





Medical education
Lessons from practice
Volume 216 - Issue 1
Infective discitis with concurrent calcific discitis masquerading as renal colic
Authors: Roland Z White, Hemant Vanmali and Matthew Sampson
Med J Aust 2022; 216 (1): 17-19. || doi: 10.5694/mja2.51363
Published online: 17 January 2022
Published online: 17 January 2022
A 76-year-old man with a history of ureteric nephrolithiasis presented with dysuria and sharp, severe right flank pain with radiation to the inguinal region
Clinical record
A 76‐year‐old man with a history of ureteric nephrolithiasis presented with dysuria and sharp, severe right flank pain with radiation to the inguinal region. He was febrile to a temperature of 39°C, tender over the right costovertebral angle, lumbar spine, right iliac fossa, and suprapubic regions with no focal neurology. Clinically, he was diagnosed with ureteric nephrolithiasis and sent for imaging. Computed tomography (CT) scan of the abdomen and pelvis revealed non‐specific right retroperitoneal inflammation (Box 1) associated with calcific material at the anterolateral L4–L5 disc space (Box 2, A and B) without evidence of appendicitis or ureteric stones. Immediate magnetic resonance imaging (MRI) scan of the spine demonstrated L4/L5 calcific material extruded anterolaterally and paraspinal inflammation (Box 3, A and B), with a diagnosis of acute calcific discitis and the caveat that this is exceedingly rare and infection is a differential. Biochemistry revealed creatinine level 138 µmol/L (reference interval [RI], 60–110 µmol/L), C‐reactive protein 342.3 mg/L (RI, 0–8.0 mg/L), white cell count 13.8 × 109/L (RI, 4–11 × 109/L), and unremarkable urine microscopy, culture and sensitivity analysis. On day 2, blood cultures returned positive for methicillin‐sensitive Staphylococcus aureus (MSSA), creatinine was 338 µmol/L and C‐reactive protein was 432 mg/L. He was managed with intravenous cephazolin 500 mg every 12 hours, the dose was adjusted for acute renal failure, presumed secondary to MSSA bacteraemia. Echocardiogram was normal, and nuclear medicine renal scan did not reveal cortical infarction. Four days after the initial presentation, the patient developed new L4/L5 hyperesthesia and MRI scan of the spine demonstrated severe canal stenosis secondary to an epidural abscess (Box 4, A and B). He underwent posterior decompression with tissue cultures positive for S. aureus. The renal failure resolved with source control for sepsis. The patient completed 12 weeks of antibiotic therapy in total; 6 weeks of intravenous cephazolin, and 6 weeks of oral clindamycin 450 mg three times a day. Six‐month follow‐up revealed the patient had no recurrence or neurological deficit.
Discussion
Symptomatic calcific discitis is a rare condition in adults. Disc calcifications are usually asymptomatic; however, if they extrude into surrounding tissues, they induce acute pain and inflammation. Symptomatic calcific discitis is clinically indistinguishable from infective discitis, with both conditions manifesting fever and elevated inflammatory markers.1,2 In patients with symptomatic calcific discitis, they often spontaneously improve within a week. Calcific discitis has a predilection for the mid‐lower thoracic region, rarely afflicting the lumbar spine;1 hence, a degree of suspicion should arise in the clinician when calcific discitis is diagnosed in the lumbar region.
This case was initially radiologically diagnosed as calcific discitis due to the calcified nucleus pulposus with anteriorly extruded calcific material (Box 2, A and B; Box 3, A and B) and no evidence of epidural abscess formation. Differential diagnoses include infective discitis, neoplasia, metastatic deposits, tuberculosis (Potts disease), and synovitis, acne, pustulosis, hyperostosis, osteitis (SAPHO) syndrome. Before evidence of radiographic calcification, the only clue of calcific discitis on MRI may be disc swelling associated with a diffuse and reactive oedema of the vertebral end plates.1 Contrast enhancement of the vertebral body may occur in calcific discitis if there is an associated vertebral body herniation of calcific material.2 However, an infective process may additionally demonstrate diffuse oedema and contrast enhancement of vertebral bodies. It is suggested that calcification of the nucleus pulposus on CT is crucial to the diagnosis of calcific discitis;1,2 however, in this case, it allayed suspicion of an infective process. This case suggests extrusion of calcific material may coincide with an infective discitis. The common route of disc infection is from the pelvic organs via Batson venous complex, with the most common microbe identified as S. aureus. Presumably, in this case, a primary infectious discitis provoked an anterolateral annulus fibrosis rupture and sepsis, allowing incidental calcium extrusion from a pre‐existing calcified disc. Calcium extrusion has not been associated with sepsis in the literature.3,4 To our knowledge, this is the first case to concomitantly involve sepsis and bacteraemia with extruded calcium from the disc. Therefore, extruded calcific material from an intervertebral disc should not exclude the presence of an infective process. With respect to the initial presentation, we suggest the anterolaterally extruded calcific material incited retroperitoneal inflammation, irritating the right ureter, mimicking renal colic.
