





Chronic traumatic encephalopathy (CTE) is a neurodegenerative tauopathy caused by repetitive head injury.1 Although it has chiefly been studied in contact sport participants, anyone who experiences repetitive head injury is at risk of CTE. It is associated with a range of neuro‐psychological problems, ranging from mood and behavioural symptoms to cognitive impairment and dementia.2 Clinical diagnostic criteria have been proposed,3 but, as for many neurodegenerative disorders, a definitive diagnosis requires post mortem brain examination.
In 2018, we established the Australian Sports Brain Bank (ASBB; https://www.brainbank.org.au) to support the study of CTE in Australia. The ASBB has since received more than 600 donation pledges from amateur and professional sportspeople. In this article we report preliminary findings based on the first 21 completed donations (to 26 March 2021). The study was approved by the Sydney Local Health District Ethics Review Committee (Royal Prince Alfred Hospital) (reference, X19‐0010).
All 21 donors had participated in sports with risks of repetitive head injury, including 17 who had played in football codes; we have previously described one case in detail.4 All but one donor exhibited some form of neurodegeneration, and 13 presented two or more neurodegenerative pathologies. The most frequent neuropathology was CTE: 12 donors had pathognomonic CTE lesions (Box 1).
The proportion of professional participants was higher in the CTE group (67% v 50%; P = 0.20). CTE was identified in the brains of older former professionals with long playing careers, but also in younger, non‐professional sportsmen and in recent professionals who had played under modern concussion guidelines. The mean age at death of the donors with CTE (48 years; standard deviation [SD], 19 years) was lower than for those without CTE (75 years; SD, 19 years), but mean duration of sport participation was similar for the two groups (Box 2). Three donors with CTE were under 35 years of age. The mean age at death of the six donors with CTE only (39 years; SD, 13 years) was lower than for the six with CTE and other neurodegenerative pathology (69 years; SD, 21 years).
Six of the 12 donors with CTE and one of nine without CTE had died by suicide (P = 0.042), suggesting CTE may be a suicide risk factor. Screening for CTE in all deaths by suicide is probably impractical, but our finding suggests it should be undertaken if a history of repetitive head injury is known or suspected.
Ascertainment bias for abnormal neuropathology was inevitable in our study; brain donations to the ASBB were motivated by clinical diagnoses or the concerns of family members. We identified some form of neurodegeneration in all but one donor brain, and it is remarkable that CTE was found in more than half of these cases; moreover, in half of the donor brains with CTE, it was the sole neurodegenerative pathology.
In this first ASBB case series, a snapshot of neurodegeneration in Australian people who participate in contact sports, CTE was the most frequent neuropathology. Our findings should encourage clinicians and policymakers to develop measures that further mitigate the risk of sport‐related repetitive head injury.
Box 1 – Representative chronic traumatic encephalopathy lesions. A. Low power (magnification: 4×), B. high power (magnification: 40×) images*
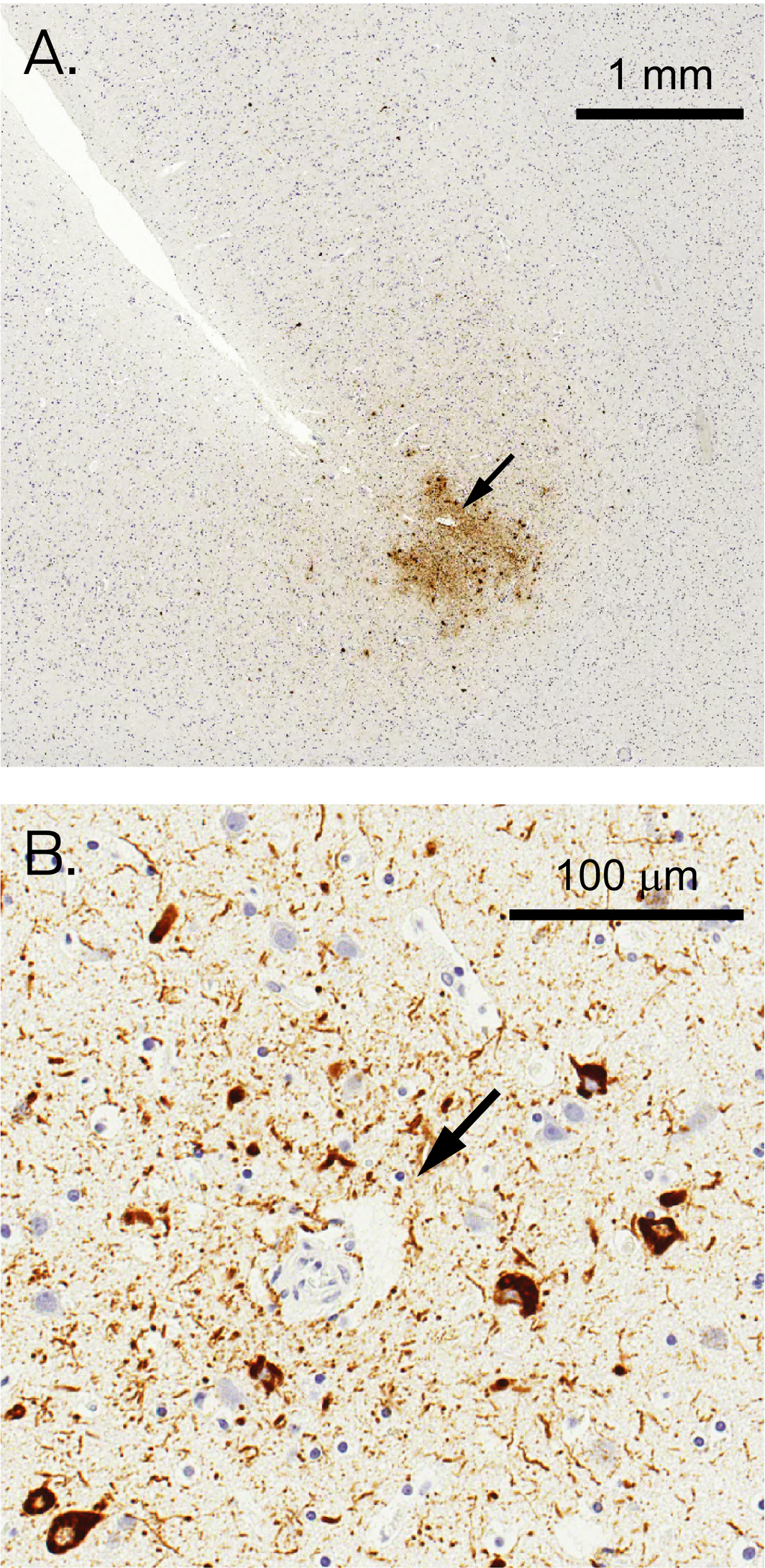
