





Medical education
Lessons from practice
Volume 215 - Issue 2
Paradoxical embolism through patent foramen ovale as a cause of myocardial infarction
Authors: Naim Mridha, Eloise Ward, Samual Hayman, Arun Dahiya and Sandhir Prasad
Med J Aust 2021; 215 (2): 68-69.e1. || doi: 10.5694/mja2.51140
Published online: 19 July 2021
Published online: 19 July 2021
A 42-year-old man presented with acute onset substernal chest pain
Clinical record
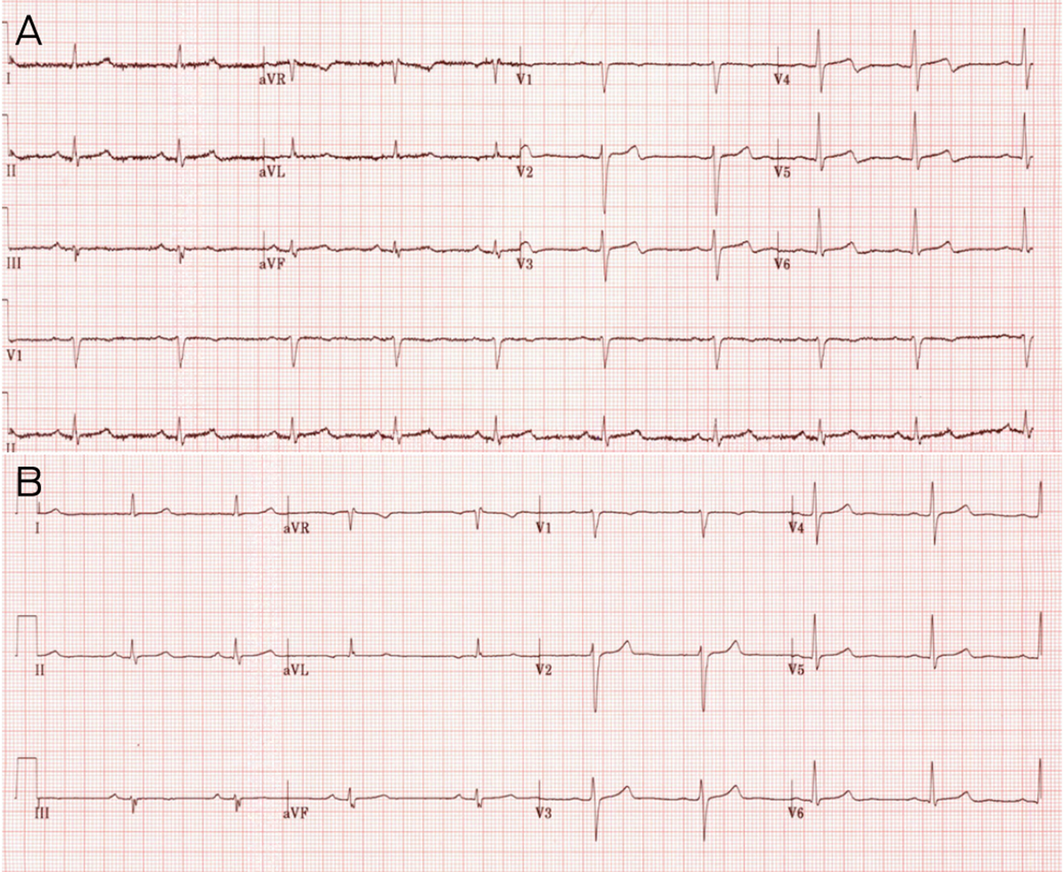
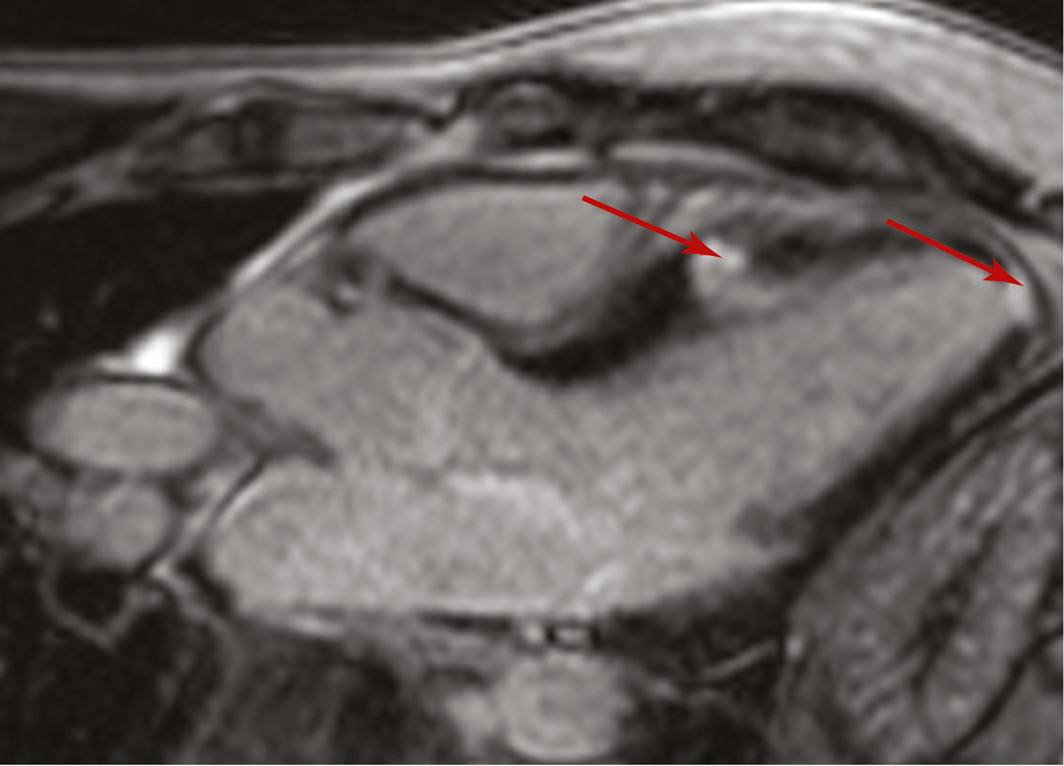
A 42‐year‐old man presented with acute onset substernal chest pain. His only cardiac risk factor was mild, medicated dyslipidaemia and he was a lifelong non‐smoker. He had a healthy body mass index and exercised regularly. There was no history of previous thromboembolic events or known haematological disease. On arrival to the emergency department, he was haemodynamically stable. Electrocardiogram initially showed sinus rhythm with biphasic anterior lead T wave inversion that resolved before angiogram (Box 1). Cardiac high sensitivity troponins were positive, peaking at 2479 ng/L (reference range, < 20 ng/L), while the remaining laboratory tests, including white cell count and inflammatory markers, were unremarkable. Telemetry throughout admission did not identify arrhythmia. Coronary angiography to investigate the source of the troponin leak showed normal coronary arteries (Box 2). Subsequent cardiac magnetic resonance imaging scan revealed localised hypokinesia of mid‐anteroseptum and apical cap with non‐contiguous subendocardial late gadolinium enhancement in mid‐septum and distal cap (Box 3), raising the possibility of embolic events. Transthoracic echocardiogram demonstrated regional wall motion abnormalities with mid‐anteroseptal and apical hypokinesis, with an early positive agitated saline bubble study and evidence of right‐to‐left shunt suspicious of patent foramen ovale (PFO). Subsequent transoesophageal echocardiogram confirmed moderate sized PFO with shunt present both at rest and after Valsalva manoeuvre. Ultrasound of the lower limbs showed superficial saphenous vein thromboembolism (unprovoked) but no deep vein thrombosis. Remaining investigations, including a thrombophilia screen, were unremarkable. After discussion with the patient, he was commenced on anticoagulation for 2 months until he underwent successful percutaneous PFO closure, at which point he was transitioned to antiplatelet therapy.
