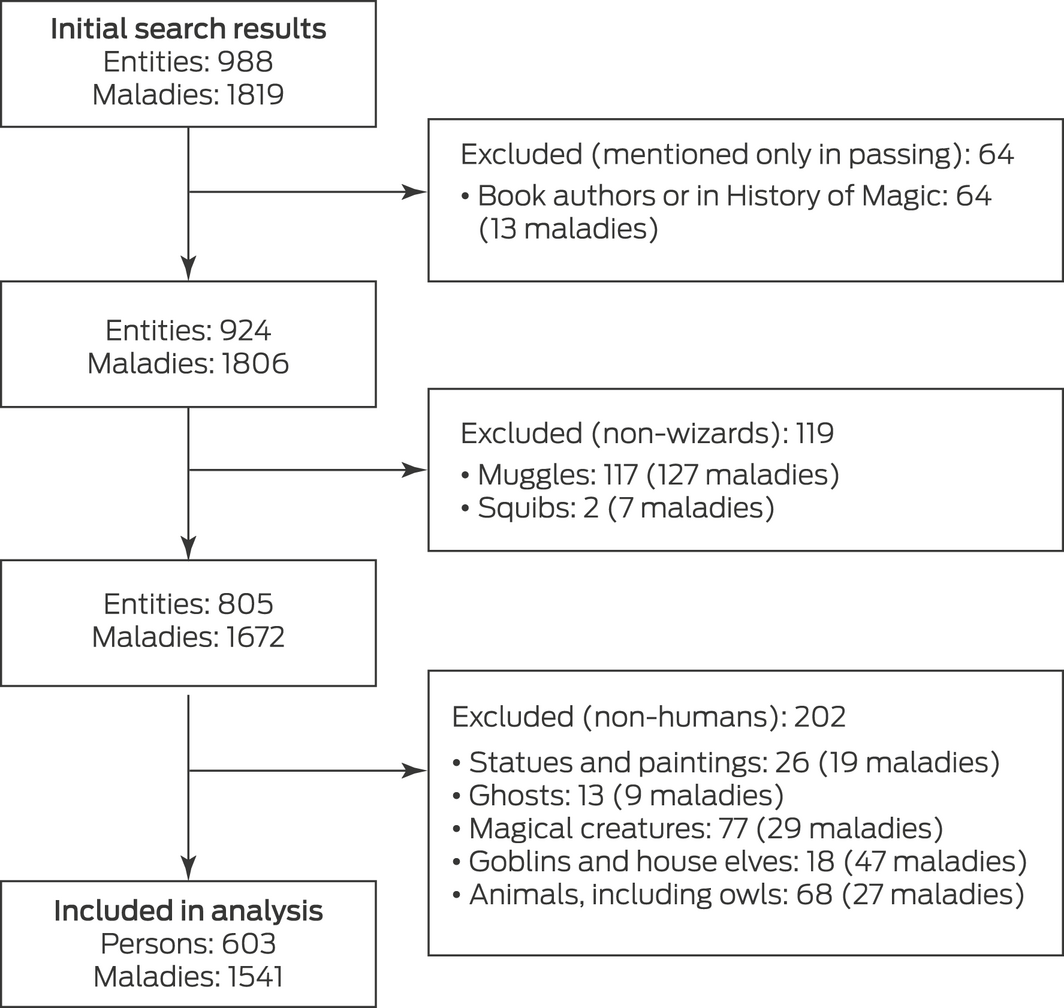
Two reviewers (VDG, EDH) read the first edition Harry Potter reports1,2,3,4,5,6,7 and independently extracted an exhaustive list of all persons and their maladies. We included only witches and wizards in our main analysis, excluding individuals mentioned only as book authors or in History of Magic lessons, as well as all Muggles, Squibs, statues, ghosts, creatures, animals, goblins, and paintings.
