





Volume 216 - Issue 2
Functional hypothalamic amenorrhoea: a diagnosis of exclusion
Authors: Elisabeth Ng, Shoshana Sztal‐Mazer and Susan R Davis
Med J Aust 2022; 216 (2): 73-76. || doi: 10.5694/mja2.51376
Published online: 7 February 2022
Published online: 7 February 2022
Functional hypothalamic amenorrhoea is common but often misdiagnosed, risking inappropriate management and compromised patient education and counselling
Functional hypothalamic amenorrhoea is common but often misdiagnosed, risking inappropriate management and compromised patient education and counselling
Secondary amenorrhoea before the age of 45 years, not due to pregnancy or lactation, lasting over 3 months in a previously eumenorrhoeic woman, or 6 months if menses have been irregular,1 is a cause for concern. Prolonged oestrogen deficiency due to amenorrhoea in reproductive aged women is associated with bone loss, increasing fracture susceptibility,2 dyslipidaemia3 and endothelial dysfunction, potentially increasing cardiovascular disease risk.4,5 Additionally, there is the psychological impact of anxiety about infertility and, conversely, possible unexpected ovulation and undesired pregnancy.6 Women with prolonged amenorrhoea experience more sexual dysfunction, depression and anxiety compared with women with eumenorrhoea.7 In this article, we summarise the available literature on the diagnosis and management of functional hypothalamic amenorrhoea (FHA). We searched PubMed, Google Scholar and the Cochrane Library for publications pertaining to the diagnosis and management of FHA from inception to June 2021. A hypothetical case study (Box 1) illustrates how the available literature can guide clinical practice.
The prevalence of secondary amenorrhoea remains uncertain. Frequent causes include FHA, polycystic ovary syndrome (PCOS), hyperprolactinaemia, premature ovarian insufficiency and early menopause (< 45 years of age). Less common aetiologies to consider and exclude include congenital adrenal hyperplasia, while rare causes include hypothalamic hypogonadism and androgen secreting tumours. Consequently, secondary amenorrhoea requires a thorough evaluation to identify the cause, as indicated in Box 2 and Box 3. Most importantly, a careful history that covers psychosocial and medical components, as described in Box 1, usually provides the key to the diagnosis.
FHA is chronic anovulation with no underlying anatomical or pathological cause, and is therefore a diagnosis of exclusion.2 PCOS, which affects an estimated 7–12% of premenopausal women, requires at least two of oligo/amenorrhoea, hyperandrogenism and sonographic evidence of polycystic ovaries for a diagnosis.8 Premature ovarian insufficiency is complete cessation of ovarian function before the age of 40 years,9 and has a reported prevalence of 4%.10 Premature ovarian insufficiency can be considered after at least 4 months of amenorrhoea with elevated follicle‐stimulating hormone (FSH) levels > 25 mIU/mL on two occasions at least 4 weeks apart.11 Although not required to make the diagnosis, low oestradiol levels characterise this condition. Hyperprolactinaemia, which may present as amenorrhoea with or without galactorrhoea, accounts for about 14% of secondary amenorrhoea in women aged 21–30 years.12 Importantly, hyperprolactinaemia may be secondary to a number of medications, notably antipsychotics and antidepressants,13 as well as clinical and subclinical hypothyroidism.14
FHA and PCOS are the two most common causes of hormonal subfertility and they can be difficult to differentiate when the classical clinical features of these two distinct conditions are absent. Such difficulty is encountered in lean women without pronounced hyperandrogenism, disturbed eating behaviour, weight loss or substantial exercise.15 While oestradiol levels are mostly low in FHA and in the normal range in PCOS, this is not always the case. Moreover, women with FHA often have multifollicular ovaries.16,17 Therefore, neither a high ovarian follicle count on ultrasound nor a high blood anti‐Müllerian hormone concentration can reliably differentiate PCOS from FHA.15,16 However, low sex hormone‐binding globulin is pathognomonic for PCOS,18 with a normal to high concentration indicating PCOS to be an