This case of infective discitis superimposed on a calcific discitis is diagnostically difficult. Calcific discitis may mimic an infective process but does not exclude their concurrent presence, and we propose calcific discitis should be a diagnosis of exclusion. In practice, it is common for the radiological diagnosis, at least initially, to become the clinical diagnosis; however, this article discourages this heuristic decision making and encourages physicians to encompass the history, physical examination, biochemistry and radiology in making a diagnosis.
Lessons from practice
- A patient with radiating flank pain and a history of nephrolithiasis should not be assumed to be having renal colic, and differential diagnoses should include pyelonephritis, perinephric abscess, discitis, aortic aneurysm, renal infarction, appendicitis, diverticulitis and musculoskeletal pain.
- Calcific discitis is a sinister condition without pathognomonic features and should be a diagnosis of exclusion once infective discitis has been confidently excluded.
- Calcific discitis is more common in children, and usually affects thoracic and cervical intervertebral discs.
- Radiology is only a piece of the diagnostic puzzle, and findings should be interpreted in the context of clinical and biochemical findings.
Box 1 – Axial computed tomography scan of the abdomen and pelvis post‐contrast*
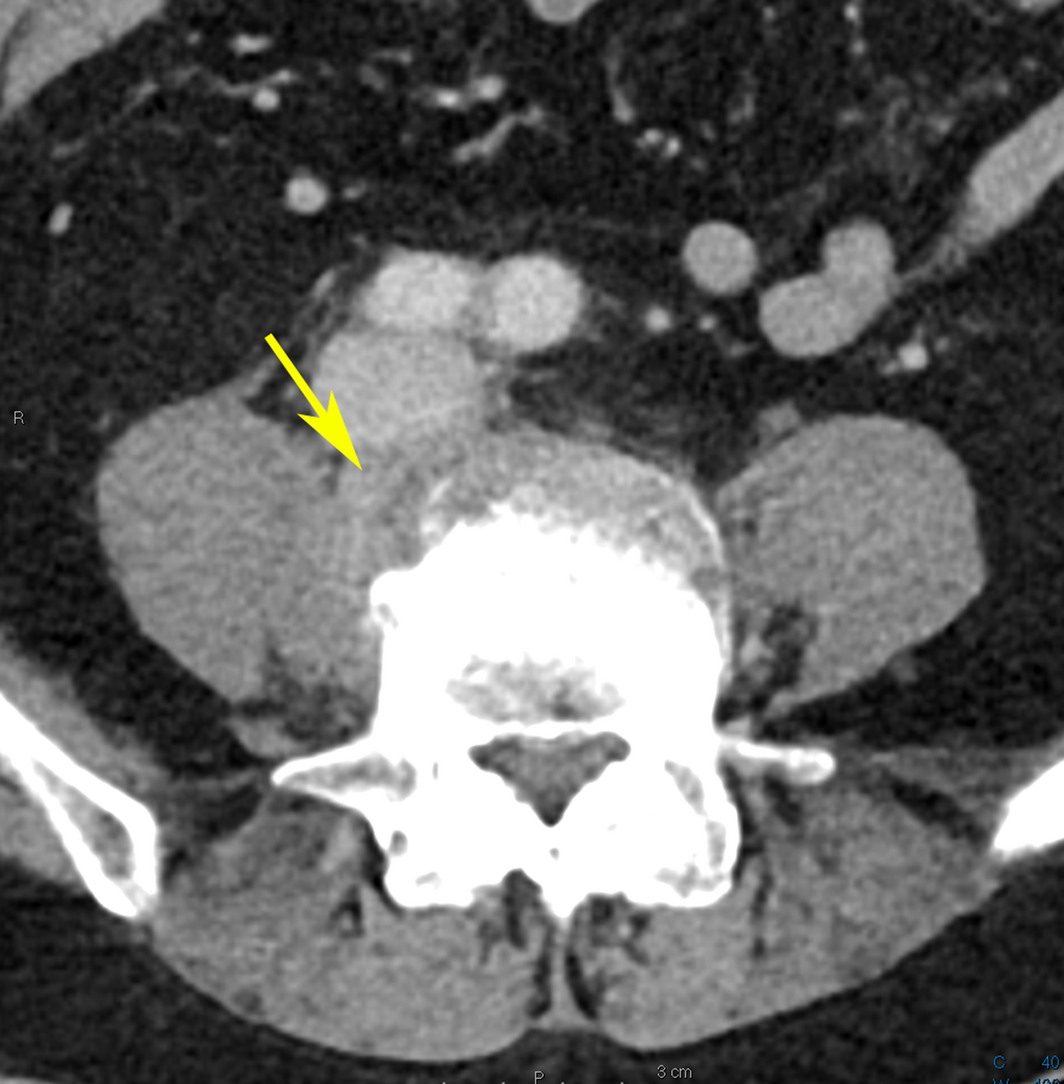
* Retroperitoneal inflammation (arrow) identified at the anterolateral L4/L5 level.
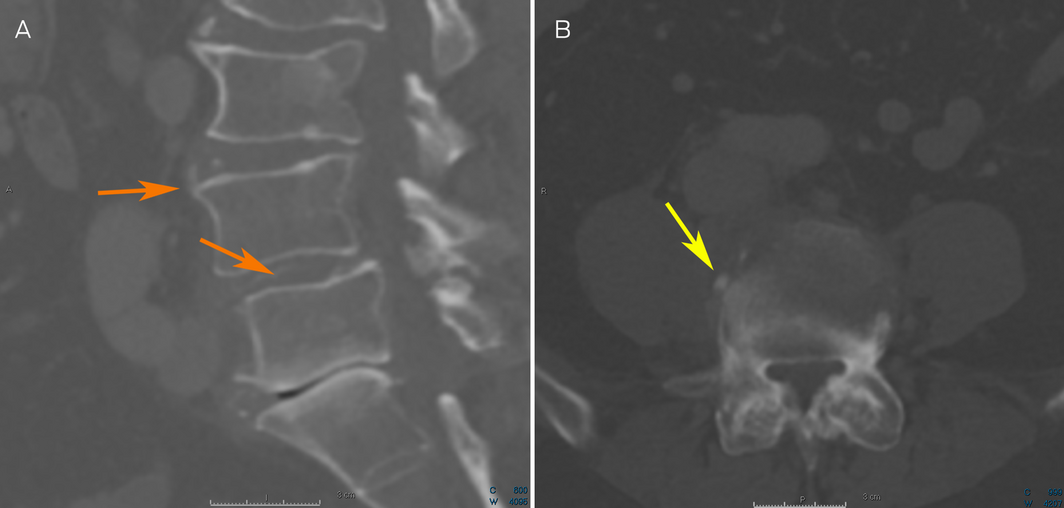
Box 2 – Reconstructed sagittal computed tomography (CT) post‐contrast scan, with calcification demonstrated at the L3/L4 and L4/L5 disc space (orange arrows) (A). Axial CT post‐contrast scan, with calcification anterolaterally at the L4/L5 disc space (yellow arrow) (B)
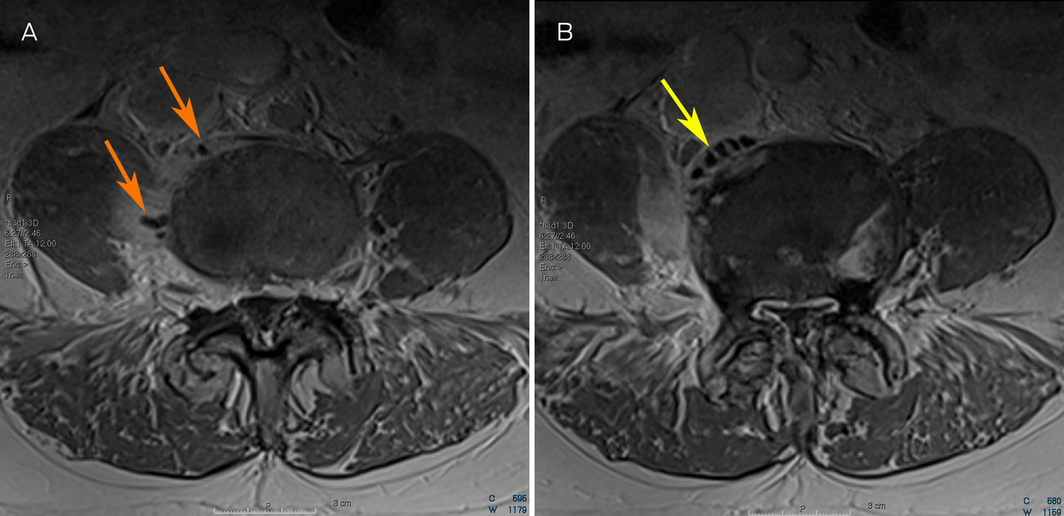
Box 3 – Post‐contrast axial T1 magnetic resonance imaging (MRI) scan of the spine showing acute discitis of the L4/L5 level with extrusion of low signal intensity (dark) calcific material (panel A, orange arrows; panel B, yellow arrow) into the paraspinal musculature with adjacent inflammatory response