For each malady, we recorded the book and page number, description of the incident, and whether it was fatal, as well as the cause, perpetrator, treatment, and duration of hospitalisation. Causes of morbidity and mortality were categorised as “duels/fights” (magical and non‐magical), “magical objects, potions, plants, or creatures”, and “Weasley's Wizard Wheezes”, as well as “trauma”, “psychiatric”, and “other causes”. For mortality, “natural cause of death” was an additional category. Treatments were classified as “magical potions and plants”, “jinxes”, “untreatable”, or “no accurate information available”.
Outcomes
The primary outcome was overall morbidity and mortality in the wizarding world. Secondary outcomes were morbidity and mortality during the seven‐year observation period, as well as causes, risk factors, and treatments.
Patient and public involvement
General public interest in the Harry Potter book series is huge: various websites examine Harry Potter's adventures in detail (eg, harrypotter.fandom.com, wizardingworld.com) and more than half a billion books have been sold to date.8 We would have liked to include patients in the design, recruitment, conduct, and analysis of our study but we unfortunately had no access to magical means of contact, such as Apparition, Floo powder, brooms, or platform 9¾ at King's Cross Station. Finally, wizards and witches have the means to remain undetected by Muggles,5,7 possibly explaining our inability to track down patients. We acknowledge that investigators from within the wizarding world may have means to access these data upon the publication of our report and to disseminate their findings effectively.
Statistical analysis
Quantitative non‐parametric data are summarised as medians with interquartile ranges (IQRs), nominal data as numbers and proportions. As the Harry Potter reports are centred on one subject, the likelihood of selection or sampling bias is high;14 we consequently undertook no inferential statistical analyses. Analyses were performed using R 3.6.2 (R Foundation for Statistical Computing).
Ethics approval
We initially sought ethics approval for our study from J. K. Rowling, author of the original reports and Chair of the Witch and Wizard Research Ethics Committee of Hogwarts School of Witchcraft and Wizardry and the Department of Magical Education of the Ministry of Magic. However, time constraints meant our application could not be assessed, and formal approval could not be granted. However, J. K. Rowling's representatives, the Blair Partnership, provided a letter exempting the study from formal approval, allowing us to proceed with our project.
Results
Seven reports including a total of 3407 pages were read between 10 February and 19 March 2022. The dataset comprised data for 988 individuals, including 603 wizards and witches we included in our analysis (Box 1, Box 2; Supporting Information, file 1).
Overall morbidity and mortality
A total of 1541 maladies or deaths were identified (Supporting Information, file 2). Initial reviewer congruence was 96.2%, and all disagreements could be resolved by consensus. A total of 1410 maladies were non‐fatal, with a median of zero maladies per included individual (range, 0–429); the incidence of any malady was 471 cases per 1000 individuals (47.1%). In total, 131 deaths were recorded, but this included eight deaths for Tom Marvolo Riddle/Lord Voldemort, caused by the destruction of his Horcruxes: three by the Sword of Gryffindor, three (including his own body and that inside Harry's body) by jinxes, and two using a basilisk fang. After adjusting for this anomaly, the corrected mortality rate was 20.6%.