unlikely diagnosis.18,19 Taken together, a pelvic ultrasound will not aid the diagnosis for normal weight or lean women with secondary amenorrhoea, who do not have biochemical or clinical hyperandrogenism. A progestogen challenge test can be used to induce a withdrawal bleed as evidence of oestrogen exposure, as occurs in women with PCOS, and no uterine outflow obstruction. As progestogens are often poorly tolerated and a bleed would be unexpected in women with chronically low oestradiol levels, this would not be diagnostically informative in our described patient (Box 1). The key differential will be establishing a psychosocial profile consistent with FHA.15
Hypothalamic amenorrhoea occurs as a result of disordered frequency and amplitude of hypothalamic gonadotrophin‐releasing hormone (GnRH) secretion, leading to loss of cyclical production of the gonadotrophins, FSH and luteinising hormone, and subsequent anovulation.20 For most women, however, serum FSH insufficiency is subtle, with levels remaining in the low normal range.17 Studies in humans have revealed that GnRH release is centrally controlled by a complex interplay between the neurotransmitters kisspeptin, neurokinin B and dynorphin released by KNDy neurons in the infundibular nucleus, and kisspeptin from the preoptic area, as shown in Box 4.21 Kisspeptin, which stimulates GnRH neurons in the hypothalamus, is inhibited by dynorphin and cortisol but stimulated by neurokinin B.22 Perturbations in this system can occur in response to physiological and/or psychological stress. Hence, mildly elevated 24‐hour mean cortisol levels are seen in women with FHA, which reflects a physiological response to stress.22 While we tend to characterise women with FHA as undertaking intense exercise, having a caloric deficit or marked weight loss, not all women with FHA will have an overt eating disorder or substantial recent weight loss.22 The aetiology is frequently subtle. Consequently, women with FHA can rarely identify a solitary stressor, as FHA often results from a synergistic combination of psychogenic and metabolic stressors, which can be seemingly minor.22 Thus, the hormonal changes that result in FHA can be precipitated by minimal stressors, such that FHA may develop without a clear history of exercise excess, disordered eating or significant weight loss, and may go undetected in weight stable, non‐exercising women.
The treatment of FHA involves explaining to the affected woman the role of psychological and metabolic stressors in hypothalamic–pituitary–adrenal axis disruption, and working with them to identify relevant modifiable behaviours.23 It is vital to reassure women with FHA that the condition is reversible and that fertility will be restored with resumption of menstrual cycles, or easily triggered with available interventions.2 Addressing FHA mostly requires a multidisciplinary team approach that may include expert medical, dietetic and psychological care. Psychological stressors should be sought and managed in all instances, with management of disordered eating and exercise excess where relevant.2 All women should receive a nutritional assessment, as nutritional deficiency may occur as a result of dietary preferences, such as vegetarianism or veganism (iron and zinc insufficiency), or dairy exclusion (calcium insufficiency). Cognitive behaviour therapy has been shown to lead to recovery of ovarian function, through addressing problematic behaviours and facilitating development of healthy coping mechanisms.24 Trauma therapy and other psychological support approaches should be offered where indicated.
Although FHA may be transient, it has been demonstrated to have lasting impacts, including low bone mineral density25 and an increased association with angiographic coronary artery disease.26 Bone mineral density and vitamin D levels should be measured in all women who have had 6 months of amenorrhoea, or less if nutritional depletion is likely to have preceded the amenorrhoea. As bone loss may commence after 6–12 months of amenorrhoea, hormone therapy in the form of oestrogen replacement with cyclic or continuous progestogen therapy should be commenced, to prevent bone loss if menstruation has not resumed within 6 months of appropriate intervention.
