





Volume 216 - Issue 10
The decline of invasive meningococcal disease and influenza in the time of COVID‐19: the silver linings of the pandemic playbook
Authors: CR Robert George, Robert Booy, Michael D Nissen and Monica M Lahra
Med J Aust 2022; 216 (10): 504-507. || doi: 10.5694/mja2.51463
Published online: 28 March 2022
Published online: 28 March 2022
A combination of targeted vaccinations and COVID-19 public health measures has led to reduced rates of invasive meningococcal disease and influenza
A combination of targeted vaccinations and COVID‐19 public health measures has led to reduced rates of invasive meningococcal disease and influenza
Both influenza and invasive meningococcal disease (IMD) are recognised as diseases of crowding,1 a factor also identified as central to coronavirus disease 2019 (COVID‐19) transmission.2 Observations from military outbreaks published more than 100 years ago illustrate the impact of overcrowding on both meningococcal carriage and invasive disease, and the effects of simple public health strategies to improve hygiene that had substantive impact on both disease rates and mortality.3 In that landmark paper from 1918, six predisposing factors for IMD were observed: season, severe weather, antecedent epidemics of influenza, temporarily lowered resistance, overcrowding, and high carriage rates. This has held true for a century; and moreover, recent work from the United Kingdom correlates reductions in carriage‐promoting social behaviours with a reduction in IMD incidence, suggesting that public health policies aimed at influencing behaviour might further reduce this disease.4 These observations resonate in 2022 as we reflect on the impact of broad scale public health measures taken during the COVID‐19 pandemic.
Influenza and invasive meningococcal disease
In recent times, the interplay between IMD and influenza has become increasingly understood.5 This correlation was demonstrated in a multi‐country analysis of the coincident seasonality of both infections, and supported by evidence that surges in influenza infections were followed by acute increases in IMD incidence.6,7 Both infections are spread between humans in proximity. The nasopharyngeal epithelial injury associated with influenza infection secondary to neuraminidase or immune dysfunction may permit colonist Neisseria meningitidis to invade and cause disease.8
In a study of IMD and influenza peaks in the United States between 1989 and 2009, correlation was identified in 19 of 20 seasons, with influenza H3N2 and H1N1 peaks being highly synchronised while pandemic influenza H1N1, influenza B and respiratory syncytial virus peaks were not.5 Notably, spikes in case numbers of seasonal influenza are typically reported in winter, as are cases of IMD. The correlation of disease spikes in Australia of confirmed cases of these diseases is pronounced, with 33 of 36 statistically detectable IMD case count spikes at 6 standard deviations concordant with independently detected spike periods for influenza between 2006 and 2021 (Box 1).
In Australia, both IMD and influenza are notifiable to government under legislation, and in 2020 and 2021, coincident with the global COVID‐19 pandemic, both IMD and influenza case numbers were the lowest since records began. We posit that this reduction in case numbers can be attributed to the series of intersecting public health policies and practices, including COVID‐19 prevention. The corollary of these interventions was the substantial reduction in notifications of other transmissible diseases, including pertussis and invasive pneumococcal disease.9 Further, IMD and influenza vaccination programs that have been systematically rolled out across Australia have also been influential in disease control (Box 2).
COVID‐19 pandemic public health measures and their impact on IMD and influenza
Broad‐ranging public health policies were introduced in Australia in response to the emergence of COVID‐19. These aimed to limit the spread of the disease by improved hygiene and physical distancing. Policies that limited crowding, including education about and enforcement of personal and social distancing measures, limitations on gathering sizes, and school closures, were enacted to prevent person‐to‐person transmission. Additional state‐level border closures, and local‐level lockdowns relating to hotspots likely further hindered the movement of pathogens. International travel restrictions limited the importation of infections from overseas.