Morbidity and mortality over time
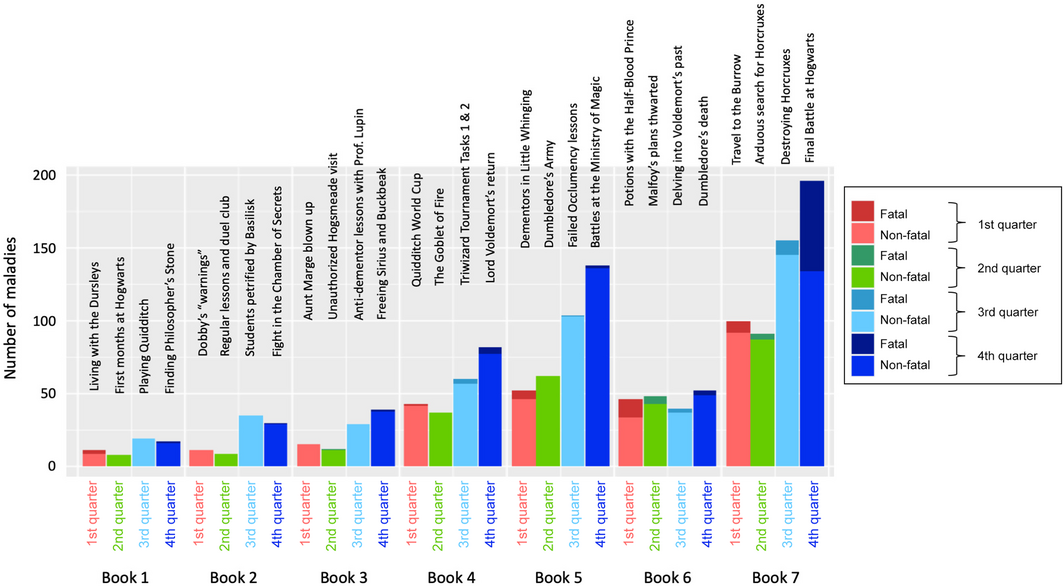
Morbidity increased continuously (with the exception of book 6) and markedly across the 7‐year period, as well as over the course of each school year for those working or attending Hogwarts; the incidence of malady and death were each highest at the end of each school year (Box 3). The increase over time remained after correction for the length of each published report (from 25 [year one] to 89 [year seven] maladies or deaths per 100 pages).
Causes of morbidity and mortality
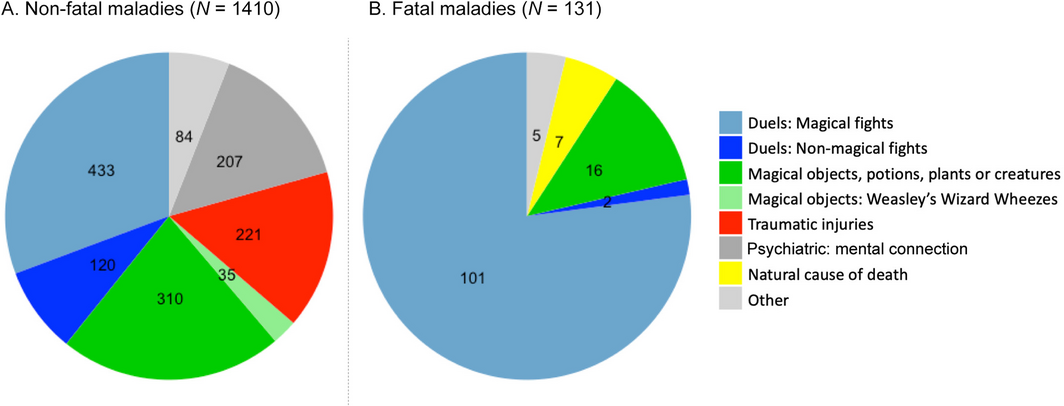
The most frequent causes of morbidity were traumatic injuries during duels and fights (magical or non‐magical; 553 of 1410, 39.2%), magical objects, potions, plants, or creatures (345, 24.5%), and non‐combative trauma (221, 15.7%). Most deaths were associated with wizarding duels (101 of 131, 77.1%); the most frequently reported used jinx was the Killing Curse, Avada Kedavra (29 of 31 reported incantations, 94%) (Box 4).
Treatments
For 980 of 1410 maladies (69.5%) no treatment was described; we presume they resolved spontaneously without therapy. The most frequent treatments were jinxes (274 of 1410, 19.4%) or potions (136, 9.6%). Only twenty of 1410 maladies (1.4%) were untreatable and described as chronic in nature. Almost all hospital stays were shorter than one week (1397 of 1410, 99.1%).
Discussion
In this first account of magical maladies, morbidity and, in particular, mortality at Hogwarts School of Witchcraft and Wizardry was very high and increased over time. Major causes of morbidity included duels and fights, magical objects, and traumatic injuries, while the major causes of mortality were magical jinxes. Treatment success rates were high, and hospitalisation durations short. This report increases understanding of magical maladies and identifies potential avenues for future treatments in the Muggle world.