Box 4 – T2 axial (A) and T2 sagittal (B) magnetic resonance imaging (MRI) scan of the spine* showing severe canal stenosis at L4/L5 level secondary to epidural abscess (arrows) causing effacement of the thecal sac and compression of the cauda equina
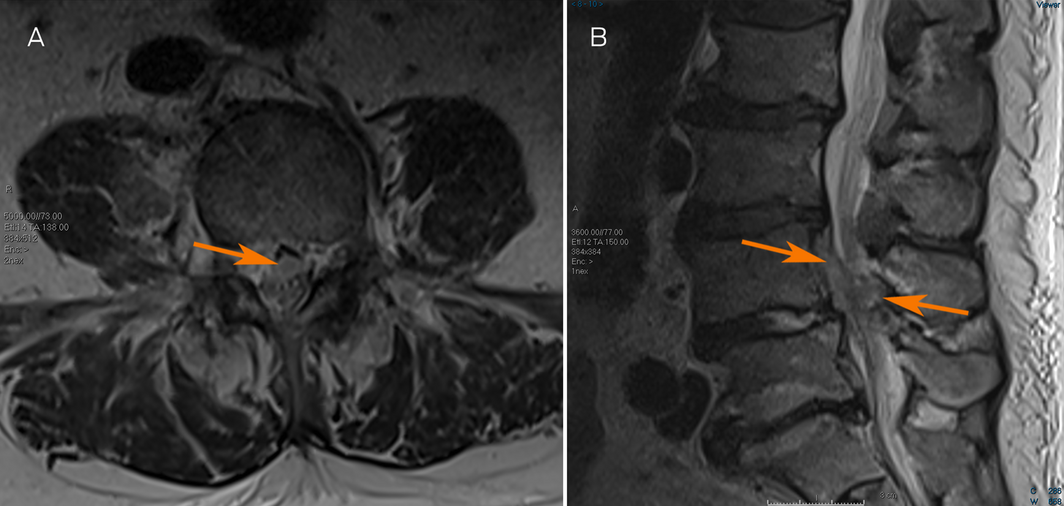
* Contrast could not be administered due to renal failure.
Competing interests
No relevant disclosures.
References
- Choueiri M, Eymard F, Guignard S, et al. Acute symptomatic calcific discitis mimicking a septic spondylodiscitis. Case Rep Rheumatol 2020; 2020: 5454197.
- Shah A, Botchu R, Grainger MF, et al. Acute symptomatic calcific discitis in adults: a case report and review of literature. Skeletal Radiol 2015; 44: 1819–1824.
- Sadek AR, Dare C, McGillion S, et al. Lumbar intravertebral disc herniation secondary to idiopathic calcific discitis. Br J Neurosurg 2019; 33: 586–590.
- Nogueira‐Barbosa MH, da Silva Herrero CF, Pasqualini W, Defino HL. Calcific discitis in an adult patient with intravertebral migration and spontaneous remission. Skeletal Radiol 2013; 42: 1161–1164.
Provenance: Not commissioned; externally peer reviewed.