Given the pathophysiological association between influenza and N. meningitidis, it is perhaps not entirely unexpected that the implementation of COVID‐19 restrictions has had a muting effect on IMD cases. Before restrictions were implemented in Australia in March 2020, there were 12 cases of IMD reported in January 2020, 13 cases in February 2020, then six cases in March 2020.9 Following restrictions, there were on average < 7 cases per month for the remainder of 2020.9 For the corresponding first quarter period for 2021 (January to March), after the introduction of restrictions, the reported IMD case numbers were substantially lower than for the corresponding period in 2020, with 18 cases recorded.9 During years when spikes in influenza have been seen, IMD case numbers have been considerably higher.
The impact of COVID‐19 public health policies on influenza has been previously documented in Australia and overseas.10 The number of laboratory‐confirmed influenza notifications from Australia in 2020 was 21 354,9 and 748 in 2021 (personal communication, National Notifiable Diseases Surveillance System, Australian Government Department of Health), substantially less than the 313 465 cases detected in 2019.9 In 2020, the vast majority (94%; 20 061/21 354) of influenza cases were reported from January to March, before the broad public health strategies and policies were implemented against COVID‐19. Of note, rates of other viruses transmitted via the respiratory route also decreased, including measles, varicella and rubella.11
Impact of vaccination practices and policies in Australia on IMD rates
Since 2003, progressive vaccine rollouts in Australia have influenced IMD rates. Vaccination programs targeting meningococcal serogroups and also those targeting influenza are relevant to IMD case reduction. Regarding meningococcal vaccination, several formulations are available in Australia, providing coverage against serogroups A (quadrivalent), B (recombinant), C (monovalent, quadrivalent, combination), W (quadrivalent) and Y (quadrivalent). The availability and funded delivery of the different vaccine classes has broadened over the past two decades, and has influenced the characteristics of seasonal meningococcal spikes.
Meningococcal serogroup C vaccination has demonstrably reduced national IMD rates,12 with a National Immunisation Program (NIP) funded monovalent vaccine available since 2003. The effect has been considerable, with IMD notifications falling from a peak 3.5 cases per 100 000 population (in 2001 and 2002) to 0.8 cases per 100 000 in 2019, before the COVID‐19 pandemic.9 Since 2018, the change from monovalent serogroup C to serogroup A, C, W and Y vaccination expanded coverage on the NIP for infants and then adolescents.13 This change followed initial jurisdictional level responses to serogroup W outbreaks and an increase in serogroup Y disease from 2017.12
Meningococcal serogroup B vaccination has been registered for individuals aged 2 months and over since August 2013. From October 2018, it was funded for eligible children including those residing in South Australia, where serogroup B disease rates are high, and then to Aboriginal and Torres Strait Islander infants nationally via the NIP on 1 July 2020. As such, only a very small proportion of the population is vaccinated, and impact is small.
Seasonal influenza vaccination in Australia has been progressively expanded over the past several decades in terms of funded coverage as well as strain coverage. Annual influenza vaccination has been offered under the NIP since 1997,14 and is currently recommended to all people aged 6 months and older.13 Presently, seven quadrivalent influenza vaccines are registered for use, containing two influenza A and two influenza B viral strains.15 Influenza vaccination reduces the frequency and severity of influenza infection, and it seems feasible that it would also reduce the likelihood of an individual developing IMD.
Implications for policy and practice in Australia and globally
The constellation of practices and policies in Australia targeting IMD and influenza over the past two decades, culminating in the extensive COVID‐19 public health measures commencing in 2020, coincided in the lowest rates of IMD and influenza since national records were kept. This outcome has likely manifested through a range of mechanisms. Several key public health lessons pertaining to these policies and practices have been learnt.
The first lessons relate to changes in IMD vaccination policy and seasonal influenza vaccination uptake. Expanded meningococcal vaccination coverage nationally has correlated with progressive reductions in serogroup‐specific IMD. Ongoing efforts are required to continue targeting serogroups that prevail, notably serogroup B. Moreover, in recognising the clear correlation between influenza and IMD spikes, measures that prevent influenza, including seasonal influenza vaccination, may play an important role in IMD case mitigation in the future.