Overall morbidity and mortality were alarmingly high in this selected wizarding population (mortality rate of 21%, morbidity almost 50%), despite the relatively low mean age. In 2010, 52.8 million Muggles died worldwide, a global mortality rate of 0.8%.15 There are several potential reasons for the higher rate in our study. First, the selected population may have been a high risk population, but, as the reports centre on adolescents in an elite United Kingdom boarding school, this seems unlikely. In two earlier reports from the Eton College sanatorium, a comparable Muggle institution, mortality was zero.16,17 Second, high mortality might be explained by specific events during data collection, reflected in chapter titles including words such as “war” or “battle”.5,6,7 The increase in morbidity and mortality across the observation period also corresponded with the increasingly sombre atmosphere of the books.1,2,3,4,5,6,7 However, risks in magical colleges may differ from Muggle schools: falling from a broom fifty feet in the air seems more dangerous than playing Muggle sports,17 and performing complex spells may be more dangerous than learning basic chemistry, particularly as jinxes can backfire on wizards (eg, when Ron Weasley started vomiting slugs).1 While overall morbidity was similar to the global incidence of Muggle morbidity,18 it was higher than in the elite Eton boarding school16 or in American emergency departments.19,20
Interestingly, causes of morbidity and mortality were quite different to the global burden of Muggle diseases. While traumatic injuries affect both populations, infections were rarely reported in the wizarding world, unlike the Muggle world.15,20 Instead, magical duels and other magical items (potions, plants, or bewitched objects, including Fainting Fancies and Puking Pastilles) are frequent causes of morbidity among wizards. While acute morbidity was high, almost all maladies resolved immediately and chronic illness was rare, again contrasting with the Muggle world.18 As duels and fights were the most frequent cause of morbidity and, more importantly, mortality, better supervision is urgently required at this school, and we call for the Ministry of Magic to investigate options for improving student safety at Hogwarts.
Possible reasons for the high morbidity and mortality include dangers associated with certain characters. Hogwarts gamekeeper and teacher Rubeus Hagrid, for example, has difficulties controlling his strength (giving rib‐cracking hugs, or inducing concussions by patting students’ backs) and loves dangerous creatures, including an Acromantula (Aragog) and a dragon (Norbert[a], the Norwegian ridgeback). However, none of his close friends died, suggesting that injuries inflicted by Hagrid or his beloved creatures were largely self‐limiting, and the risk may be outweighed by the friendship with a loving and caring half‐giant. However, the only known friends of Rubeus Hagrid are Harry Potter, Ron Weasley, Hermione Granger, Albus Dumbledore, and Olympe Maxime. The first three, key characters in the reports, sustained most of the injuries caused by Hagrid. As any statistical analyses would therefore have been subject to unresolvable confounding, we could not substantiate our assumption with valid, rigorously collected data.
Further, certain school subjects, including “Defence Against the Dark Arts”, “Herbology” — involving dangerous plants such as Devil's Snare, which almost suffocated Harry and Ron in year one, and Venomous Tentacula, particularly when they are teething1 — and “Care of Magical Creatures” — at least when Blast‐Ended Skrewts are being studied4 — may be associated with morbidity. “History of Magic”, on the other hand, seems safe, as no student was actually bored to death, with the possible exception of Professor Binns himself, whose body died one day, but his ghost returned to continue his teaching. However, improved learning experiences in more dangerous subjects need to be weighed against potentially increased danger. Prospective studies are required to tease out risk factors.
While morbidity was high, almost all maladies resolved very quickly. Magical treatments had an immediate effect; for example, the reduction of front teeth after the Densaugeo spell, Rennervate to revive people after the Stunning Spell, and Expecto Patronum for warding off Dementors. Some immediate remedies may also be useful in the Muggle world, such as the Pepper‐Up Potion that makes the drinker steam from the ears but offers immediate relief from upper respiratory infections.2 Such remedies may help overcome current challenges in Muggle medicine, such as the rise in antibiotic resistance.21 Unfortunately, no information on recipes could be obtained, and knowledge of jinxes among Muggle physicians is limited. Interestingly, few problems in the wizarding world needed longer term medication, such as the Wolfsbane Potion for relieving the symptoms of werewolfry.3 Chocolate was described as the most effective remedy after Dementor attacks,3 but its effectiveness in Muggle medicine has regrettably not been investigated in large prospective trials.