* Visualised by diaminobenzidine immunohistochemistry with the AT8 hyperphosphorylated tau (p‐tau) monoclonal antibody (Thermo Fisher) on a Leica BOND‐MAX autostainer; images captured with a Leica Aperio AT2 digital microscope. Brown staining indicates p‐tau, blue staining indicates cell nuclei stained with haematoxylin; blood vessels are indicated by arrows. A. p‐Tau accumulation is evident in both neurons and astrocytes in the depth of a cortical sulcus in the frontal cortex of a man in his early fifties who had played amateur rugby union for ten years. B. The perivascular accumulation of p‐tau is largely restricted to neurons in the frontal cortex of a man in his early thirties who had played amateur and semi‐professional rugby league for 13 years.
Box 2 – Australian Sports Brain Bank donor characteristics, by presence of chronic traumatic encephalopathy
|
Characteristic |
Chronic traumatic encephalopathy |
||||||||||||||
|
Present |
Not present |
||||||||||||||
|
|
|||||||||||||||
|
Number of donors |
12 |
9 |
|||||||||||||
|
Age at death (years), mean, (SD) |
48 (19) |
75 (19) |
|||||||||||||
|
Sex |
|
|
|||||||||||||
|
Men |
12 |
7 |
|||||||||||||
|
Women |
0 |
2 |
|||||||||||||
|
Sporting history |
|
|
|||||||||||||
|
Australian rules football |
6 |
2 |
|||||||||||||
|
Rugby union/league |
5 |
4 |
|||||||||||||
|
Other* |
1 |
3 |
|||||||||||||
|
Active playing period (years), mean (SD) |
15 (5) |
16 (10) |
|||||||||||||
|
Sporting level |
|
|
|||||||||||||
|
Professional |
8 |
3 |
|||||||||||||
|
Amateur/representative |
4 |
6 |
|||||||||||||
|
Chronic traumatic encephalopathy stage5 |
|
|
|||||||||||||
|
Low |
10 |
— |
|||||||||||||
|
High |
2 |
— |
|||||||||||||
|
Other neuropathology |
|
|
|||||||||||||
|
None |
6 |
1 |
|||||||||||||
|
Alzheimer disease |
3 |
6 |
|||||||||||||
|
Age‐related tau astrogliopathy |
3 |
5 |
|||||||||||||
|
Cerebrovascular pathology |
4 |
6 |
|||||||||||||
|
Other† |
1 |
5 |
|||||||||||||
|
Cause of death |
|
|
|||||||||||||
|
Suicide |
6 |
1 |
|||||||||||||
|
Other |
6 |
8 |
|||||||||||||
|
|
|||||||||||||||
|
SD = standard deviation. * Boxing, football (soccer), basketball, or equestrian sport. † Frontotemporal dementia, Lewy body disease, or limbic‐predominant age‐related TAR DNA‐binding protein‐43 encephalopathy. |
|||||||||||||||
Received 12 August 2021, accepted 21 December 2021
- 1. McKee AC. The neuropathology of chronic traumatic encephalopathy: the status of the literature. Semin Neurol 2020; 40: 359–369.
- 2. Mez J, Daneshvar DH, Kiernan PT, et al. Clinicopathological evaluation of chronic traumatic encephalopathy in players of American football. JAMA 2017; 318: 360–370.
- 3. Mez J, Alosco ML, Daneshvar DH, et al. Validity of the 2014 traumatic encephalopathy syndrome criteria for CTE pathology. Alzheimers Dement 2021; 17: 1–16.
- 4. Pearce AJ, Sy J, Lee M, et al. Chronic traumatic encephalopathy in a former Australian rules football player diagnosed with Alzheimer’s disease. Acta Neuropathol Commun 2020; 8: 23.
- 5. Bieniek KF, Cairns NJ, Crary JF, et al. The second NINDS/NIBIB consensus meeting to define neuropathological criteria for the diagnosis of chronic traumatic encephalopathy. J Neuropathol Exp Neurol 2021; 80: 210–219.
The Australian Sports Brain Bank is supported by the Sydney Local Health District (LHD), and received seed funding from the Concussion Legacy Foundation (United States), the Northern Sydney LHD, and the StopConcussions Foundation. We are grateful to our brain donors and their families, without whom this report would not be possible.
No relevant disclosures.