Additional lessons relate to the impact of public health measures targeting COVID‐19 that have had wider benefits in terms of reduction of transmissible diseases. The broad‐scale public education strategies aimed at disrupting transmission dynamics, including restricting travel, improving hand hygiene practices, physical distancing, improving ventilation of indoor spaces, and mask wearing, have directly or indirectly influenced case numbers. There is little doubt that general awareness of infection control principles and practices has been raised in the population. This reinforces recent findings that changing social behaviours might further reduce rates of IMD, and is consistent with the historic findings from controlled defence settings,3 but also demonstrates that reductions in case numbers can be achieved in a broader social context and on a far greater scale.
Lessons are still being learnt with regard to the impact of COVID‐19 itself on IMD. However, based on data available to date, there appears to be little firm evidence suggesting that COVID‐19 itself is associated with IMD, given the decline in IMD cases seen during the COVID‐19 pandemic period, and particularly during the surge of cases seen with SARS‐CoV‐2 variant of concern Omicron.
Moving forward, while the combination of factors that have driven IMD and influenza in Australia to their lowest levels on record in 2020 and 2021 may not continue to conspire, the public health lessons will hopefully not be forgotten.
Box 1 – Correlation of spike periods for invasive meningococcal disease (IMD) and influenza in Australia
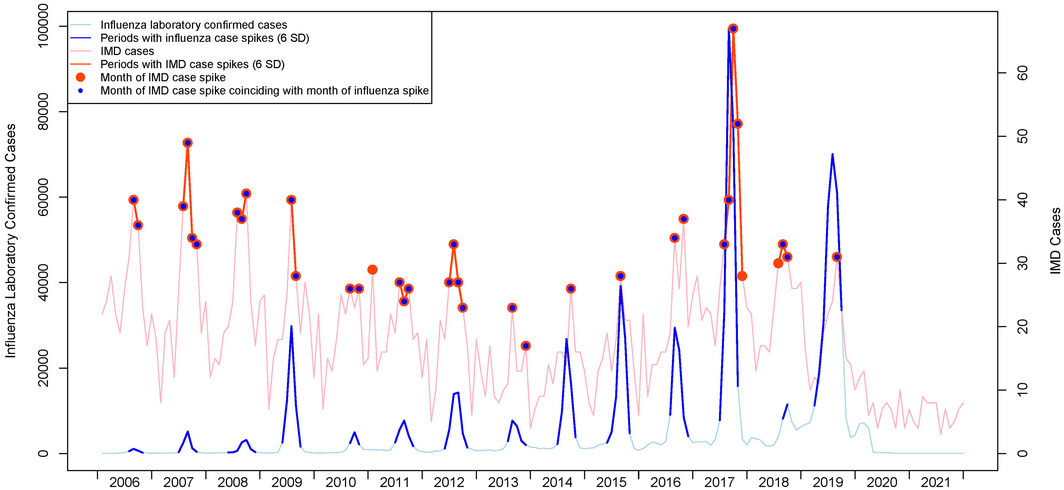
Source: National Notifiable Diseases Surveillance System. SD = standard deviation.