The US Endocrine Society guideline recommends against the use of a combined oral contraceptive pill to provide oestrogen replacement because, as intended, this inhibits ovulation and therefore masks recovery.2 Furthermore, oral oestrogen, whether as ethinyloestradiol or oestradiol, has not been found to improve bone mineral density in women with FHA.27 Conversely, transdermal oestradiol (100 µg 17‐β oestradiol) with cyclic progesterone has been shown to improve bone mineral density in adolescents with anorexia nervosa28 and in athletes aged 14–25 years with oligoamenorrhoea.29 Women with FHA often have disturbed cortisol and thyroid hormone production, which also affects their bone health.23,30 It is not known whether oral oestrogen further interferes with cortisol or thyroid hormone homeostasis through its effects on hepatic production of cortisol and thyroid‐binding globulins, thus impairing the efficacy of oral oestrogen on bone recovery.30 Therefore, specifically in the management of FHA, first line therapy should be with transdermal oestradiol (which does not undergo first pass hepatic metabolism) to optimise bone health,2,27 unless contraception is required, in which case an oestradiol‐containing combined oral contraceptive pill is preferred. A progestogen should be co‐prescribed to protect against endometrial hyperplasia and cancer. While body‐identical progesterone is the most physiological option and is preferred, many women will be limited to a synthetic progestin by cost. Although the goal is to achieve a transdermal oestradiol dose (with a patch or a gel) equivalent to a 100 µg/day oestradiol patch, treatment should be initiated at a lower dose to avoid side effects such as mastalgia and heavy bleeding, which many women with FHA may not tolerate. The US Endocrine Society recommends against the use of bisphosphonates for bone protection in FHA, as no studies have provided evidence for their use in this condition.2 Moreover, bisphosphates are stored in bone for many years and should therefore preferably not be used in women likely to subsequently become pregnant.2 Other antiresorptive agents have not been sufficiently studied in premenopausal women to justify their use.
In summary, FHA, although a common cause of secondary amenorrhoea, is a diagnosis of exclusion. Given the potential adverse physical health outcomes associated with secondary amenorrhoea due to any cause, combined with the psychological consequences of delayed diagnosis as well as misdiagnosis, it is important that women with secondary amenorrhoea are fully assessed when they first present. This should include assessment of bone health and cardiovascular health as part of the initial work‐up and management. A proactive approach to secondary amenorrhoea will enable a diagnosis to be made promptly and accurately, and expedite targeted treatment of the underlying cause.
Box 1 – Hypothetical case study
Karen (a fictional patient described for learning purposes and based on clinical experiences), a 27‐year‐old woman, presents with 16 months of amenorrhoea after ceasing the combined oral contraceptive pill. Karen underwent menarche at 12 years of age and had regular menses up until she commenced the combined oral contraceptive pill at 16 years of age for contraception. Although initially unconcerned, she is now worried that there is something wrong that might affect her future fertility, and while she is not presently in a relationship, she desires assessment and advice.
Karen is taking no other medication, is quite confident she is not pregnant, and gives a history of generally good health. She denies galactorrhoea, acne, management of excessive hair growth and vasomotor symptoms. She does not exercise in excess but does yoga and pilates. Her nutritional history is unremarkable. She works full‐time in marketing, lives in a shared house, drinks alcohol on weekends and does not smoke. She denies personal stress, anxiety and depression. On examination, her body mass index is 23.6 kg/m2 and no abnormalities are identified. Following the algorithm in Box 3, Karen’s pregnancy test result is negative (serum human chorionic gonadotropin level < 1 IU/L). Her thyroid‐stimulating hormone, prolactin and follicle‐stimulating hormone concentrations are normal — 0.66 mU/L (reference interval [RI], 0.5–5.0 mU/L), 212 mIU/L (RI, 90–630 mIU/L) and 6 IU/L (postmenopausal RI, > 25 IU/L), respectively — and she has a low serum oestradiol concentration (96 pmol/L; postmenopausal RI, < 200 pmol/L).
On reviewing Karen with her results, her history reconfirms that there has been no overt weight loss, eating disorder or mental illness. However, on re‐questioning, Karen shares that she has been feeling very “under the pump” at work, and is stressed about her work performance. She does not feel that she is anxious but she tends to worry about small things. This picture is consistent with functional hypothalamic amenorrhoea. Had biochemical investigations been indicative of a specific endocrine condition, further work‐up, as suggested by our algorithm (Box 3), would have been required.