Discussion
A PFO is required during fetal development to facilitate the flow of oxygenated blood from the right to the left atrium. This can persist into adulthood in 20–34% of the population, with higher prevalence rates reported among people with cryptogenic stroke.1 Since paradoxical embolism was first described by Cohnheim in 1877,2 ischaemic stroke due to paradoxical embolism has become the most recognised potential clinical manifestation of PFO.1 Coronary artery embolism is a less recognised complication, with limited case reports and pathological series suggesting that this represents 5–10% of all paradoxical emboli.3,4
Myocardial infarction secondary to paradoxical coronary artery embolism demands a high index of clinical suspicion, although the association of embolic events can be difficult to prove. The diagnosis should be presumed in patients who have low risk for acute coronary syndrome, do not have a left atrial thrombus and demonstrate a venoarterial shunt on echocardiography.5 Evidence of peripheral venous thromboembolism may be an additional clue; our patient had no history of prior thromboembolic event and he had no risk factors. While identifying an embolus during angiography would support this diagnosis (often requiring manual thrombectomy), a normal coronary angiogram should not preclude clinical suspicion, particularly if patients have received anticoagulation before the procedure as part of their acute coronary syndrome management. Differential diagnoses of chest pain and troponin leak in the absence of significant angiographic atherosclerotic coronary artery disease includes plaque erosion, myocarditis (including myopericarditis), spontaneous coronary artery dissection and myocardial infarction with non‐obstructive coronary arteries (MINOCA). Despite the challenges, recognising PFO as a mechanism of acute myocardial injury in young patients is important to prevent further embolic phenomena with the potential to cause severe disability or death.
Recent randomised controlled trials have established that PFO closure reduces the risk of recurrent stroke compared with medical therapy alone in patients with cryptogenic stroke, particularly in younger patients.6 Evidence is limited on whether these principles can be extrapolated to patients presenting with suspected coronary artery embolism. However, we advocate that initial anticoagulation and PFO closure should be recommended in appropriately selected patients if other aetiologies of myocardial infarction are excluded and a high index of clinical suspicion remains. Further investigation for sources of emboli, including deep vein thrombosis and thrombophilia screening, may assist in further risk stratification. In the longer term, prospective data are required to consolidate management, but performing a randomised controlled trial for a rare condition like this is difficult.
Lessons from practice
- Paradoxical embolism should be considered in the differential diagnosis of patients presenting with acute coronary syndrome who are identified to have patent foramen ovale (PFO).
- Features supporting paradoxical embolism include younger patients, absence of vascular risk factors, absence of left atrial thrombus, angiographically normal coronary arteries, or demonstration of thrombotic occlusion of a coronary artery without significant coronary atheroma.
- Evidence supporting PFO closure in addition to anticoagulation in patients with cryptogenic stroke may also be relevant in the management of patients with embolic infarction; however, longer term, randomised and prospective data are required to consolidate management.

Competing interests
No relevant disclosures.
References
- Giblett JP, Abdul‐Samad O, Shapiro LM, et al. Patent foramen closure in 2019. Interv Cardiol 2019; 14: 34–41.
- Lippmann H, Rafferty T. Patent foramen ovale and paradoxical embolization: a historical perspective. Yale J Biol Med 1993; 66: 11–17.
- Hakim FA, Kransdorf EP, Abudiab MM, Sweeney JP. Paradoxical coronary artery embolism — a rare cause of myocardial infarction. Heart Views 2014; 15: 124–126.
- Namasivayam M, Spina R, Bobillo L, et al. Acute myocardial infarction due to paradoxical embolism. Int J Cardiol 2016; 209: 190–191.
- Johnson BI. Paradoxical embolism. J Clin Pathol 1951; 4: 316–332.
- Søndergaard L, Kasner SE, Rhodes JF, et al. Patent foramen ovale closure or antiplatelet therapy for cryptogenic stroke. N Engl J Med 2017; 377: 1033–1042.
Provenance: Not commissioned; externally peer reviewed.