Box 2 – Vaccination interventions targeting invasive meningococcal disease (IMD) in Australia and circulating serogroups
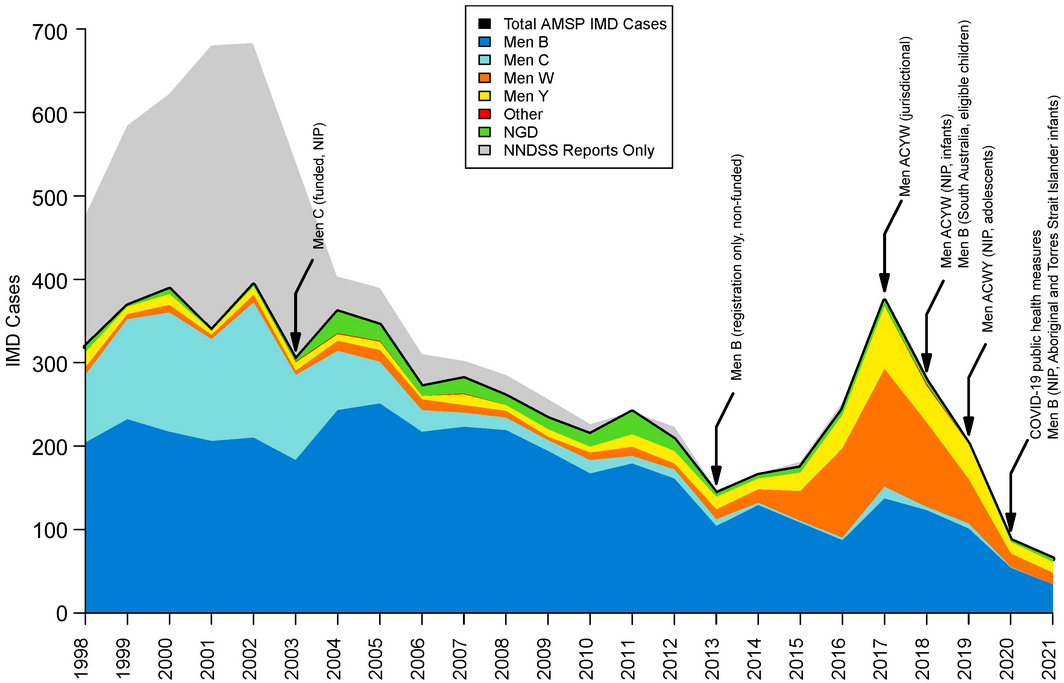
Sources: Australian Meningococcal Surveillance Programme and National Notifiable Diseases Surveillance System. AMSP = Australian Meningococcal Surveillance Programme; Men B = meningococcal serogroup B; Men C = meningococcal serogroup C; Men W = meningococcal serogroup W; Men Y = meningococcal serogroup Y; NIP = National Immunisation Program; NNDSS = National Notifiable Diseases Surveillance System; NGD = Not groupable or determinable.
Competing interests
Robert Booy consults to all vaccine companies supplying the Australian market. Michael Nissen is Principal Medical Officer, Australian Government Department of Health.
Acknowledgements
The Australian Government Department of Health funds the Australian Meningococcal Surveillance Programme.
References
- Booy R, El Bashir H, Rashid H, et al. Influenza and meningococcal disease: lessons for travellers and government from 2 epidemic diseases. Travel Med Infect Dis 2009; 7: 253‐256.
- Rader B, Scarpino SV, Nande A, et al. Crowding and the shape of COVID‐19 epidemics. Nat Med 2020; 26: 1829‐1834.
- Glover JA. “Spacing out” in the prevention of military epidemics of cerebro‐spinal fever. Br Med J 1918; 2: 509‐512.
- MacLennan JM, Rodrigues CMC, Bratcher HB, et al. Meningococcal carriage in periods of high and low invasive meningococcal disease incidence in the UK: comparison of UKMenCar1‐4 cross‐sectional survey results. Lancet Infect Dis 2021; 21: 677‐687.
- Jacobs JH, Viboud C, Tchetgen ET, et al. The association of meningococcal disease with influenza in the United States, 1989‐2009. PLoS One 2014; 9: e107486.
- Hubert B, Watier L, Garnerin P, Richardson S. Meningococcal disease and influenza‐like syndrome: a new approach to an old question. J Infect Dis 1992; 166: 542‐545.
- Cartwright KA, Jones DM, Smith AJ, et al. Influenza A and meningococcal disease. Lancet 1991; 338: 554‐557.