Muggle medication use and health care‐associated costs could be reduced by introducing treatments from the wizarding world. However, the choice and success of magical therapies seem to be highly dependent on the treating wizard or witch. For example, severe injuries (broken arms, noses, ankles, or a cracked skull, as well as injuries caused by dragon‐fighting or sustained hypothermia) could be mended “in no time” by Madam Pomfrey,1,2,4,5,6 but a non‐qualified wizard (Gilderoy Lockhart) made all the bones in Harry Potter's right arm vanish when he tried to mend them after a Quidditch accident.2 More effective regulation of the use of healing spells may therefore be needed.
Limitations
First, the longitudinal nature of our study made it difficult to disentangle time effects from age‐related effects. Second, we only included data from the original seven published accounts and neglected data from related reports (spin‐offs) about the same universe in literary and audio‐visual formats. Third, descriptions of all maladies were based on third‐person accounts. Ideally, we would have physically examined all affected persons or at least witnessed the events first‐hand; however, resource constraints precluded more detailed assessment, as the acquisition of devices such as Pensieves and Time‐Turners proved more difficult than expected.
Finally, and most importantly, we concede that data extracted from a literary account centred on a single individual are subject to severe sampling or selection bias.22 In a non‐randomly selected sample of participants, inferential data analysis is not robust and possibly misleading,16,22,23 which is why we restricted ourselves to descriptive statistics. As maladies in the Harry Potter accounts were more likely to be reported if sustained by one of Harry Potter's friends, it is not permissible to extrapolate our data to the entire wizarding population or to statistically compare our findings with data for the Muggle population. Nevertheless, our report provides a first account of maladies and deaths in the wizarding world, and insights into possible causes and therapies.
Conclusion
In this first account of magical maladies in the Harry Potter universe, morbidity and mortality were very high, and increased over time. Major causes of morbidity included duels and fights, magical objects, and traumatic injuries, while the major causes of mortality were magical curses. Treatment success rates were high. Our report contributes to understanding magical maladies and identifies potential avenues for novel treatments in the Muggle world.
Dissemination of our findings to relevant patient and public communities
We will disseminate this article widely across the wizarding world by contacting the Headmaster or Headmistress of Hogwarts School of Witchcraft and Wizardry, and the Department of Education and the Department of Health at the Ministry of Magic. However, we anticipate challenges, given the lack of contact addresses and phone numbers, unless we should come across alternative means of transportation (eg, brooms, Floo powder, Portkeys, or side‐along Apparition) or detect either of the two places by chance. We will also send our article to the author of the original account (J. K. Rowling) via her publishers, hoping she will contact and disseminate our findings in the wizarding world.
Data availability
The original data are available in bookstores, libraries, and even private households in most countries around the world in various languages. The detailed list of individuals and maladies extracted from the books is provided in the Supporting Information.
Box 2 – Baseline characteristics of the 603 wizards and witches we included in our analysis
|
Characteristics |
Number |
||||||||||||||
|
|
|||||||||||||||
|
Age group |
|
||||||||||||||
|
Adults |
426 (71%) |
||||||||||||||
|
Children |
177 (29%) |
||||||||||||||
|
Sex |
|
||||||||||||||
|
Male |
252 (42%) |
||||||||||||||
|
Female |
141 (23%) |
||||||||||||||
|
Unknown |
210 (35%) |
||||||||||||||
|
Hogwarts students (children only) |
153 (86%) |
||||||||||||||
|
Gryffindor |
42 [28%] |
||||||||||||||
|
Hufflepuff |
18 [12%] |
||||||||||||||
|
Ravenclaw |
19 [12%] |
||||||||||||||
|
Slytherin |
23 [15%] |
||||||||||||||
|
Unknown House |
51 [33%] |
||||||||||||||
|
Sports participation |
|
||||||||||||||
|
Confirmed Quidditch player |
57 (9.5%) |
||||||||||||||
|
|
|||||||||||||||
|
The complete dataset is included in the Supporting Information, file 1. |
|||||||||||||||
Competing interests
We declare that we are all fervent admirers of the Harry Potter reports. In a Sorting Hat quiz (https://www.potterquizzes.com/which‐harry‐potter‐house‐are‐you‐quiz), we were sorted into the following houses: Vincent Gaertner and Brett Manley (Gryffindor), Elia Helwig (Slytherin), Omar Kamlin (Ravenclaw), and Andrea Kraus and Christoph Rüegger (Hufflepuff). Vincent Gaertner declares that he thinks he may actually be a wizard and is still waiting for his invitation to attend Hogwarts School of Witchcraft and Wizardry. We have no other conflicts of interest to declare.