Box 2 – A pragmatic assessment of a woman presenting with secondary amenorrhoea
History
- ▪ Exclude pregnancy, lactation, chronic and severe illness
- ▪ Current medications
- ► Hormonal contraception
- ► Drugs that cause hyperprolactinaemia
- ► Recreational drugs: cocaine and opioids
- ▪ Lifestyle
- ► Exercise habits
- ► Dietary pattern, caloric restriction
- ► Weight loss
- ► Stressors: work, study or personal
- ► Eating disorder or mental illness
- ▪ Hyperandrogenism: hirsutism, acne, alopecia
- ▪ Hyperprolactinaemia: galactorrhoea
- ▪ Ovarian insufficiency: hot flushes, vaginal dryness, poor sleep, prior chemotherapy or ovarian surgery
- ▪ Hypothalamic–pituitary disease: headaches, visual field changes, fatigue, symptoms of pituitary hormone deficit or excess
- ▪ Thyroid dysfunction: fatigue, weight or appetite change, bowel changes, weather intolerance
- ▪ Obstetric history: factors that may affect the endometrial lining; eg, surgical intervention, dilatation and curettage, endometritis or infection
- ▪ Family history: premature ovarian insufficiency, congenital adrenal hyperplasia, thyroid disease
- ▪ Past medical history including any chronic disease (past and present), autoimmune disease, infection (tuberculosis, syphilis)
- ▪ Height, weight, body mass index
- ▪ Urine pregnancy test
- ▪ Evaluate pubertal development and breast development
- ▪ Evidence of features of genetic conditions such as Turner syndrome: short stature, high arched palate, broad short neck, broad chest with widely spaced nipples, epicanthic fold
- ▪ Features of hyperandrogenism or virilisation: alopecia, breast atrophy, deep voice, increased muscle bulk, clitoromegaly
- ▪ Features of insulin resistance (polycystic ovary syndrome): acanthosis nigricans, skin tags