- Salomon A, Berry I, Tuite AR, et al. Influenza increases invasive meningococcal disease risk in temperate countries. Clin Microbiol Infect 2020; 26: 1257.e1‐e7.
- Australian Government Department of Health. National Notifiable Diseases Surveillance System. http://www9.health.gov.au/cda/source/cda‐index.cfm (viewed July 2021).
- Olsen SJ, Azziz‐Baumgartner E, Budd AP, et al. Decreased influenza activity during the COVID‐19 pandemic‐United States, Australia, Chile, and South Africa, 2020. Am J Transplant 2020; 20: 3681‐3685.
- Bright A, Glynn‐Robinson AJ, Kane S, et al. The effect of COVID‐19 public health measures on nationally notifiable diseases in Australia: preliminary analysis. Commun Dis Intell (2018) 2020; 44; https://doi.org/10.33321/cdi.2020.44.85.
- Lahra MM, Hogan TR, National Neisseria Network, Australia. Australian Meningococcal Surveillance Programme annual report, 2019. Commun Dis Intell (2018) 2020; 44; https://doi.org/10.33321/cdi.2020.44.62.
- Australian Technical Advisory Group on Immunisation. Australian immunisation handbook. Canberra: Australian Government Department of Health, 2018.
- National Centre for Immunisation Research and Surveillance. Adult vaccination. Vaccines for Australian adults: information for immunisation providers. Canberra: NCIRS, 2017.
- Therapeutic Goods Administration. 2021 seasonal influenza vaccines: information for consumers and health professionals. 13 April 2021. https://www.tga.gov.au/alert/2021‐seasonal‐influenza‐vaccines (viewed July 2021).
Linked content
-
MJA Podcast: Dr Robert George and Professor Monica Lahra
-
InSight+: Red flag for GPs: look out for meningococcal disease
Provenance: Not commissioned; externally peer reviewed.
Hospital-Admitted Injection-Related Infections Among Incarcerated People Who Inject Drugs in Australia: A Retrospective Cohort Study
Andrew Palmer, Matthew Carter, Jeremy Yeo, Cecilia Shim, Jason Connor, Jeremy Hayllar, Gerald Holtmann, Naomi Moy, Elliott G. Playford, Naomi Runnegar, Paul J. Clark
The Live Attenuated Influenza Vaccine in Australia: An Additional Tool for Influenza Prevention
Cyra Patel, Alexis Pillsbury, Tran Nguyen, Xia Wang, Helen E. Quinn, Clayton K. Chiu, Allen C. Cheng, Katie L. Flanagan, Zhicheng Wang
Reflex Testing for Hepatitis D Infection: A Unique Opportunity to Reduce Hepatitis D-Related Chronic Liver Disease Deaths in Australia
Jessica Howell, Lauren Andersson, Miriam T. Levy, James O'Beirne, Leon Adams, Katharine Irvine, Avik Majumdar, Golo Ahlenstiel, Kathy Jackson, Krispin Hajkowicz, Joseph Doyle, Jane Davies, Sarah Cherian, Wayne Dimech, Alexander J. Thompson
Localised Herpes Simplex Following Midline Laparotomy
Jessica S. Bulluss, Paul Chee, Matthew J. Verheyden
West Nile virus Kunjin subtype in rural NSW
Emily Gibson, Megan Whitley, Peter Murray, Linda Hueston, Jane Bennett, Raguharan Kathiresu, David N Durrheim
Differentiated and simplified oral HIV pre‐exposure prophylaxis (PrEP) models hold the key to virtually eliminating HIV transmission in Australia by 2030
Tyson Arapali, Sarah Warzywoda, Anthony K J Smith, Curtis Chan, Timothy R Broady, Erin Sullivan, Catherine MacPhail, Mohamed A Hammoud, Alexander Dowell‐Day, Benjamin R Bavinton