Acknowledgements
First and foremost, we thank J. K. Rowling for writing the primary account of life at the Hogwarts School of Witchcraft and Wizardry. Without her, it would not have been possible to extract all this information on diseases and maladies in the wizarding world. We also thank Sophie Gaertner for sparking the initial idea for this study.
References
- Rowling JK. Harry Potter and the philosopher's stone. London: Bloomsbury, 1997.
- Rowling JK. Harry Potter and the chamber of secrets. London: Bloomsbury, 1998.
- Rowling JK. Harry Potter and the prisoner of Azkaban. London: Bloomsbury, 1999.
- Rowling JK. Harry Potter and the goblet of fire. London: Bloomsbury, 2000.
- Rowling JK. Harry Potter and the Order of the Phoenix. London: Bloomsbury, 2003.
- Rowling JK. Harry Potter and the half‐blood prince. London: Bloomsbury, 2005.
- Rowling JK. Harry Potter and the Deathly Hallows. London: Bloomsbury, 2007.
- More than 500 Harry Potter books sold. Wizarding World, 1 Feb 2018. https://www.wizardingworld.com/news/500‐million‐harry‐potter‐books‐have‐now‐been‐sold‐worldwide (viewed June 2022).
- List of Harry Potter translations. Potterglot, undated. https://www.potterglot.net/the‐list (viewed June 2022).
- Baimas‐George M, Vrochides D. The sorting hat of medicine: why Hufflepuffs wear stethoscopes and Slytherins carry scalpels. J Surg Educ 2020; 77: 772‐778.
- Bryant V. Harry Potter and the osteopathic medical school: creating a Harry Potter‐themed day as a high‐yield review for final exams. Med Sci Educ 2021; 31: 819‐825.
- Gupta A. Harry Potter, magic, and medicine. JAMA Intern Med 2018; 178: 747‐748.
- Von Elm E, Altman DG, Egger M, et al; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Ann Intern Med 2007; 147: 573‐577.
- Warden G. Definitions of bias in clinical research. Methods Mol Biol 2021; 2249: 35‐52.
- Lozano R, Naghavi M, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012; 380: 2095‐2128.
- Briscoe JH. Sanatorium admissions in a boys’ boarding school. Public Health 1985; 99: 146‐153.
- Briscoe JH. Sports injuries in adolescent boarding school boys. Br J Sports Med 1985; 19: 67‐70.
- Global Burden of Disease Study 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018; 392: 1789‐1858.
- Rasooly IR, Mullins PM, Alpern ER, Pines JM. US emergency department use by children, 2001–2010. Pediatr Emerg Care 2014; 30: 602‐607.
- Pines JM, Zocchi MS, Black BS, et al; US Acute Care Solutions Research Group. Characterizing pediatric emergency department visits during the COVID‐19 pandemic. Am J Emerg Med 2021; 41: 201‐204.
- Frieri M, Kumar K, Boutin A. Antibiotic resistance. J Infect Public Health 2017; 10: 369‐378.
- Rothman KJ. Epidemiology: an introduction. New York: Oxford University Press, 2002.
- Nohr EA, Liew Z. How to investigate and adjust for selection bias in cohort studies. Acta Obstet Gynecol Scand 2018; 97: 407‐416.