- ▪ Features of cortisol excess: proximal myopathy, striae, bruising, moon facies, buffalo hump, abdominal striae, central adiposity, thin skin, hypertension
- ▪ Breast and vulvovaginal examination: galactorrhoea, signs of oestrogen deficiency
- ▪ Signs of hyperthyroidism or hypothyroidism
- ▪ If concern of pituitary pathology: visual fields
Box 3 – Approach to the work‐up of secondary amenorrhoea
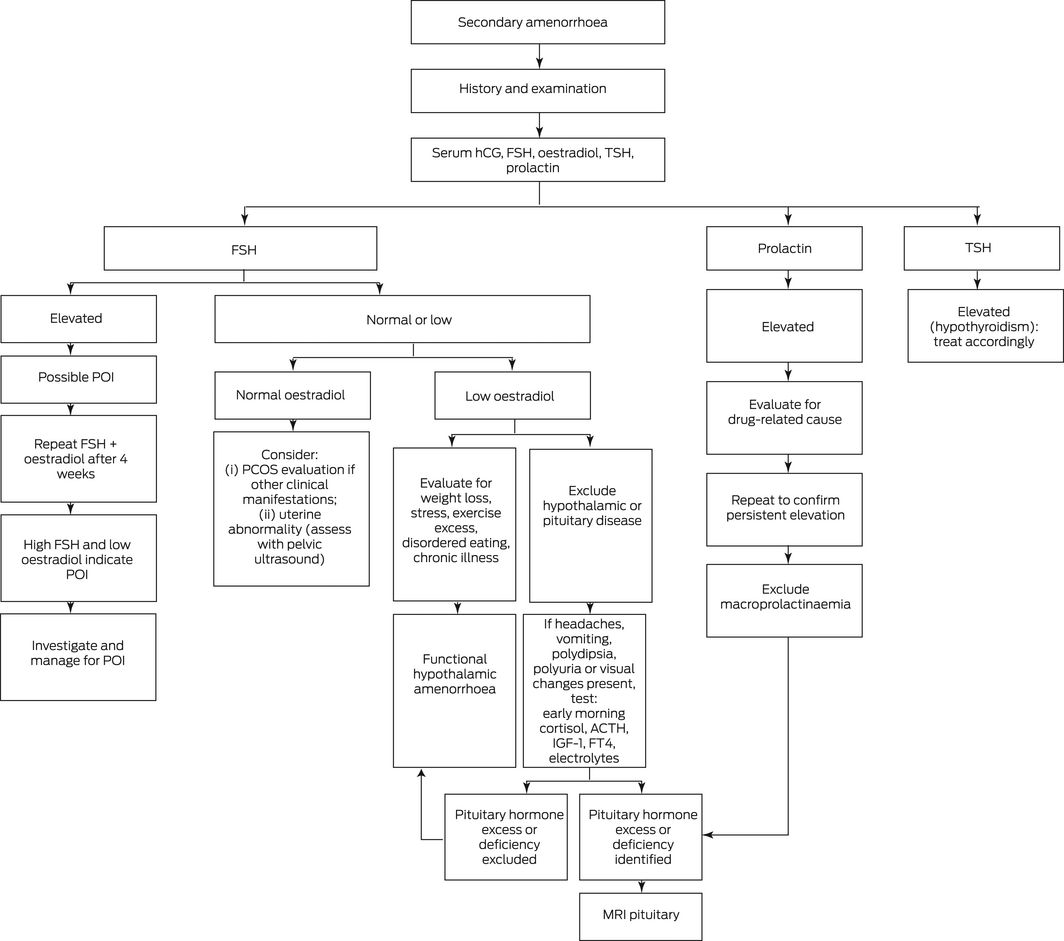
ACTH = adrenocorticotropic hormone; FSH = follicle‐stimulating hormone; FT4 = free thyroxine; hCG = human chorionic gonadotrophin; IGF‐1 = insulin‐like growth factor‐1; MRI = magnetic resonance imaging; PCOS = polycystic ovary syndrome; POI = premature ovarian insufficiency; TSH = thyroid‐stimulating hormone.
Box 4 – Central control of female reproduction
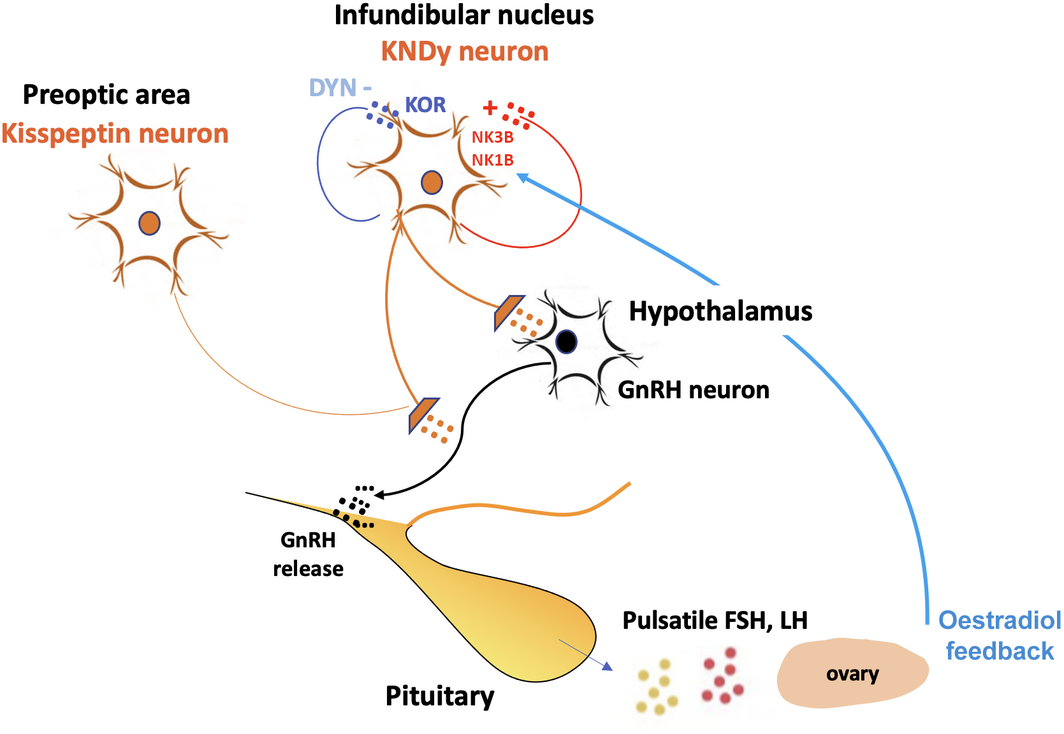
Kisspeptin, released from neurons in the preoptic area and infundibular nucleus, triggers gonadotrophin‐releasing hormone (GnRH) release. This is inhibited by dynorphin (DYN) via its receptor, the κ opioid receptor (KOR) and stimulated by neurokinin 3B (NK3B) and neurokinin 1B (NK1B) via receptors in the KNDy neuron complex. The pattern of kisspeptin release translates into the frequency and amplitude of GnRH pulses, which determine follicle‐stimulating hormone (FSH) and luteinising hormone (LH) release from the anterior pituitary gland.
Competing interests
Susan Davis has been paid for developing and delivering educational presentations for Besins Healthcare, BioFemme and Pfizer Australia; has been on advisory boards for Theramex, Abbott Laboratories, Astellas, Mayne Pharmaceuticals and Roche Diagnostics; has been a consultant to Lawley Pharmaceuticals, Southern Star Research and QUE Oncology; and has been an investigator for QUE Oncology and Ovoca Bio.
References
- Deligeoroglou E, Athanasopoulos N, Tsimaris P, et al. Evaluation and management of adolescent amenorrhea. Ann N Y Acad Sci 2010; 1205: 23–32.
- Gordon CM, Ackerman KE, Berga SL, et al. Functional hypothalamic amenorrhea: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 2017; 102: 1413–1439.
- Stevenson JC, Crook D, Godsland IF. Influence of age and menopause on serum lipids and lipoproteins in healthy women. Atherosclerosis 1993; 98: 83–90.
- Meczekalski B, Katulski K, Czyzyk A, et al. Functional hypothalamic amenorrhea and its influence on women’s health. J Endocrinol Invest 2014; 37: 1049–1056.
- Shuster LT, Rhodes DJ, Gostout BS, et al. Premature menopause or early menopause: long‐term health consequences. Maturitas 2010; 65: 161–166.
- Alper MM, Jolly EE, Garner PR. Pregnancies after premature ovarian failure. Obstet Gynecol 1986; 67(3 Suppl): 59S–62S.
- Dundon CM, Rellini AH, Tonani S, et al. Mood disorders and sexual functioning in women with functional hypothalamic amenorrhea. Fertil Steril 2010; 94: 2239–2243.
- Skiba MA, Islam RM, Bell RJ, Davis SR. Understanding variation in prevalence estimates of polycystic ovary syndrome: a systematic review and meta‐analysis. Hum Reprod Update 2018; 24: 694–709.
- Kovanci E, Schutt AK. Premature ovarian failure: clinical presentation and treatment. Obstet Gynecol Clin North Am 2015; 42: 153–161.
- Golezar S, Ramezani Tehrani F, et al. The global prevalence of primary ovarian insufficiency and early menopause: a meta‐analysis. Climacteric 2019; 22: 403–411.
- Webber L, Davies M, Anderson R, et al; European Society for Human Reproduction and Embryology (ESHRE) Guideline Group on POI. ESHRE guideline: management of women with premature ovarian insufficiency. Hum Reprod 2016; 31: 926–937.
- Lee DY, Oh YK, Yoon BK, Choi D. Prevalence of hyperprolactinemia in adolescents and young women with menstruation‐related problems. Am J Obstet Gynecol 2012; 206(213): e1–5.
- Samperi I, Lithgow K, Karavitaki N. Hyperprolactinaemia. J Clin Med 2019; 8: 2203.
- Sharma LK, Sharma N, Gadpayle AK, Dutta D. Prevalence and predictors of hyperprolactinemia in subclinical hypothyroidism. Eur J Intern Med 2016; 35: 106–110.
- Bradbury RA, Lee P, Smith HC. Elevated anti‐Mullerian hormone in lean women may not indicate polycystic ovarian syndrome. Aust N Z J Obstet Gynaecol 2017; 57: 552–557.
- Futterweit W, Yeh HC, Mechanick JI. Ultrasonographic study of ovaries of 19 women with weight loss‐related hypothalamic oligo‐amenorrhea. Biomed Pharmacother 1988; 42: 279–283.
- Jonard S, Pigny P, Jacquesson L, et al. The ovarian markers of the FSH insufficiency in functional hypothalamic amenorrhoea. Hum Reprod 2005; 20: 101–107.
- Deswal R, Yadav A, Dang AS. Sex hormone binding globulin — an important biomarker for predicting PCOS risk: a systematic review and meta‐analysis. Syst Biol Reprod Med 2018; 64: 12–24.
- Qu X, Donnelly R. Sex hormone‐binding globulin (SHBG) as an early biomarker and therapeutic target in polycystic ovary syndrome. Int J Mol Sci 2020; 21: 8191.
- Roberts RE, Farahani L, Webber L, Jayasena C. Current understanding of hypothalamic amenorrhoea. Ther Adv Endocrinol Metab 2020; 11: 2042018820945854.
- Skorupskaite K, George JT, Anderson RA. The kisspeptin‐GnRH pathway in human reproductive health and disease. Hum Reprod Update 2014; 20: 485–500.
- Morrison AE, Fleming S, Levy MJ. A review of the pathophysiology of functional hypothalamic amenorrhoea in women subject to psychological stress, disordered eating, excessive exercise or a combination of these factors. Clin Endocrinol (Oxf) 2021; 95: 229–238.
- Ruiz‐Zambrana A, Berga SL. A Clinician’s guide to functional hypothalamic amenorrhea. Clin Obstet Gynecol 2020; 63: 706–719.
- Berga SL, Loucks TL. Use of cognitive behavior therapy for functional hypothalamic amenorrhea. Ann N Y Acad 2006; 1092: 114–129.
- Nose‐Ogura S, Yoshino O, Dohi M, et al. Low bone mineral density in elite female athletes with a history of secondary amenorrhea in their teens. Clin J Sport Med 2020; 30: 245–250.
- Kaplan JR, Manuck SB. Ovarian dysfunction and the premenopausal origins of coronary heart disease. Menopause 2008; 15: 768–776.
- Aalberg K, Stavem K, Norheim F, et al. Effect of oral and transdermal oestrogen therapy on bone mineral density in functional hypothalamic amenorrhoea: a systematic review and meta‐analysis. BMJ Open Sport Exerc Med 2021; 7: e001112.
- Misra M, Katzman D, Miller KK, et al. Physiologic estrogen replacement increases bone density in adolescent girls with anorexia nervosa. J Bone Miner Res 2011; 26: 2430–2438.
- Ackerman KE, Singhal V, Slattery M, et al. Effects of estrogen replacement on bone geometry and microarchitecture in adolescent and young adult oligoamenorrheic athletes: a randomized trial. J Bone Miner Res 2020; 35: 248–260.
- Altayar O, Al Nofal A, Carranza Leon BG, et al. Treatments to prevent bone loss in functional hypothalamic amenorrhea: a systematic review and meta‐analysis. J Endocr Soc 2017; 1: 500–511.
Provenance: Not commissioned; externally peer reviewed.